
Abstract
Study Design
Case study.
Objectives
We report the case of a 58-year-old Caucasian man, who presented with a 4-month history of increasing low back pain and gait difficulty. Objective neurologic examination revealed a severe paraparetic symptomatology without any sphincter involvement.
Methods
Spinal magnetic resonance imaging (MRI) showed an extradural mass formation situated dorsally at the level of thoracic vertebrae T2 to T4.
Results
A laminectomy was performed with total removal of the mass; histology suggested a highly vascularized lesion with lobular architecture, which seems a very rare case, compatible with a capillary hemangioma.
Conclusions
A careful follow-up for the next 4 years, including control MRIs every postoperative year, showed a very good neurologic condition of the patient and no recurrence on imaging findings.
Introduction
Vascular lesions involving the neuraxis are obviously more common within the intracranial territories. In the spine, vascular lesions in general are less frequently encountered than those inside the brain; nevertheless spinal vascular lesions are extremely challenging for the treating clinician, especially regarding the clinical consequences that might follow their appearance. Capillary hemangioma is considered a vascular malformation, based on the histologic findings. Considered as a vascular malformation, this type of tumor has been frequently found at autopsy in patients with idiopathic “diffuse” or progressive myelopathy, in the pre–magnetic resonance imaging (MRI) age. 1 , 2 It has even been reported as an incidental finding in 11% of spines on autopsy. 1 Progressive paraplegia, pain, and sphincter involvement are characteristics of these lesions. Due to their unaggressive behavior and benign histologic features, cases whose clinical course exceeded 20 years of history have been published. 3
Spinal epidural capillary hemangiomas are rarely reported, and a careful differential diagnosis with other spinal masses is necessary. Very important, on the other hand, is their histologic characterization, because distinguishing capillary hemangiomas from malignant vascular proliferations, which are characterized through intralesional hemorrhage and (albeit modest) cellular proliferation, is a decisive step, both surgically and prognostically. 4
Case Report
A 58-year-old Caucasian man presented with a history of pain involving both lower extremities and lasting 3 months, with progressive weakness seriously restricting his everyday life activities. Neurologic examination revealed a severe inferior spastic paraparesis, with a bilateral motor deficit 2 to 3/5 (motor strength evaluation, MRC scale) and a sensory impairment below T3 dermatome; brisk reflexes (+3) in both lower extremities and Babinski reflex were present as well.
MRI showed an extradural mass situated posteriorly at the level of three thoracic vertebrae (T2 to T4); the mass was isointense on T1-weighted images, hyperintense on T2-weighted images, and enhanced homogenously upon intravenous gadolinium administration (T1-weighted images; Fig. 1). Axial projections showed an extension bilaterally of the mass toward the intervertebral foramina, which involved two spinal levels (Fig. 2).

(Left) T1-weighted; (right) T1-weighted, contrast-enhanced magnetic resonance images showing an extradural posterior mass at the levels of thoracic vertebrae T2, T3, and T4. Note the bright T1 signal, considered as classic for this pathology.
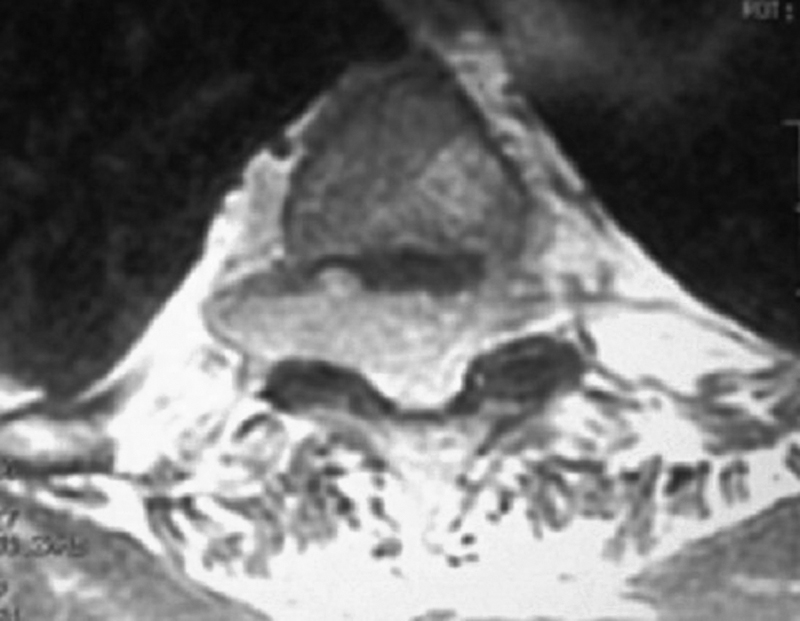
Axial magnetic resonance image, showing a bilateral tumor extension toward intervertebral foramina.
The patient opted for the surgical solution, and a T2 to T4 laminectomy was performed. Macroscopically a red epidural mass, soft and easily cleavable from the dura, was observed and totally resected. The histologic examination confirmed a capillary hemangioma. The finding was unexpected, because the preoperative history was rather one of a quick progression; even intraoperatively, the mass more closely resembled a hematopoietic tumor. The unusual localization was another challenging clue to the entire clinical picture.
Histologic examination demonstrated a highly vascular tumor, composed of vessels of various calibers (Fig. 3). The vessel walls were internally lined from endothelium with a total lack of smooth muscular elements; continuous basal lamina participated in the lobular architecture of the entire structure. No mitotic activity or cellular atypia was seen. The histologic diagnosis was that of a lobular capillary hemangioma. The lesion presented separated lobules, each of them fed from a vessel by itself.
