
Abstract
Study Design
Case report and review of the literature.
Objective
To report a case of traumatic L5–S1 spondyloptosis and review the literature.
Method
A 28-year-old man presented with severe low back pain, numbness at the soles of feet, and bowel and bladder dysfunction. Two days before admission, a tree trunk fell on his back while he was seated. A two-stage posterior-anterior procedure was performed. At the first stage, posterior decompression, reduction, and fusion with instrumentation were performed. At the second stage, which was performed 6 days after the first stage, the patient underwent anterior lumbar interbody fusion. The patient received physical therapy 1 week after the second stage.
Results
The patient's numbness improved immediately after the first posterior surgery. His fecal and urinary incontinence improved 6 months after discharge. He has been pain-free for a year and has returned to work.
Conclusion
A PubMed search was performed using the following keywords: lumbosacral spondyloptosis, lumbosacral dislocation, and L5–S1 traumatic dislocation. The search returned only nine reported cases of traumatic spondyloptosis. Traumatic spondyloptosis at the lumbosacral junction is a rare ailment that should be suspected in cases of high, direct, and posterior impact on the low lumbar area, and surgical treatment should be the standard choice of care.
Introduction
Lumbosacral spondyloptosis, by definition, is more than 100% anterior displacement of the L5 vertebra with regard to the sacrum. It is also known as grade 5 spondylolisthesis. 1 , 2 , 3 It represents a rare type of injury and most of the time is a result of a high-energy trauma. 4 , 5 This report describes our experience with a case of acute traumatic L5 spondyloptosis.
Case Report
A 28-year-old man presented with severe low back pain, numbness at the soles of feet, and bowel and bladder dysfunction. Two days before admission, a tree trunk fell on his back while he was seated. He remained under the tree for several hours until he was rescued. The patient was transferred to the hospital near his house and was followed for 2 days with the treatment of analgesic medication.
When he was transferred to our center, his physical examination was significant with tenderness of the posterior low lumbar area, wide ecchymosis in the lumbosacral area, and severe low back pain. Neurologic examination revealed 5/5 motor strength of both lower extremities according to manual muscle testing and numbness at the soles of his feet. He was not able to urinate and defecate by himself.
Radiologic workup was obtained including radiographs, magnetic resonance imaging, and computed tomography. Plain radiographs suggested L5 spondyloptosis with regard to S1 (Fig. 1). Computed tomography demonstrated double vertebral arch (Fig. 2), and magnetic resonance imaging suggested almost complete dural sac obstruction between L5 and S1 levels as well as disrupted disk space (Fig. 3).

Lateral radiograph of lumbar spine demonstrating spondyloptosis of L5 over S1.
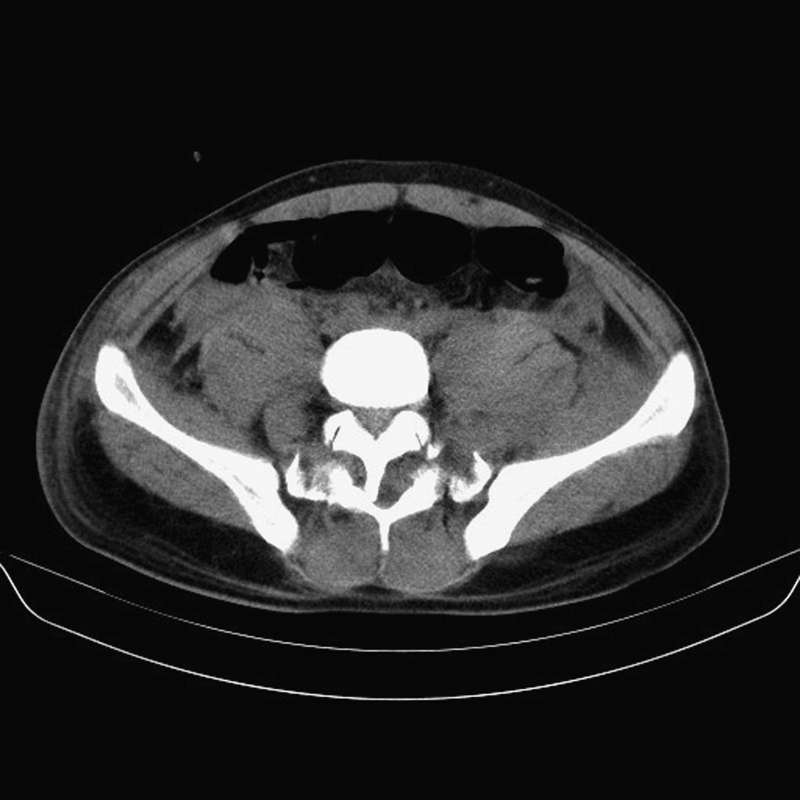
Computed tomography axial image demonstrating double vertebral arch at L5–S1.
