
Abstract
Cystic thymoma was diagnosed in 14 cats in a period of 6 years. The most common clinical sign was laboured breathing. The tumours were characterized by various-sized cystic spaces with central vessels. The epithelial cells varied from oval to spindle to polygonal cells enclosing cystic spaces or in pure epithelial cell components. The nuclei of the neoplastic cells had scattered chromatin and small nucleoli. The cytoplasm was pale eosinophilic. The concentration of mature lymphocytes varied from area to area with rare germinal centres.
Immunohistochemically, the epithelial cells stained only with AE1/AE3. The central vessels were positive for vimentin, smooth muscle actin, and factor VIII antigen. Electron microscopy revealed that the cyst walls were lined by epithelial cells that were joined by desmosomes, and the walls were well separated from the cystic spaces by a well-defined basement membrane. The neoplastic epithelial cells contained scattered tonofilaments. Three of the cats had metastasis to the lymph nodes and lungs. Two novel cases of ectopic cystic thymoma have also been described. Results of this study reveal that cystic thymoma is uncommon in cats, and that the histomorphologic, immunohistochemical, and electron microscopic features are similar to those of cystic thymoma in humans.
The thymus is a complex but highly specialized organ. It is derived from the third and partially from the fourth pharyngeal pouches and contains cells from the three germinal layers. In addition to the main components (lymphoid cells, mostly T-cells, and epithelial cells), the thymus contains various other cell types with the potential to develop neoplasms, both epithelial and mesenchymal (Suster & Rosai 1990).
Thymoma is a neoplasm arising from epithelial cells that are often intermixed with a variable number of small, non-neoplastic lymphoid cells. In humans, various histologic classifications of thymoma and thymic carcinoma are based on the proportion of epithelial cells to lymphocytes, a cortical or medullar location, and identification of the different types of epithelial cells composing the tumour (Rosai & Levine 1976, Suster & Rosai 1991b, Kuo & Lo 1993, Moran 1995), but histologic classification has not proven very useful as a prognostic factor (Rosai & Levine 1976, Kuo & Lo 1993).
Thymoma as reported in humans is rare in animals. The neoplasm has been reported in cattle, dogs, cats, sheep, goats, horses, pigs, and rabbits (Parker & Casey 1976, Carpenter & Holzworth 1982). In cats, both benign and malignant thymoma with metastasis have been reported (Mackey 1975, Dubielzig & DeLaney 1980, Carpenter & Holzworth 1982, Middleton et al 1985).
It is reported that 40% of thymomas in humans are characterized by cystic degeneration. In some, the cystic changes proceed to the extent that most or all of the tumour becomes cystic (Rosai & Levine 1976, Suster & Rosai 1991a, Suster & Rosai 1992, Suster & Moran 1995). The criteria for diagnosing cystic thymoma have been established as follows (Suster & Rosai 1991a, Suster & Rosai 1992, Suster & Moran 1995): (1) solid expanses within the cyst wall consisting of a dual population of epithelial cells and small mature lymphocytes; (2) perivascular spaces and foci of medullary differentiation; and (3) the absence of an epithelial lining. The pathogenesis of these cysts is attributable to the distension and fusion of the perivascular spaces (Suster & Rosai 1992, Suster & Moran 1995).
In contrast, in thymoma with multilocular cysts, the cystic spaces are lined by flattened, cuboidal, and columnar often ciliated or squamous epithelial cells with normal thymic tissue in the walls (Suster & Rosai 1991a, Suster & Rosai 1992, Suster & Moran 1995). In many instances, the multilocular cysts can be traced to distended degenerating Hassall's corpuscles. These multilocular cysts are often accompanied by inflammation and follicular lymphoid hyperplasia. Similar cystic changes and inflammation may be seen in cystic thymoma, but the changes in involve the non-neoplastic thymus that surrounds the tumour rather than the tumour itself. Cystic changes and cystic thymoma have also been reported in cats (Carpenter & Holzworth 1982, Gores et al 1994, Galloway et al 1997, Malik et al 1997).
Materials and methods
All cases of thymoma in cats diagnosed by the Department of Pathology of The Animal Medical Center from 1993 to 1998 were reviewed. Of 25 thymomas, 11 (44%) cystic thymomas were identified including one thymic carcinoma. Three additional cases of cystic thymoma were taken from the necropsy records for the same period, so that a total of 14 thymomas were included in the study. Cystic thymoma was diagnosed on the basis of the criteria described above. Lymphoma of the anterior mediastinum, including thymus, was not included. The tissues were fixed in 10% buffered formalin, routinely processed, and stained with haematoxylin and eosin. A few of the tumours (four) were stained with mucin carmine. Immunohistochemical studies were performed on selected slides by use of a super-sensitive immunodetection system (Biogenics Corporation, Sam Romon, California 94583, USA), an improved biotin-streptavidin amplification system, following the instructions provided in the kit. Sections were stained for AE1/AE3 vimentin, factor VIII antigen, and smooth muscle actin (SMA).