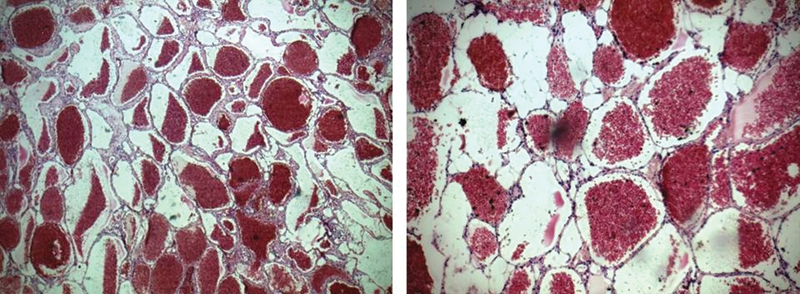
Histologic specimen (hematoxylin and eosin); (left) original magnification ×100; (right) original magnification ×200.
The patient had an uneventful postsurgical course and was discharged the third postoperative day. The first follow-up visit 1 month later showed an impressive improvement in the motor abilities (lower extremities 4 to 5/5 MRC scale) but the sensory deficit persisted for almost half a year, with dermatomal paresthesia (below T4) fading slowly but continually.
The patient had MRIs every year; no radiologic signs of tumor recurrence were seen.
Discussion
Capillary hemangiomas can be grossly distinguished from cavernous angiomas based on their clinical course. Cavernomas often present with an acute symptomatology, mainly related to intratumoral bleeding; this is an exceptional event for hemangiomas, which show a very slow progression of symptoms. 5 Considered as benign vascular lesions, capillary hemangiomas are most often encountered in the skin and soft tissues of pediatric patients and are commonly denominated as “pyogenic granulomas,” which is in fact a misnomer. 6 When discussing unusual localizations such as those adjacent to the spinal cord and an epidural placement, the general opinion favors the hypothesis of their originating from the vertebral body. 7 Capillary hemangiomas of lobular histologic characteristics have been found attached to dura, peripheral nerves, muscles, and skin. 8 Other locations have been described, such as intramedullary, as an extension from a nerve root capillary hemangioma, or from a cutaneous capillary hemangioma. 1 A posttraumatic origin has also been occasionally formulated. 9 Nevertheless, as for any other form of vascular malformation, capillary hemangiomas of the spinal cord are probably related with a dysembryogenetic process, when their localization is intramedullary. 10
Capillary hemangiomas of the spinal cord have been reported, although very rarely, in different levels of this structure, starting from the cervical cord to the cauda equina, regardless of the localization of the tumor with regard to the dura and the neuraxis. 8 , 11 , 12 , 13 , 14 Spinal intradural hemangiomas are reported more frequently, with clinical symptoms mimicking other intramedullary tumors. 13 Considered as benign tumors, nevertheless particular precautions are advisable, as authors occasionally report extensive bleeding when masses are incidentally approached. 11 On the other hand, cases with rapid regrowth after a presumably total resection have been noted as well within 6 months after initial surgery, a fact that indicates the extreme importance of close clinical and radiologic follow-ups. 14
Although intradural masses form the majority of the cases, there have also been a few published cases of epidural capillary hemangiomas; from a search of PubMed with the keywords “epidural capillary hemangioma,” six results were found. 1 , 7 , 15 , 16 , 17 , 18 Three of these cases had some nerve root involvement and foraminal extension, and one case was even considered and treated as a disk herniation. 15 , 16 , 17
Authors describe four clinical syndromes that characteristically depict the presence of extradural hemangiomas: slow and progressive spinal cord syndrome (the most common form); acute spinal cord syndrome; back pain; and radiculopathy. 19
Enlarging the scope of the search, other cases in particular settings can be found, interestingly related to pregnancy and to the complications of delivery. 20 , 21 The possibility of an intra- and/or extradural compression has to be taken into consideration when pregnancy is at the background, especially when making the differential diagnosis of paraplegias following labor activity. Indeed, uterine contractions result in increased venous pressure within the epidural venous system, thus altering the hemodynamics of an angioma, if one is present. 22
Two sources have described a particular form of the epidural masses; a Spanish group, encountering a cavernoma, described it as a reloj de arena (hourglass), which seems equivalent to the term dumbbell, as denoted by Badinand et al in their report of a capillary hemangioma. 7 , 23
When discussing the surgical approach of capillary hemangiomas, rather than intramedullary localization, authoritative sources advise that the treating surgeon must avoid potentially excessive treatment, because the benign nature of hemangiomas has been emphasized repeatedly. 5 , 10 Apart from the discrepancies, opinions converge on the necessity of a total resection of the benign mass. The same rule applies for the epidural hemangiomas, taking note of the fact that their almost constant foraminal extension makes a total resection of the intraforaminal portion difficult. 1
The unexpected intraoperative finding of a highly vascularized tumor brings with it the risk of diffuse bleeding and of an incomplete removal; even reoperation will not guarantee a complete resection. 24 Therefore, a careful preoperative workup is necessary, especially when the preoperative imaging is suggestive, with particular features including a lobular contour, T1 hyperintensity, or multisegmental involvement. 24 Of course, MRI with its different imaging modalities and sequences remains the most sensitive diagnostic tool. 25
Disclosures
None