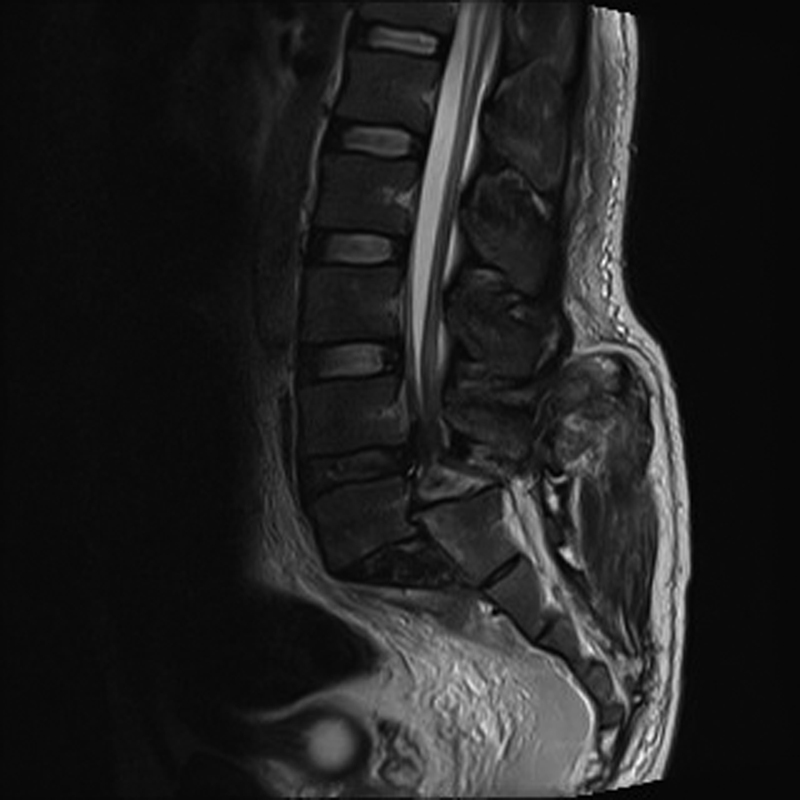
Magnetic resonance imaging showing complete dural sac obstruction between L5 and S1 levels and disrupted disk space.
Surgical treatment was chosen as the patient presented with severe low back pain in adjunct to neurologic deficit and unstable L5–S1 segment due to spondyloptosis. A two-stage posterior-anterior procedure was performed. At the first stage, the patient underwent surgery in a prone position with a classic midline incision. Intraoperatively, a gap between L4 and S1 segments and fracture-dislocation of L5 inferior facets were observed. Decompression of the dural sac and nerve roots was performed via laminectomy of L5 and inferior and superior parts of the laminae of L4 and S1, respectively. A dural tear was detected and repaired. Posterior instrumentation from L4 to S1 was then performed, followed by reduction of the L5 segment. Six days after the first stage, the patient underwent an anterior lumbar interbody fusion procedure trough a left paramedian approach. Both surgeries were completed uneventfully.