For electron microscopic examination, tissues were fixed in a mixture of buffered formalin and glutaraldehyde, post-fixed in osium tetroxide, dehydrated in graded alcohol, and embedded in an epoxy resin. Specimens for transmission electron microscopy, selected from thick epoxy sections stained with toludine blue, were sequentially stained with uranyle acetate and lead citrate.
Clinical and gross pathologic information were collected from the appropriate records.
Results
Clinical findings
Of the 14 cats with cystic thymoma, 12 were domestic short hair cats, one was a Maine coon, and one was an Abyssinian. The age range was 4 to 16 years, and the median age was 10 years. The number older and younger than 10 years was equal. There were seven neutered males, five neutered females, one intact male, and one intact female.
The most common clinical signs on examination were laboured breathing and dyspnoea in nine of the 14 cats (64%). Less common clinical signs were weight loss (two cats), anorexia (three), cough (three), sneezing (one), and intermittent vomiting (one). Muffled heart sounds were ausculted in two cats because the tumour was located inside the pericardial cavity.
Results of biochemical analysis of serum revealed high glucose, high blood urea nitrogen, and high creatinine in two cats each, and high alkaline phosphate, high triglyceride, high cholesterol, and high total protein in one cat each.
Radiography and ultrasound were diagnostic in all cats with an anterior mediastinal mass. Ultrasound revealed complex, hyperechoic areas in almost half of the anterior mediastinal masses (8). Various quantities of pleural fluid were seen in all cats. In the two cats with muffled heart sounds, the heart was displaced by a mass enclosing the heart and causing cardiac tamponade, and in one of the two, the mass was partly intra-and partly extrapericardial. In both, the mass was diffusely hyperechoic.
Follow-up
Half the cats (7/14) with cystic thymoma were killed, six after diagnosis and one after 30 days because of recurrence. Five cats were alive at the last inquiry, 15 to 2520 days after diagnosis. The longest surviving cat had three tumour resections and radiation and chemotherapy after the last resection. This cat had pulmonary metastasis. The fourth cat was alive after 306 days. The fifth cat was lost to follow-up after 15 days. Follow-up information was not available for two of the cats.
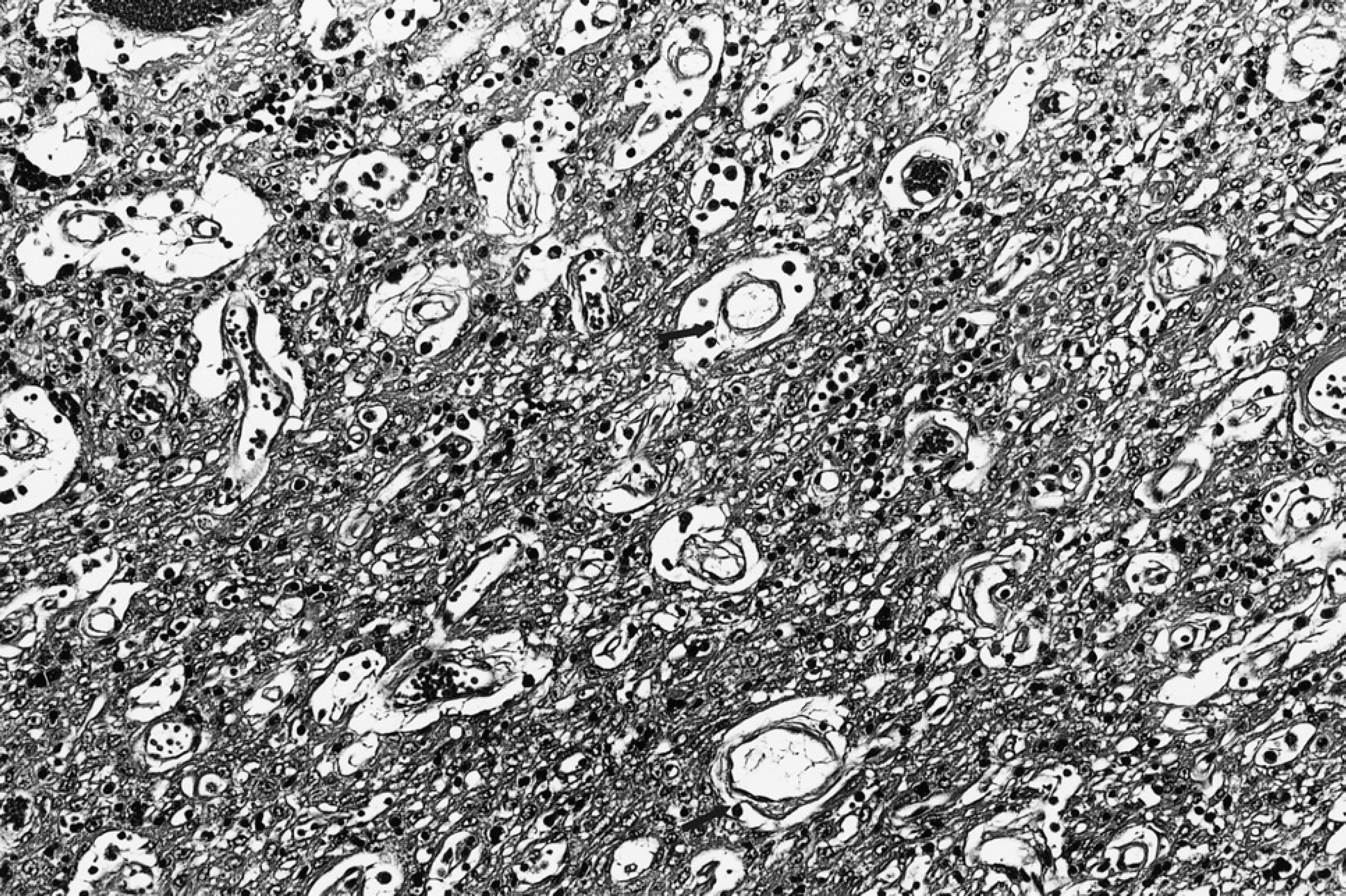
Cystic thymoma. Notice the small to moderately-sized cysts with central vessels and perivascular spaces surrounded by neoplastic epithelial cells (arrows). (Haematoxylin and eosin, magnification x200.)
