
Abstract
Background Context
Isolated spinal artery aneurysms not associated with vascular malformations are exceedingly rare.
Purpose
To present a rare case of subarachnoid hemorrhage after thoracic radiculomedullary artery pseudoaneurysm rupture in a patient who abused synthetic cannabinoids and methamphetamines.
Study Design
Case report.
Methods
A 41-year-old man with a history of polysubstance abuse presented with acute-onset headache, back pain, and transient bilateral lower-extremity numbness. He reported daily use of the synthetic cannabinoid “Spice.” He denied use of other illegal drugs, but laboratory testing was positive for methamphetamines. Magnetic resonance imaging showed a focal hematoma at T2–3, and spinal angiography was negative for vascular abnormalities; however, a follow-up angiogram 6 days later revealed interval development of an irregular dilation of the left T3 radiculomedullary artery originating from the left supreme intercostal artery.
Results
Surgical trapping and resection of the lesion yielded a good clinical outcome.
Conclusions
Although two previous case reports have described patients with thoracic radiculomedullary pseudoaneurysm causing spinal subarachnoid hemorrhage (SAH), this is the first reported case associated with synthetic cannabinoids and methamphetamine abuse. Although this diagnosis is exceptionally rare, clinical presentation of SAH with associated back pain and lower-extremity symptoms warrants an aggressive imaging workup. Even in the setting of negative angiography, repeat cerebral and spinal angiograms may be necessary to identify a potentially treatable cause of spinal SAH.
Spinal subarachnoid hemorrhage (SAH) is most commonly due to arteriovenous malformations (AVMs) and tumors. 1 , 2 , 3 , 4 , 5 , 6 Spinal artery aneurysms associated with vascular malformations are rare but well-known causes of spinal SAH, whereas isolated spinal artery aneurysms are exceedingly rare. Although several case series have described both open and endovascular management of these lesions, 7 , 8 , 9 , 10 to our knowledge there are only two other reports of thoracic radiculomedullary pseudoaneurysm causing spinal SAH, neither of which was associated with synthetic cannabinoid (“Spice”) or methamphetamine abuse. We present a case of spinal SAH resulting from a rupture of a radiculomedullary artery pseudoaneurysm temporally associated with the use of Spice and methamphetamine.
Case Report
A 41-year-old man with a history of incarceration and polysubstance drug abuse presented with 1 day of acute-onset headache, upper back pain, and transient bilateral lower-extremity numbness. Prior to arrival at our institution, the patient was complaining of subjectively decreased sensation involving his bilateral lower extremities. Upon admission, the patient had a Glasgow Coma Scale score of 15. The patient did have mild nuchal rigidity and patchy decreased sensation to light touch at the T4 level and below but had normal motor strength and no evidence of abnormal upper-motor findings. Laboratory testing included a positive drug screen for amphetamines but otherwise was unremarkable. The patient admitted to daily smoking of illicit Spice but denied use of narcotics or amphetamines.
Computed tomography (CT) of the head revealed extensive posterior fossa SAH with a small amount of subdural hemorrhage layering along the falx and tentorium and mild ventriculomegaly (Fig. 1). A CT angiogram of the patient's head and neck was negative for any vascular abnormality but showed SAH throughout the craniocervical region. Magnetic resonance imaging (MRI) of the cervical, thoracic, and lumbar spine, although significantly limited by motion artifact, demonstrated a curvilinear focus of enhancement ventral to the left thoracic spinal cord at the T2–3 level (Fig. 2). Given the focal spinal clot, cerebral and spinal angiography was performed, but it was negative for any vascular abnormality. The patient underwent lumbar drain placement. Because of high clinical suspicion for a vascular abnormality, a follow-up cerebral and spinal angiogram was performed on hospital day 6. Follow-up spinal angiography demonstrated a focal irregularity and enlargement of the T3 radiculomedullary branch, which arose from the left supreme intercostal artery (Fig. 3). An echocardiogram was within normal limits and demonstrated no evidence of aortic anomalies.
