
Abstract
Study Design
Case report and review of the literature.
Objective
To present an unusual case of conus medullaris ependymal cyst.
Methods
This is a case of a 41-year-old woman with a diagnosis of ependymal cyst who presented with a history of shock-like pain to the lower limbs.
Results
The patient underwent a successful cyst decompression.
Conclusion
A few cases have been reported in the literature. Including this case, there are a total of eight cases of ependymal cyst in the conocaudal segment reported.
Keywords
Introduction and Case Description
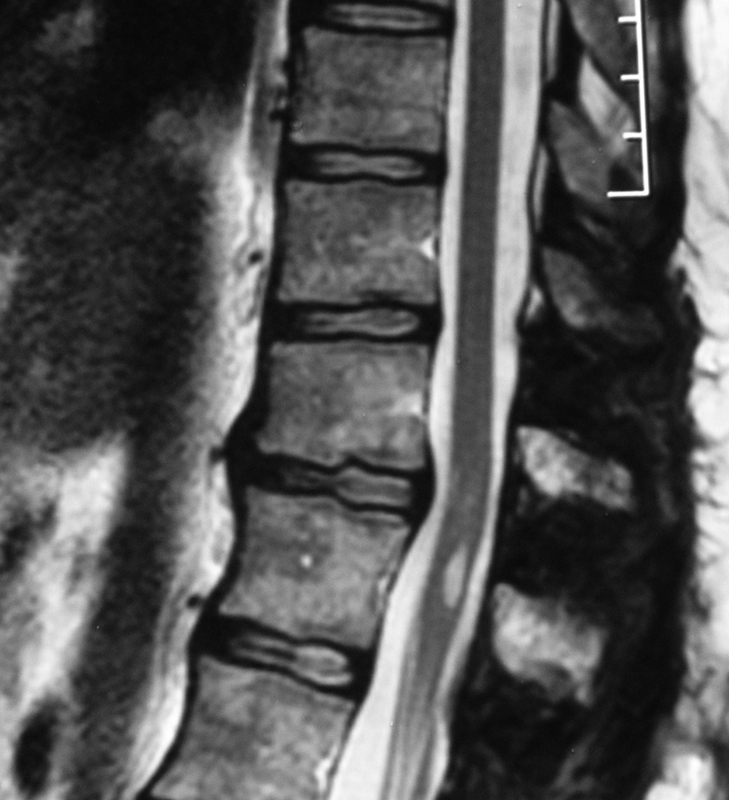
A 41-year-old woman with a 2-month history of shock-like pain radiating down the spine to the lower limbs with a radicular pattern was admitted into our department. Neurologically, muscle strength was normal, deep tendon reflexes were diminished without pathologic reflexes, and there were no sensory abnormalities. Perineal examination revealed a slight sacral hypoesthesia with no motor deficits. Spinal X-ray revealed no distinct abnormalities. Magnetic resonance imaging (MRI) revealed a circumscribed intramedullary lesion at the level of T11–T12 that appeared isointense compared with the cerebrospinal fluid (CSF) on both T1-weighted and T2-weighted MRI (Fig. 1). The clinicoradiologic diagnosis was ependymal cyst. The patient was operated on in December 2011. A laminoplasty of T11–T12 was performed, which revealed an expanded spinal cord at this level (Fig. 2). We proceeded with a splitting cord approach through the midline, which allowed us to enter the cyst right at its lower portion where we could see the nerve roots split by the lesion. We avoided going around the cyst, and we do not recommend this approach as the risk of neurologic deficits increases. The cyst was opened and clear CSF-like fluid was obtained, resulting in immediate collapse of the cyst (Fig. 3). The cyst wall was partially removed to obtain a diagnosis, and adequate communication between the cyst and the subarachnoid space was ensured (Fig. 4). Pathology showed cuboidal epithelium without a basement membrane, resting on fibrous tissue (Fig. 5). Postoperatively, the patient noted immediate improvement with absence of the shocking pain and resolution of the perineal hypoesthesia. She has been followed for almost 2 years and no recurrence of symptoms has been noted. Her latest MRI still shows a collapsed cyst (Fig. 6).