One cat with cystic thymoma and lymph node metastasis developed myasthenia gravis 8 months after surgery. The acetylcholine receptor titre antibody was 0.51 nmol/l initially, going up to 0.84 nmol/l; this cat responded well to appropriate treatment. The acetylcholine receptor antibody value was 0.12 nmol/l 2 weeks later, even though there was no radiographic evidence of tumour recurrence or metastasis. The cat was alive 1 year after surgery.
Gross pathology
Three-dimensional measurements were available for six of the neoplasms. The smallest and the largest neoplasm were 48 cm3 and 305 cm3, respectively. The mean volume was 212 cm3. Four of these six neoplasms were located in the cranial mediastinum. One of these four was intrapericardial, enclosing the heart, and another involved both the pericardial sac and the mediastinum. Most of the six neoplasms were described as encapsulated. Two neoplasms were adherent to the major vessels and adjoining lungs. All were described as grey or brown with variously cystic, solid, or spongy areas.
Histopathology
The neoplasms were characterized by various-sized, confluent, macro- and microcystic spaces. Many of the spaces had central blood vessels and perivascular spaces (Fig 1). The larger confluent cystic spaces did not have vessels and were not lined by ciliated or squamous epithelial cells.
The cysts were separated by stroma containing a mixture of epithelial cells and small lymphocytes forming a single to multiple cell layer, often merging with solid areas containing an intimate mixture of epithelial cells and lymphocytes. The neoplastic cells were oval, spindle, and polygonal, the nuclei had scattered chromatin with one or two small nucleoli, and the cytoplasm was pale, eosinophilic, or vacuolated (Fig 1). Clear cell components were seen in five neoplasms. These cells had distinct cell borders and empty cytoplasm. Only one neoplasm had a high number of mitotic figures. The mitotic rate was one to two per high power field. Areas of oedema and partial necrosis were seen, with eosinophilic, non-cellular material enclosing small groups or rows of neoplastic cells. Some of the cystic perivascular spaces contained a few lymphocytes, red blood cells, or pale eosinophilic material. One neoplasm had areas resembling follicular configuration with greyish, mucoid, mucicarmine-negative material. Some of these structures had central vessels with perivascular spaces.
Cystic thymoma. Notice areas of spindle cells between lymphoid follicles. (Haematoxylin and eosin, magnification x200.)
The proportion of epithelial cells to lymphocytes in all the neoplasms varied from neoplasm to neoplasm and from area to area within the same neoplasm.
All 14 neoplasms had distinct fibrous capsules with fibrous interlobular septae. In half of the neoplasms, the subcapsular and interlobular spaces contained bands of spindle cells and scattered lymphocytes, which merged with cystic areas, in which islands of spindle cells were also seen (Fig 2).