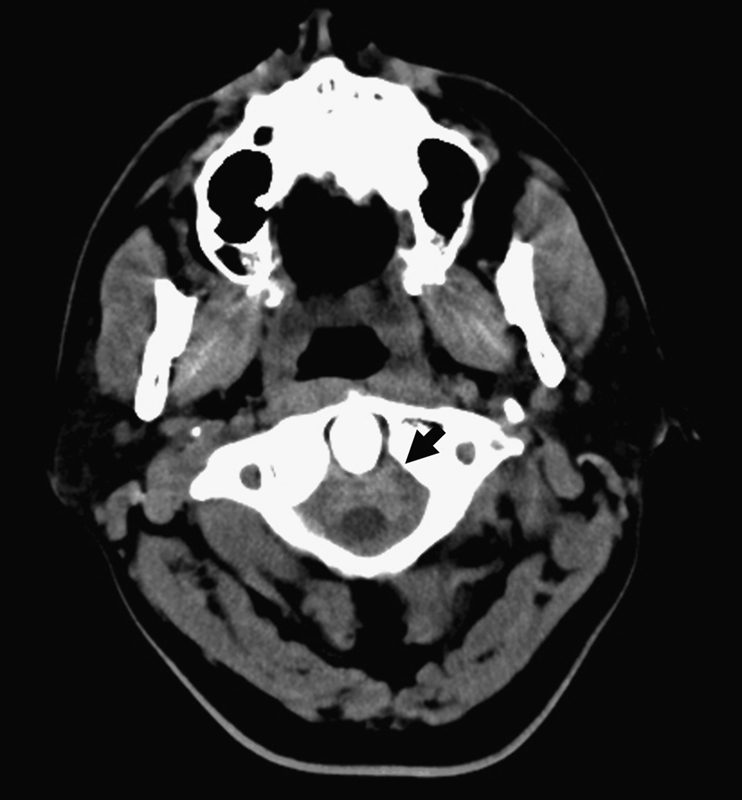
Noncontrast computed tomography image at the level of C1 showing extensive subarachnoid hemorrhage surrounding the upper cervical cord (black arrow).

Sagittal fat-saturated T1-weighted magnetic resonance image postgadolinium showing a small focus of enhancement (white arrow) posterior to the T2–T3 disc space on the left, corresponding with the location of the pseudoaneurysm. No corresponding intrinsic T1 signal was present on the precontrast T1 sequence.

Digital subtraction angiographic image from a subselective injection of the left supreme intercostal artery shows an irregular, fusiform pseudoaneurysm of the left T3 radicular artery (white arrow). This pseudoaneurysm was not present on the first spinal angiogram.
The patient underwent open clipping/trapping of the pseudoaneurysm. After a T2 and T3 laminectomy, the dura was opened sharply, revealing a focal subdural clot inferior to the exiting T3 nerve root. The clot was carefully elevated and evacuated, exposing the exiting nerve and associated radiculomedullary artery. The associated dentate ligaments were divided, and the T3 radiculomedullary artery was followed distally along the lateral extent of the spinal cord, revealing a focally thrombosed pseudoaneurysm. Intraoperative ultrasound with both color and power Doppler evaluation did not demonstrate any detectable flow. The proximal and distal segments were clipped, and the thrombotic arterial dilation was sent for pathological analysis.
Pathological evaluation demonstrated a well-organized blood clot with no appreciable vessel intima to allow evaluation for vasculitis. The dilated vessel wall revealed complete disruption of internal intima with nearly no appreciable vessel wall on the entire length of the dilated arterial segment.
Postoperatively, the patient remained neurologically intact without recurrence of his lower-extremity sensory symptoms. The patient was discharged to home on postoperative day 8. The patient was subsequently readmitted to the cardiology service 14 days later with an episode of coronary vasospasm and mild troponin elevation. The patient acknowledged continued daily Spice abuse but denied any other drug use. His toxicology screen was subsequently negative for methamphetamines. The patient was observed by the cardiology service for 24 hours and discharged without further complication.
Discussion
Although isolated spinal cord aneurysms causing SAH have been documented in several case reports, 9 , 10 , 11 , 12 , 13 they are exceedingly rare occurrences. The most common causes of spinal SAH are spinal dural arteriovenous fistulas (AVFs), AVMs, or vascular neoplasms (e.g., hemangioblastomas, cavernous malformations). 14 Despite their increased incidence in spinal SAH, spinal AVFs and AVMs typically present with symptoms of venous hypertension and progressive myeloradiculopathy. As an exception, type 2 (intramedullary) AVMs will present with SAH in 40 to 50% of cases, sometimes secondary to intranidal aneurysms. Neoplastic vascular lesions more frequently present with symptoms secondary to mass effect. 14 In contrast, spinal aneurysms most often present with SAH and acute-onset back pain. To our knowledge, we present the first case of spinal aneurysmal SAH secondary to methamphetamine abuse.
Massand et al 9 recently reported four patients with isolated spinal artery aneurysms. Similar to our patient, none of the patients had any additional intracranial aneurysms, connective tissue disease (e.g., Ehlers-Danlos, fibromuscular dysplasia), or history of aortic anomaly that might predispose them to aneurysm formation. Also similar to our patient, three of the patients reported in their series had fusiform dilation along the course of the artery and one patient was found to have a thrombosed aneurysm upon surgical exploration. All four patients were treated with open surgery with good clinical outcomes. In another recent series, Berlis et al 10 described three patients who presented with spinal SAH secondary to isolated ruptured spinal aneurysms. Interestingly, in this series, the authors reported spontaneous aneurysm occlusion in all three patients, who all had good neurological recovery.