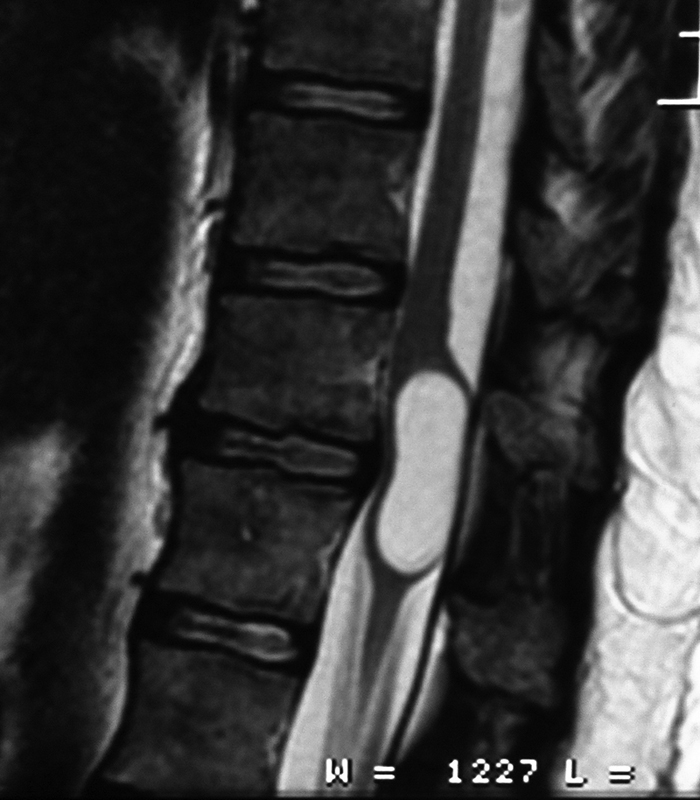
Sagittal magnetic resonance imaging (MRI) revealing a circumscribed intramedullary lesion at the level of T11–T12 that appears isointense compared with the cerebrospinal fluid on T2-weighted MRI.
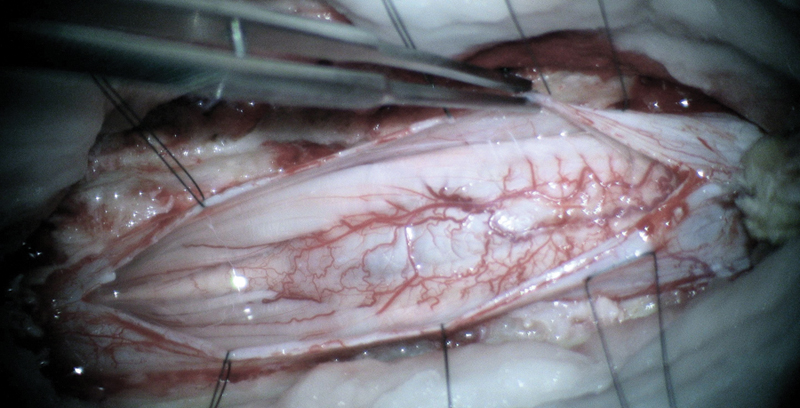
Laminoplasty of T11–T12 revealing an expanded spinal cord at this level.