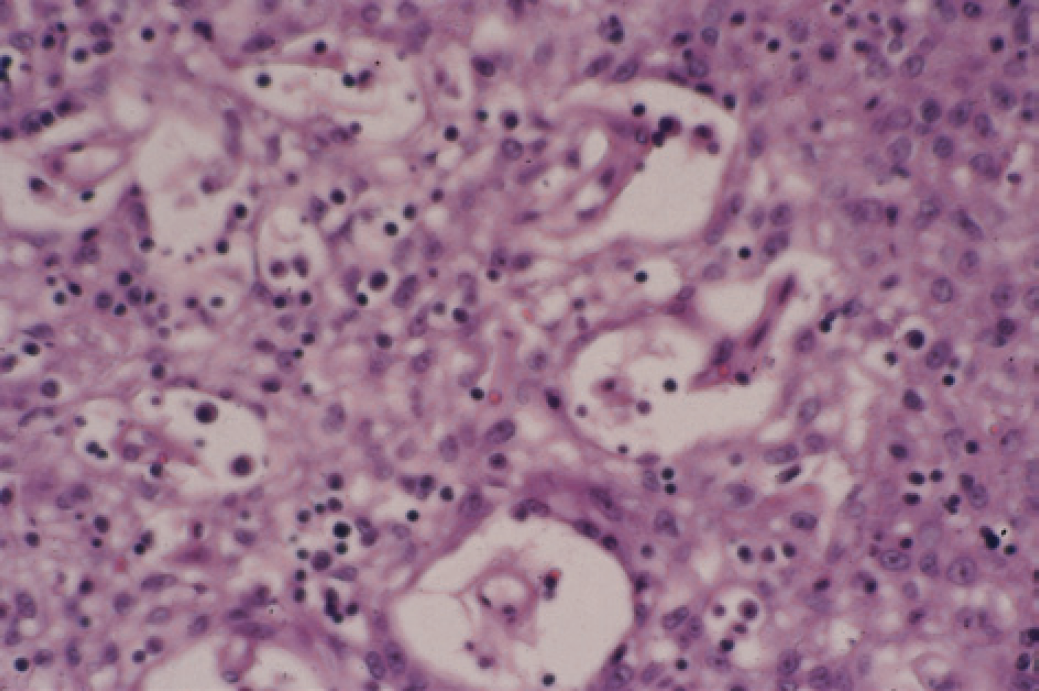
Medullary changes were characterized by well-defined round foci containing small, mature lymphocytes mixed with abundant, plump epithelial cells. Rarely, a Hassall's corpuscle was associated with the changes (Fig 3).

Cystic thymoma. Notice the medullary changes with a Hassall's corpuscle (arrow). (Haematoxylin and eosin, magnification x200.)
Three of the cats had distant metastasis. One had both lung and hilar lymph node metastasis, while the other two had only hilar lymph node metastasis. The lung metastasis contained an intimate mixture of epithelial cells and lymphocytes, similar to regular thymoma, whereas the lymph node metastasis had focal microcystic areas with central vessels. The lung and lymph node