
Abstract
Study Design
Case report and review of the literature.
Objectives
Case report of a traumatic dissection of all major brain-supplying arteries resulting from a horseback-riding accident. Overview of the literature on diagnostic and therapeutic recommendations.
Methods
Case presentation. For the discussion, handpicked articles and PubMed database research with the keywords “dissection,” “vertebral artery,” “spine trauma,” “computed tomography,” “magnetic resonance imaging,” and “angiography” were used.
Results
Despite high-energy induced acute lesion of all four cervical arteries, this 45-year-old patient did not demonstrate signs of microemboli nor suffer from stroke.
Conclusion
In case of high-energy trauma of the head and/or the neck, emergency physicians must consider traumatic cervical artery dissection (TCAD). Thus, emergency care algorithms should routinely include computed tomography angiography and magnetic resonance imaging. Although the incidence of TCAD-induced stroke is low, antiplatelet therapy is recommended in the presence of TCAD.
Keywords
Introduction
Traumatic cervical artery dissection (TCAD) represents a rare but under certain circumstances life-threatening injury. Due to improvements in the diagnostic algorithms in the emergency room, blunt TCAD has increasingly been recognized. The most common injury mechanisms are combined movements of distraction and extension, distraction and flexion, and lateral flexion. The formation of a thrombus at the site of the intimal lesion can lead to an ischemic neurologic deficit if cerebral blood flow is compromised or embolization to the brain occurs. Even injuries of the vertebral arteries alone without any lesion of the carotid arteries can lead to symptomatic cerebral lesions. Interestingly, there seems to be no correlation between the size of the occlusion and the neurologic outcome. 1
Recent studies have shown TCAD in 1.0 to 3.7% of all blunt trauma admissions. 2 , 3 In patients at risk for TCAD, aggressive screening has revealed an incidence of 13 to 39% of those serious vascular injuries. 2 , 4 Neurologic deficits were present in more than a quarter of patients suffering from TCAD. 4 Cases of traumatic quadruple lesions of the cervical arteries have exhibited pronounced neurologic deficits. 5 , 6 The following case report describes TCAD of all four cervical arteries after a high-energy horse-riding injury of a woman with no resulting neurologic deficit.
Case Report
A 45-year-old woman was admitted to the emergency department after falling off a galloping horse without wearing a helmet. The patient was treated according to Advanced Trauma Life Support guidelines. At a Glasgow Coma Scale of 15 points, the patient initially complained of right-sided chest pain and exhibited progressive respiratory insufficiency. After successful treatment of hematothorax with a thoracic drain, the patient was intubated and put under controlled ventilation. Diagnostics revealed right-sided pulmonary contusion, fracture of the sixth through tenth ribs, and fracture of the scapula as well as a compression fracture of the second lumbar vertebra, accompanied by extensive soft tissue contusions of the right side of the neck and shoulder. No bony or discoligamentary injury of the cervical spine was found.
Following extubation and neurologic examination, the patient demonstrated paresis of abduction and anteversion of the right arm that was clinically allocated to an upper brachial plexus injury. Magnetic resonance imaging (MRI) of the right shoulder revealed a diffuse accumulation of fluid around the upper right brachial plexus. A secondary finding was an elongated dissection of both vertebral arteries in the V2 segment (Fig. 1). Immediate MRI examination of head and neck showed no signs of thromboembolic lesions and cerebral ischemia. However, imaging did show stenosis due to intimal flaps of both carotid arteries between the carotid bifurcation and the base of the skull without signs of thrombosis (Fig. 1). The diagnosis of quadruple cervical arterial injury was confirmed by computed tomography angiography (CTA; Fig. 2). The patient was initially treated with heparin. After 1 week, anticoagulation with heparin was stopped and antiplatelet therapy was initiated.

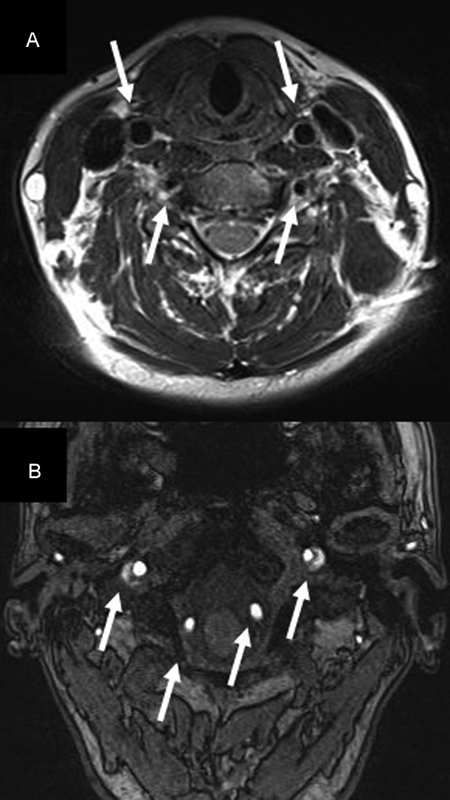
Images from 1.5-T Avanto (Siemens, Munich, Germany) magnetic resonance imaging (MRI). (A) Axial T2-weighted MRI of the neck. Flow voids in both common carotid arteries (arrows), indicating arteries are perfused normally. Thin flow voids in both vertebral arteries (VA), indicating reduction of arterial lumen (open arrows). (B) Axial T2-weighted MRI of the base of the skull. Flow voids in both VAs (open arrows) but only partial flow voids in both internal carotid arteries (arrows), indicating reduced perfusion.