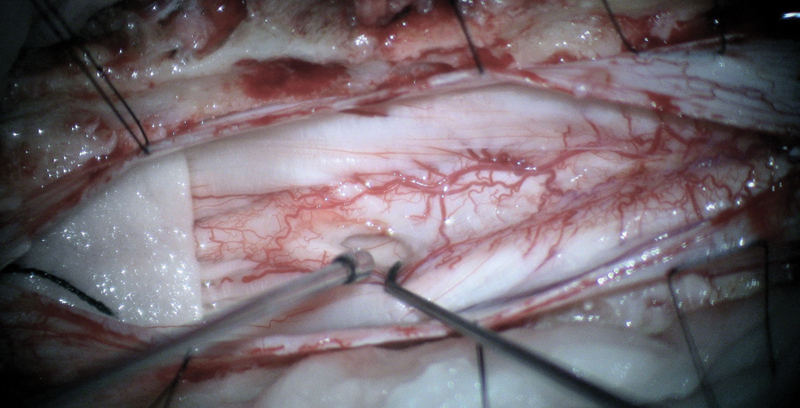
Opening of the cyst. Cerebrospinal fluid–like substance was obtained, resulting in collapse of the cyst.
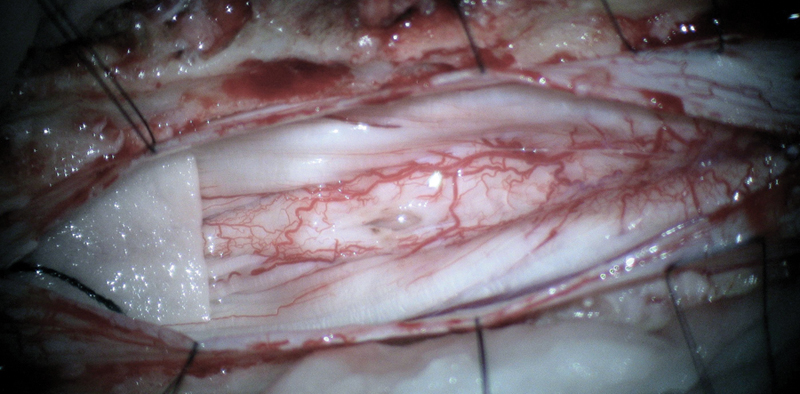
The cyst wall was partially removed. Adequate communication between the cyst and the subarachnoid space was ensured.
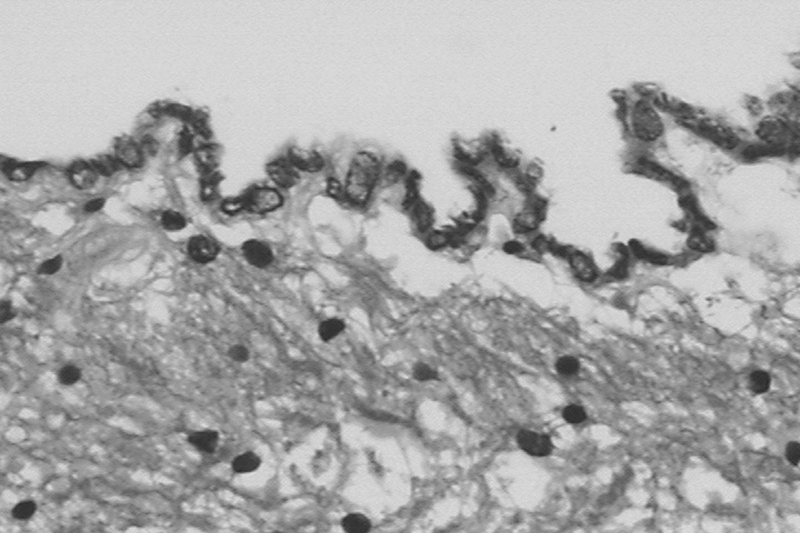
Pathology showing a cuboidal epithelium without a basement membrane, resting on fibrous tissue.
Late magnetic resonance imaging showing adequate communication between the cyst and the subarachnoid space.