metastases were observed 970 days after surgery. In the other two cats, lymph node metastasis was seen at the time of surgery. Another cat had severe mesothelial proliferation with sclerosis in and around the capsule, resembling epithelial-type mesothelioma. Three other cats had an additional tumour seen in including intestinal mast cell tumour with lymph node metastases (one), intestinal lymphoma (one), and pulmonary carcinoma (one).
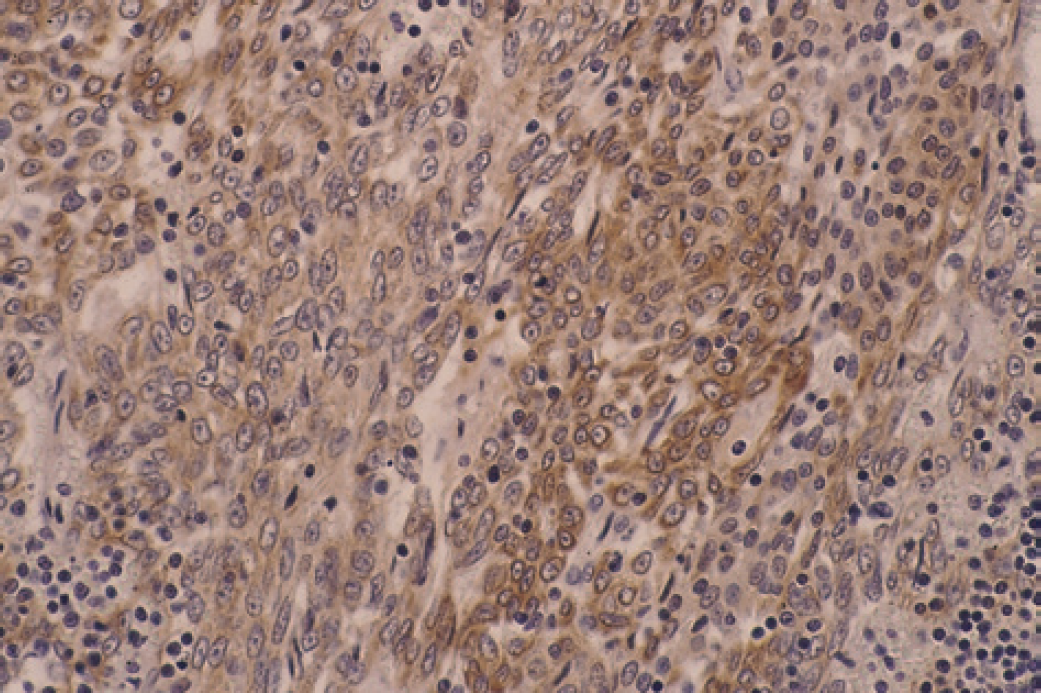
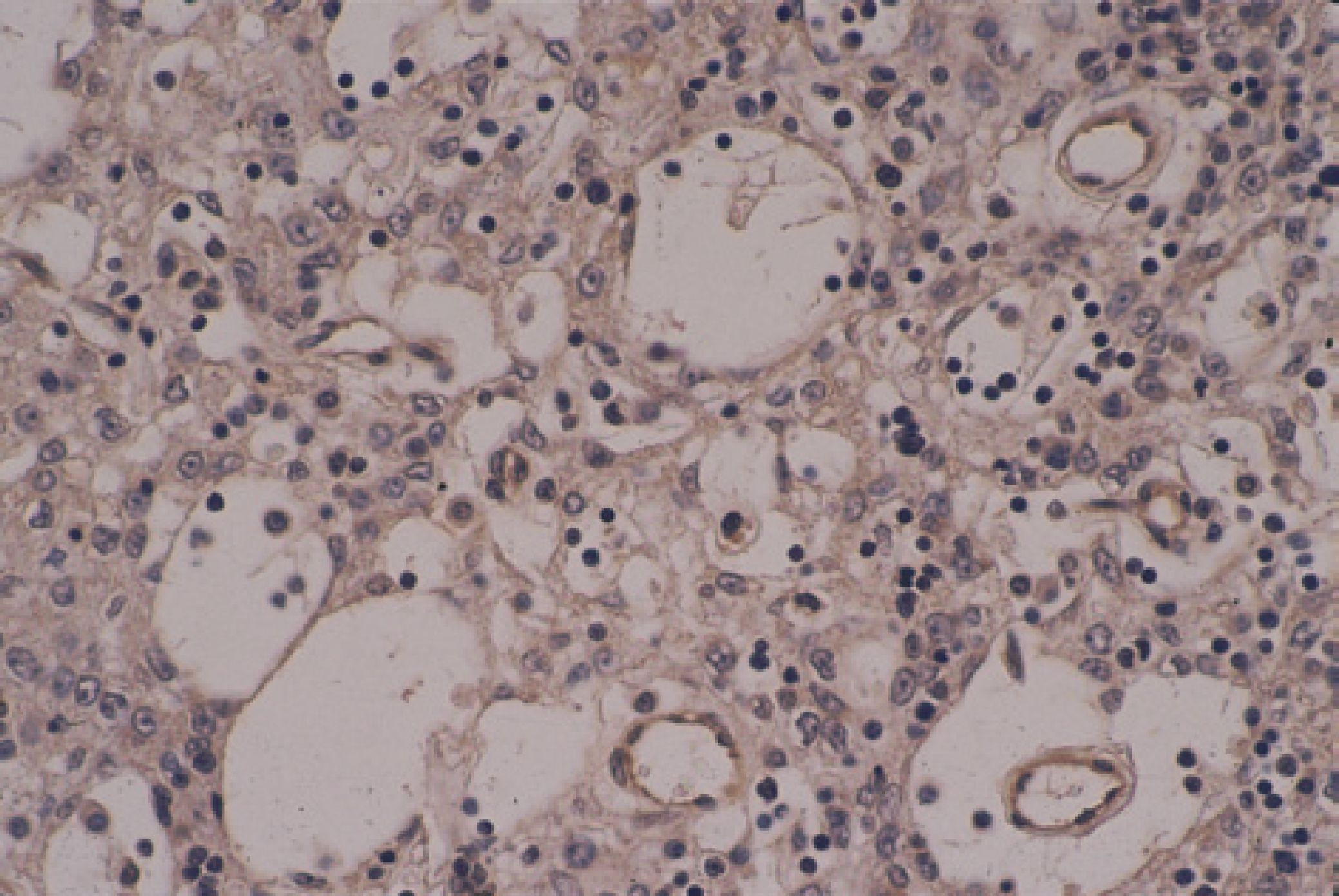
Cystic thymoma. Immunohistochemically stained for AE1/AE3 (by supersensitive immunodetection system, Biogenex Corporation). Notice the peri-cytoplasmic staining in the tumour cells (arrows) (counterstain, Gill III haematoxylene, magnification x400).