The patient received physical therapy 1 week after the second-stage operation. His numbness improved immediately after the first posterior surgery. His fecal and urinary incontinence improved 6 months after discharge. He has been pain-free for a year and has returned to work (Fig. 4A to 4C).
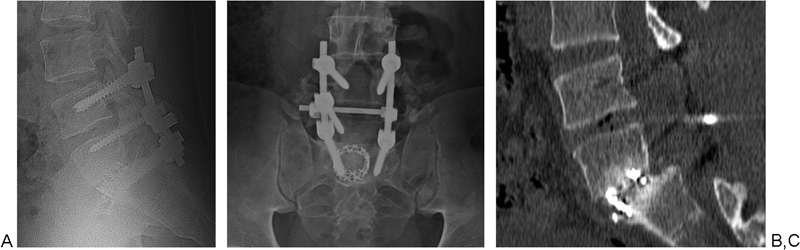
(A) Lateral and (B) anterior-posterior radiographs at postoperative month 6. (C) Computed tomography revealed solid interbody fusion between L5–S1 levels. The patient's fecal and urinary incontinence improved 6 months after discharge. He has been pain-free for a year and has returned to work.
Discussion
A PubMed search was performed by using the following keywords; lumbosacral spondyloptosis, lumbosacral dislocation, and L5–S1 traumatic dislocation. Only nine reported cases of traumatic spondyloptosis (Table 1) could be found in the English literature. Most of these cases (six of nine) were the result of motor vehicle accident or substantial falls. One case occurred following a grand mal epileptic seizure, one case resulted after a motor vehicle accident due to a tonic-clonic seizure, and one occurred following a landslide. 4 , 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 Our case, to our knowledge, is the first case that occurred after a direct impact of an object (tree trunk).
Traumatic spondyloptosis of L5–S1 cases in the literature
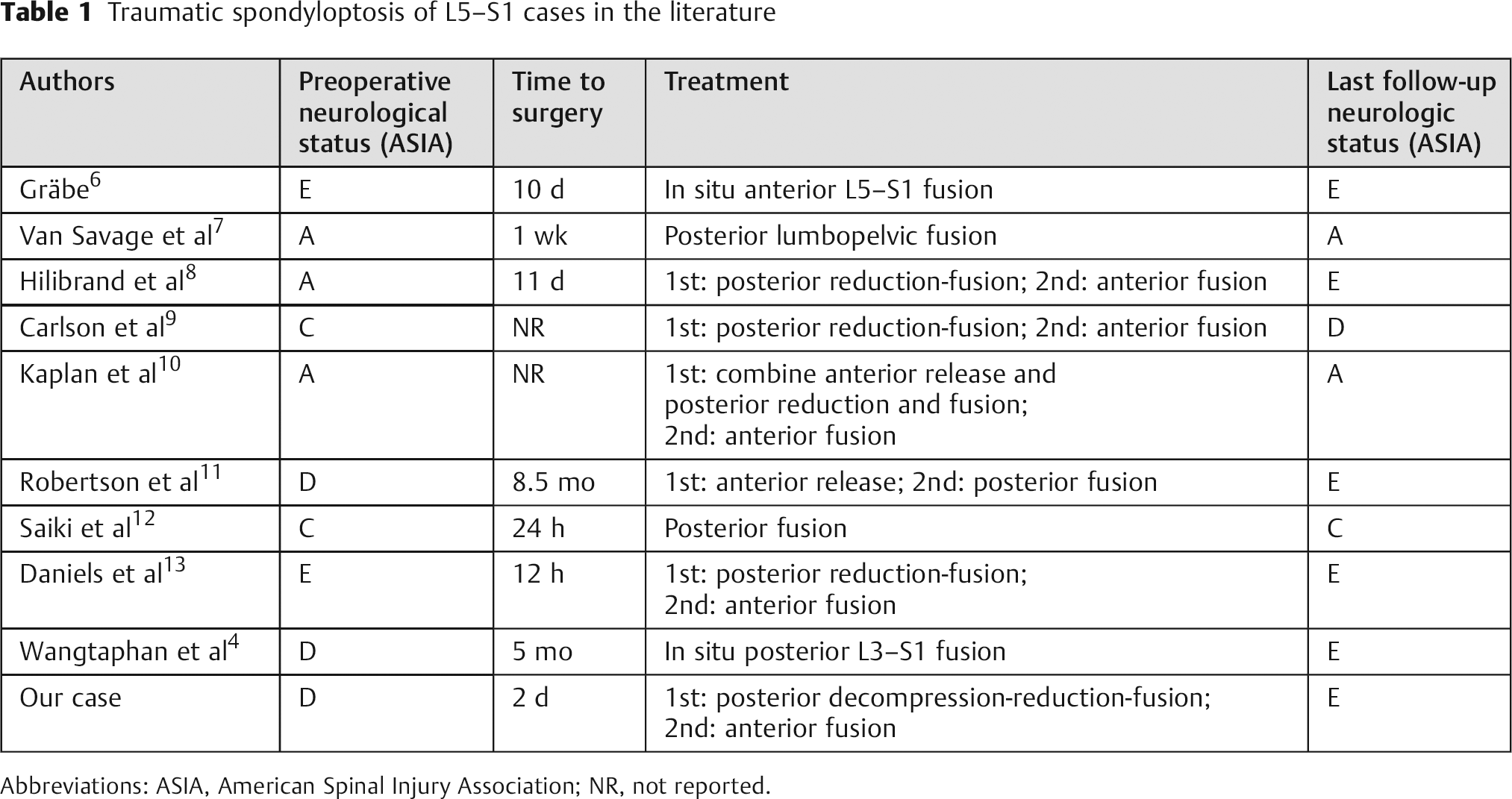
Abbreviations: ASIA, American Spinal Injury Association; NR, not reported.