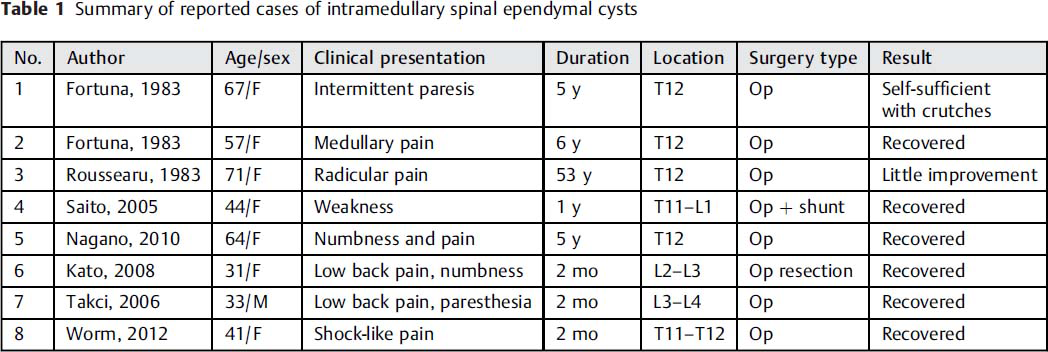
An intramedullary ependymal cyst is a rare lesion of dysembryoplastic origin, and only a few cases have been documented in the conus medullaris. Including this case, there are eight cases of ependymal cyst of the thoracolumbar region (Table 1). There have been only 22 reports of an intramedullary ependymal cyst since the first in 1938. Ependymal cysts occur more commonly in the conocaudal segment (56%) than in the cervical (22%) or thoracic (22%) spine. However, only seven ependymal cysts have been reported in the conus medullaris. 1 , 2 , 3
Summary of reported cases of intramedullary spinal ependymal cysts
Intradural spinal cysts are uncommon benign formations histologically classified as arachnoid, enterogenous, and ependymal cysts. Ependymal cysts are also called glioependymal, neuroepithelial, or choroidal epithelial cysts. Arachnoid cysts are the most common intradural spinal cysts and usually occur in the subarachnoid space but not in the intramedullary compartment. Enterogenous cysts generally occur in the anterior portion of the third ventricle and have an epidermal lining of intestinal origin. Ependymal cysts originate from evaginated cell resting on the floor plate of the neuroectoderm, which are cut off from the main mass of the neural tube in the developing embryo. The intramedullary variety might originate from islets of ependymal cells, which are frequently found near the ependymal canal. 1 , 2 , 3
There is a female preference for the cysts in the conus medullaris (only one case has been reported in a male patient). A variable clinical presentation includes paresis, radicular symptoms, and paresthesia. The pathogenesis indicates that the floor plate of the neural tube is evaginated on the ventral side and then a cyst forms later. Pathologically, ependymal cysts are lined with columnar or cuboidal epithelium with or without cilia that lack a basement membrane and rest on fibrous tissue. They usually are located in the anterior cord. The cyst does not communicate with the central canal and must be differentiated from syringomyelia and terminal ventricle. Ventriculus terminalis cysts are congenital midline conus cysts that could be related to spinal dysraphism and are more common in children. 1 , 2 , 3
Magnetic resonance is the best imaging method for evaluation of spinal cord cysts. The borders of the ependymal cyst are smooth and well defined. The cyst is also isointense with CSF on T1- and T2-weighted images without contrast enhancement. 1 , 2 , 3
Anticytokeratin antibodies CAM5.2 and AE1/AE3 are useful markers of ependymal tumors of neuroepithelial origin. Ependymal cysts are also positive for glial fibrillary acidic protein and S-100, both of which are glial markers expressed by normal ependymal epithelium, whereas enterogenous cysts express epithelial markers but no glial cell markers. 1 , 2 , 3
Conclusion
The treatment recommended is surgical decompression. Various techniques have been reported for ependymal cysts, including total resection, partial resection, biopsy, marsupialization of the cyst, and cystosubarachnoid shunt. Recurrence of this type of cyst is rare, and neurologic signs and symptoms are usually relieved by surgical decompression. 1 , 2 , 3 Nevertheless most authors recommend a surgical procedure that provides adequate decompression and communication between the cyst cavity and subarachnoid space. Total resection is not recommended.
Disclosures
None