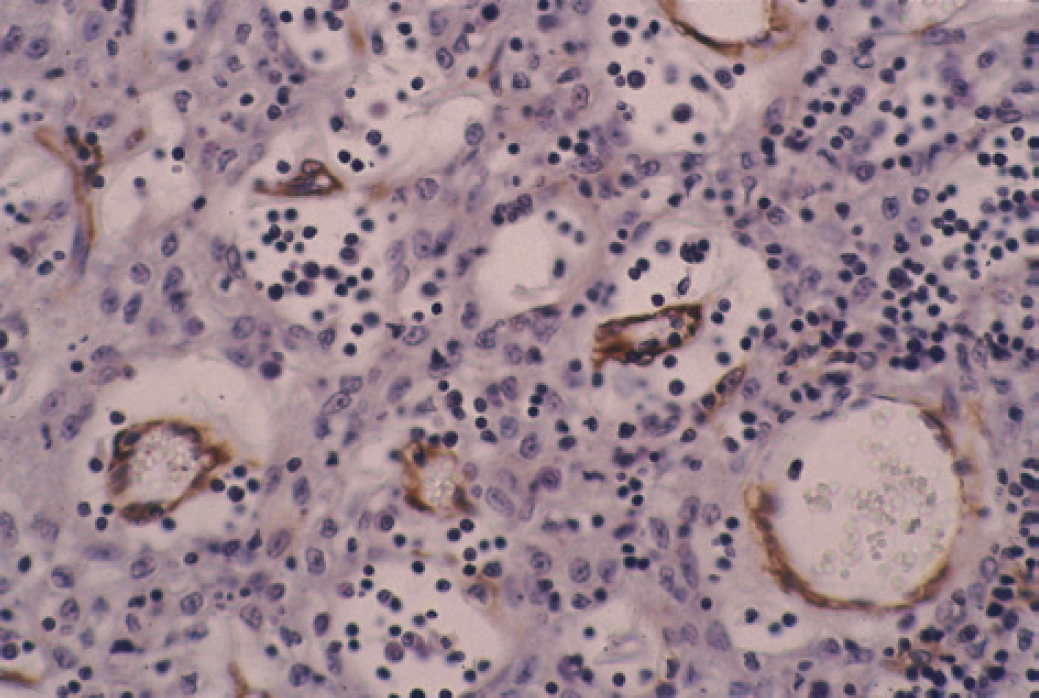
Cystic thymoma. Immunohistochemically stained for smooth muscle actin (by supersensitive immunodetection system, Biogenex Corporation). Notice the central vessels in the cysts (counterstain, Gill III haematoxylene, magnification x400).
Cystic thymoma. Immunohistochemically stained for factor VIII antigen (by supersensitive immunodetection system, Biogenex Corporation). Notice the central vessels in the cysts (counterstain, Gill III haematoxylene, magnification x400).
Immunocytochemistry
The epithelial cells, including the clear cells, in both the cystic and solid areas stained with AE1/AE3 in varying intensity (Fig 4). None of the epithelial cells were stained with vimentin, SMA, or factor VIII antigen. The central vessels in the cysts were stained with vimentin, SMA (Fig 5), and factor VIII antigen (Fig 6), clearly demonstrating the vessels.
Electron microscopy
Three of the 14 thymomas were submitted for ultrastructural evaluation. The walls of the variable-sized cysts were lined with one to three layers of round or oval-shaped epithelial cells that were joined by desmosomes and lined by a continuous basement membrane (Figs 7 and 8). Solid foci consisting of admixtures of epithelial cells and lymphocytes in varying proportions were also identified (Fig 8). The cytoplasm of the epithelial tumour cells contained scattered tonofilaments, clusters of glycogen particles, and inconspicuous organelles (Figs 7 and 8). Smaller cystic spaces also were evident between the epithelial cells lining the true cysts (Fig 7). No true lumen or microvilli were identified.