Although there has been no biomechanical study to explain the pathomechanism of traumatic spondyloptosis, the injury tends to happen when a force is applied to the lumbar spine, especially when the pelvis and sacrum are in a fixed position. 10 , 14 However, Saiki et al reported in their review that hyperextension can lead to anterior lumbosacral dislocation if there is a preexisting spondylolytic lesion at L5. 12 In our case, we believe that the mechanism of injury was a sudden posterior-to-anterior force applied by a big tree trunk.
There have been different reports regarding the neurologic deficit caused by traumatic spondyloptosis including complete and incomplete neurologic deficit. Some reports suggested that grade of slip correlates with neurologic deficit. Of the nine cases with L5–S1 spondyloptosis, three had complete and four had incomplete neurologic injury, whereas two cases that resulted from seizures were neurologically intact. 4 , 8 , 9 , 15 In our case there was no motor deficit at the extremities but urinary and fecal incontinence as well as numbness in the sole of both feet. The patient's numbness improved after the first surgery. After a period of 6 months of physical therapy, his bowel and bladder incontinence completely resolved. The reason for this, in our opinion, may be a transient neuropraxia of S2–S5 nerve roots.
Surgical treatment for traumatic spondyloptosis is reasonable. Surgery aims to reduce, decompress, stabilize, and fuse the spondyloptotic segment. 4 , 6 , 13 As decompression was necessary in our case (due to neurologic deficit), we preferred to start with a posterior approach to decompress, reduce, and fix the unstable segment. To enhance fusion and stability, we then performed an anterior interbody fusion.
In conclusion, traumatic spondyloptosis at the lumbosacral junction is a rare ailment that should be suspected in cases of high, direct, and posterior impact on the low lumbar area, and surgical treatment should be the standard choice of care.
Disclosures
None