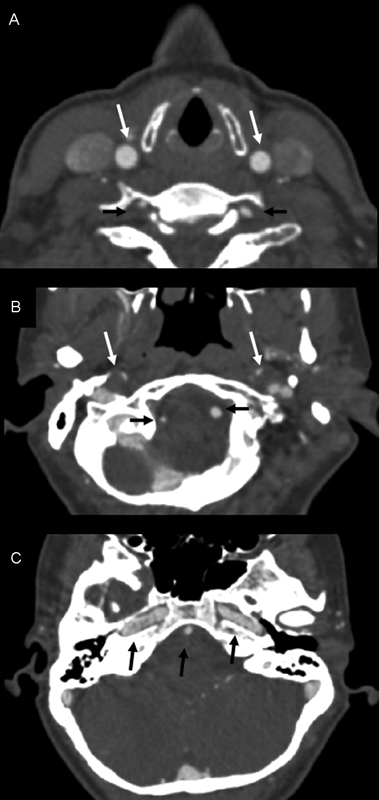
Computed tomography angiography on 16-Slice Sensation (Siemens, Munich, Germany). (A) Normally perfused common carotid arteries (white arrows) but filiform-perfused vertebral arteries (VA) (black arrows) at the level of the larynx. (B) Filiform-perfused internal carotid arteries (ICA) and normally perfused VAs at the base of the skull. (C) Regular perfusion of basilar artery and both ICAs at level of carotid canal.
At the follow-up examination after 3 months, paresis of the right shoulder joint had completely resolved. Clinical examination did not reveal any central and/or peripheral neurologic deficit. MRI after 3 months showed that all arterial lesions had regressed in size (Fig. 3).
Images from 3-T TrioTim (Siemens, Munich, Germany). (A) Both common carotid arteries and vertebral arteries (VA) open with residual reduction of lumen of right VA. (B) At the base of the skull, all four arteries are perfused; however, both internal carotid arteries still show reduced lumen.
Discussion
As far as we know, there has to date been no other case of an asymptomatic dissection of all four brain-supplying arteries originating from high-energy trauma to the neck. This case is highly interesting due to three facts: (1) asymptomatic TCAD may be easily missed. (2) CTA should be routinely performed in the emergency diagnostic procedures according to the patient's history. (3) Anticoagulation treatment may still be in discussion.
Of all diagnostic modalities, digital subtraction angiography (DSA) reaches the highest level of sensitivity and specificity in the detection of vascular lesions and represents the gold standard. The diagnostic accuracy of CTA varies between institutions depending on the quality of the CT as well as the quality of image interpretation by the radiologist. 7 In a recent prospective study, only 68 of 112 patients with CTA results suggestive of TCAD were confirmed by DSA. 8 Meta-analysis of the diagnostic accuracy of CTA and DSA in the detection of traumatic cervical vascular injuries showed that sensitivity of CTA (66%) was inferior to DSA, yet CTA specificity (97%) was high. It was suggested that patients with cervical artery injury detected by CTA, who suffered accompanying injuries indicating high risk of TCAD, may receive treatment without confirmation of diagnosis by DSA. 7 In clinical practice, CTA is faster, less prone to complications, and more useful for diagnosing secondary injuries. 9 In the face of these advantages on top of the increasing sensitivity of modern CT instruments, CTA has become more and more important for the diagnosis of traumatic arterial dissections. 10 With regard to our trauma protocol in the emergency room, CTA has been included into the secondary trauma survey in the presence of a patient history indicating high risk of TCAD. In contrast to DSA, not only does MRI angiography allow screening of TCAD, but it is also capable of detecting thromboembolic cerebral lesions. 11 In addition, many patients with multiple injuries do not tolerate further invasive and sometimes long-lasting diagnostic procedures such as DSA. Because diagnosis of quadruple arterial dissection was positive in both CTA and MRI angiography, we did not perform DSA as a third diagnostic procedure after risk-benefit evaluation.
In our case, surgical therapy of the vascular injuries was never considered due to the fact that neurologic deficit, signs of acute hemorrhage, or ischemia was not detected. In fact, TCAD may be more benign than previously thought and therefore only requires aggressive surgical treatment in very rare cases. 12 Finally, any surgical procedure to be performed in a patient with multiple injuries has to be carefully evaluated. This latter point clearly makes the difference between a patient with TCAD and a patient suffering from chronic stenosis of the carotid arteries.
Most authors agree that some form of antithrombotic therapy is necessary after diagnosis of those injuries, although the overall incidence of ischemic stroke among patients with TCAD is low. 8 However, the type of antithrombotic therapy is controversial. The use of heparin is more popular than antiplatelet therapy, but the risk of hemorrhagic complications is high. 2 , 13 , 14 , 15 , 16 Nevertheless, we decided to use heparin in our patient with multiple injuries because of its capability to maintain continuous and immediate control of anticoagulation. After 1 week, during which the patient remained asymptomatic, her vital functions had stabilized, and no surgical procedures had been necessary, the treatment was changed to antiplatelet therapy. The latter have been found to be equivalent or even superior to heparin therapy with regard to thromboembolic complications, but with a more favorable profile of potential side effects. 17 , 18 , 19
This is in agreement with a recent study by Cothren and coworkers. 17 The authors looked at the therapeutic options after blunt TCAD and clearly demonstrated that the type of treatment, heparin versus antiplatelet agents, does not appear to significantly affect either the risk of stroke or the injury healing rates. 17 We conclude from the experience with our case and the recent literature that anticoagulation in the presence of TCAD is necessary but may be different from patients with chronic atherosclerosis. We recommend heparin at the beginning because of its excellent capability of dose and effect regulation. Long term, antiplatelet agents seem to be the therapy of choice. 20
Disclosures
None