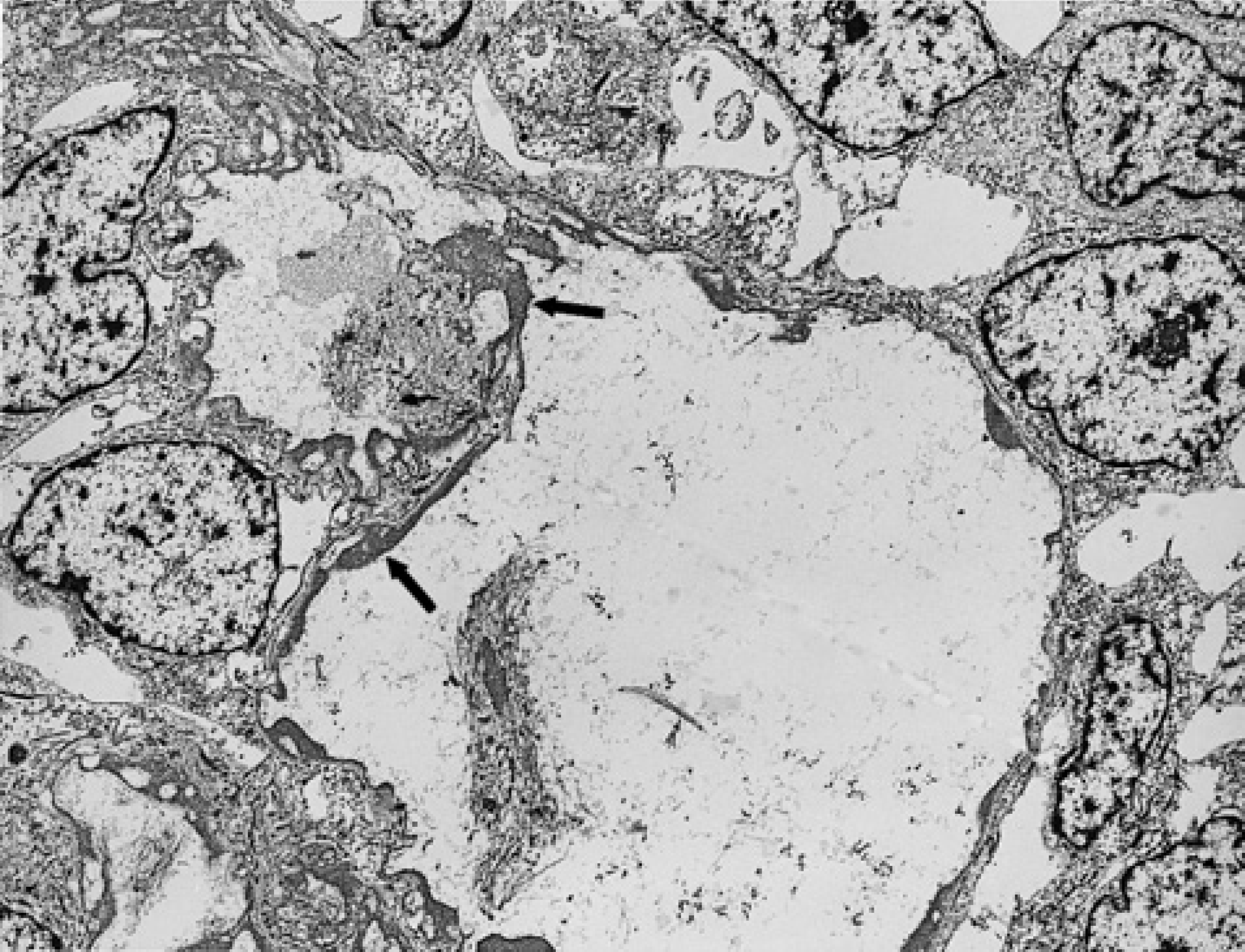
Ultrastructural appearance of cystic thymoma, showing large, empty, cyst-like spaces lined by linear deposits of amorphous substance (arrows). Surrounding tumour cells have a bland appearance and small, uniform nuclei (magnification x3018).

Detail of a cyst wall composed of oval-shaped epithelial cells joined by scattered desmosomes (arrow head) intermixed with small lymphocytes (arrows) (magnification x4200).
Discussion
Cystic changes in the anterior mediastinum are relatively uncommon in humans and result from different mechanisms (Rosai & Levine 1976, Suster & Rosai 1990, Suster & Rosai 1991a, Suster & Rosai 1992, Suster & Moran, 1995). Most are non-neoplastic, either congenital or acquired, and are of branchial origin. Cystic changes can be superimposed on various neoplasms in the anterior mediastinum, including thymoma. In thymoma, cystic changes develop in two ways: as a component of thymoma, or in the non-neoplastic, thymic parenchyma primarily located adjacent to the neoplasm. In both types, the cysts are lined by epithelial cells including squamous cells (Rice 1992, Suster & Rosai 1992). Diagnosis of cystic thymoma in this study was done according to previously described criteria (Suster & Rosai 1991a, Suster & Rosai 1992). According to our results, cystic thymoma in cats is morphologically, immunohistochemically, and ultrastructurally similar to that reported in humans (Suster & Rosai 1991a, Suster & Rosai 1992, Suster & Moran 1995).
Thymic branchial cysts have been described in both dogs and cats (Liu et al 1983). These non-neoplastic lesions are occasionally seen in necropsy and biopsy material.