Although exceedingly rare, thoracic radiculomedullary artery pseudoaneurysms have been reported in two previous cases in the literature. Walz et al 15 reported a patient with Moyamoya disease who presented with acute-onset headache and subsequent quadriplegia. After a negative cerebral angiogram, the patient underwent spinal angiography, which revealed an enlarged spinal artery arising from the supreme intercostal artery with a 1.1 × 1.1-cm irregular pseudoaneurysm associated with a cervical subdural hematoma. The patient was not a surgical candidate, and the aneurysm was managed via endovascular obliteration. Yahiro et al 16 reported a patient with a history of autoimmune hepatitis who presented with posterior fossa SAH and progressive lower extremity paresis. Spinal MRI demonstrated a subdural hemorrhage at the T4–5 level. Spinal angiography revealed a left-sided T5 radiculomedullary artery pseudoaneurysm originating from the fifth intercostal artery. The patient underwent open surgical trapping and resection of the aneurysm.
Increasingly, spinal AVMs are managed with endovascular techniques. This increasing experience suggests outcomes are highly dependent on the type and location of the lesion. 17 , 18 , 19 Although there are still limited data on the endovascular treatment of spinal fusiform aneurysms, the long-term occlusion rates of spinal dural AVFs may not be as high as those obtained with surgical ligation or excision. 20 Surgical treatment of vascular malformations, in particular dural AVFs, is generally curative with a low morbidity rate. 19 , 21 Given the intradural extramedullary appearance, the authors determined that surgical ligation represented a safe and durable treatment option in the present case.
Although cocaine and amphetamine abuse are well-known risk factors for intracranial hemorrhage 22 , 23 , 24 , 25 , 26 , 27 , 28 and myocardial ischemia, 29 , 30 , 31 , 32 , 33 , 34 the risks associated with synthetic cannabinoid abuse are largely unknown. The primary psychoactive ingredient in Spice is a synthetic cannabinoid, JWH-018 (1-pentyl-3-(1-naphthoyl)indole). 35 Similar to the primary psychoactive ingredient in cannabis, delta-9-tetrahydrocannabinol (THC), synthetic cannabinoids act upon the endogenous cannabinoid receptors. 36 Until recently, JWH-018 and other similar synthetic cannabinoids (JWH-081, JWH-250, AM-2201, RCS-4) were widely available for legal consumption. A recent move by the U.S. Drug Enforcement Agency and several individual states has made the sale and consumption of these synthetic cannabinoids illegal, thus creating a black market for the sale of Spice and various combinations of often-illicit intoxicating substances and known narcotics. 37
Myocardial ischemia, myocardial infarction, transient ischemic events, and ischemic strokes have all been linked to marijuana use 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 and are believed to be largely due to the increased heart rate and the labile effect on blood pressure produced directly by THC's interaction with central and peripheral cannabinoid receptors. 46 Although little is known about the in vitro effects of synthetic cannabinoids, several recent reports of acute cardiac events following consumption have appeared in the literature. 36 , 47 , 48 Despite these and other reports of complications associated with polysubstance abuse involving cannabis and cocaine, the potential deleterious effects from mixing synthetic cannabinoids with other illicit drugs are yet to be fully realized. 38 , 49 , 50 , 51
Liu et al 52 recently reported a 41-year-old patient who presented with acute-onset back pain and lower-extremity paresis. The patient tested positive for amphetamines and was found to have both thoracic SAH and a focal subdural clot. A spinal angiogram was negative for any vascular abnormality. The patient was treated with surgical evacuation, and at 6-month follow-up he had made a complete neurological recovery. As described in the review by Howington et al, 22 patients who present with intracranial SAH associated with cocaine use have a statistically higher rate of clinically significant vasospasm and a 3.3-fold increased risk for a poor outcome. Although there are not enough cases in the literature to know whether this holds true for spinal SAH associated with stimulant use, our patient had no symptoms of vasospasm during his hospitalization and was neurologically intact upon discharge. Interestingly, this patient was readmitted approximately 1 week later with delayed myocardial ischemia presumably secondary to methamphetamine abuse.
Although the association between stimulant use and intracranial aneurysmal SAH is well described in the literature, we present the first case of aneurysmal spinal SAH associated with methamphetamine and synthetic cannabinoid abuse. Similar to previously reported cases of aneurysmal spinal SAH, our patient made a good neurological recovery and demonstrated no evidence of any additional intracranial vascular abnormalities. In addition, as several authors have observed with their patients, our patient ultimately went on to spontaneous thrombosis of the pseudoaneurysm. Although this diagnosis is exceptionally rare, clinical presentation of SAH with associated back pain and lower-extremity symptoms warrants an aggressive imaging workup. Even in the setting of negative angiography, repeat cerebral and spinal angiograms may be necessary to identify a potentially treatable cause of spinal SAH.
Disclosures
Wilson Z. Ray, None
Khaled M. Krisht, None
Alex Schabel, None
Richard H. Schmidt, None
Footnotes
Acknowledgments
The authors thank Lubdha Shah, MD, and Kristin Kraus, MSc, for assistance in the preparation of this paper.