Cystic thymoma and cystic changes in thymoma have been described in dogs and cats (Carpenter & Holzworth 1982, Galloway et al 1997, Malik et al 1997). In one study of 11 thymomas in cats, six (55%) had cystic changes (Carpenter & Holzworth 1982). These cysts were reported to be lined by flattened epithelial cells, which occasionally formed sheets of ‘spindle form cells’, but perivascular changes were not described. In another report of cystic thymoma, no histologic description of the cystic component was included (Galloway et al 1997). In another study of two cats, the cysts were histologically described as being lined by cuboidal and/or squamous cells (Malik et al 1997). Gores et al (1994) described cystic lesions in eight of 12 (67%) thymomas in cats, which apparently were lined by spindle-shaped thymic epithelial cells like the rest of the tumour. No mention was made of other components of cystic thymoma.
It is apparent from the above review that all of the criteria recently established (Suster & Rosai 1991a, Suster & Rosai 1992, Suster & Moran, 1995) for the diagnosis of cystic thymoma were not taken into consideration in these studies. Some of the neoplasms described can be considered cystic thymoma, but those with cysts lined by cuboidal cells and differentiated epithelial cells cannot be so considered. These should be considered thymoma with multi-lobular cysts (Suster & Rosai 1991a). Thus, it is difficult to compare our results with those of these previous studies.
The clinical signs seen in the cats of this study—lethargy, anorexia, and various respiratory difficulties—are non-specific; but with radiography and, especially, ultrasound, thymic neoplasms were diagnosed in all 14 cats. Six of the cystic thymomas of this study were described as complex, hyperechoic, anterior, mediastinal masses, which differentiated them from other anterior mediastinal masses, especially lymphoma (Konde & Spaulding 1991).
In two cats, the tumour was located in the pericardial sac. In one, the neoplasm was located in the pericardial sac enclosing the heart, which we considered the primary site. The second one involved the pericardial sac as well as the anterior mediastinum, making it difficult to determine the primary site. It was not considered primary in the pericardium. Review of the English literature revealed no reports of intrapericardial thymoma in cats. The location in the intrapericardial sac makes the neoplasm more dangerous because of the limited space for the pericardial sac to extend. Compression of the heart and major vessels can lead to cardiac tamponade. Ectopic thymoma in humans is extremely rare. The neoplasm has been described in the neck, bronchial tract, pulmonary parenchyma, thyroid and parathyroid glands, and pleural cavity (Rosai & Levine 1976, Moran et al 1995, Payne et al 1994, Shih et al 1997, Fushimi et al 1998). Only a few intrapericardial thymomas have been described, including one cystic thymoma (Schloss et al 1975, Airan et al 1990, Mirra et al 1997). Recently, two cases were described, but neither was cystic (Mirra et al 1997).
The histogenesis of ectopic thymoma is not clear. The most convincing theory is that the abnormal development of the thymus gland during its phase of embryonic descent from the thymic analogue is associated with misplacement of gland remnants at various sites. But the theory of uncommitted ‘germinal stem cells’ as the origin of pulmonary thymoma may as well be considered for other ectopic thymomas (Moran et al 1995, Suster & Moran 1995).
A clear cell thymoma has been described in a cat on the basis of histologic findings (Mackey 1975). Rarely, clear cell components are seen in thymoma of cats and dogs (Carpenter & Holzworth 1982, Aronsohn et al 1984). In five of the 14 neoplasms in this series, clear cells containing clear or vacuolated cytoplasm (commonly containing glycogen) were seen in various numbers at random in both solid and cystic areas. Since clear cells are seen in a variety of neoplasms, their presence in thymoma is most likely not significant (Rosai & Levine 1976).
Three of the cats (21%) in this series had distant metastasis. One cat developed metastasis to the lungs and hilar lymph nodes more than 4 years after resection of the cystic thymoma. In the other two cats, the hilar lymph nodes were involved at the time of surgery for thymoma. The pulmonary metastasis was morphologically similar to regular noncystic thymoma; but the lymph node metastasis had microcystic areas with prominent vessels and perivascular spaces, similar to that found in primary cystic thymoma, suggesting that both solid and cystic components be found in metastatic lesions.
Metastasis in humans with thymoma is rare (Rosai & Levine 1976, Suster & Rosai 1991b, Suster & Rosai 1992). In one study of cystic thymoma in humans, none had metastasis (Suster & Rosai 1992). Although thymoma with metastasis has rarely been described in dogs and cats, none of the thymomas with cysts had metastasis (Robinson 1974, Carpenter & Holzworth 1982, Aronsohn et al 1984, Middleton et al 1985). In this series, three cats (21%) had metastasis, which has to be considered a high rate.
Acquired myasthenia gravis is the most common systemic disease associated with thymoma, occurring in 29% of the thymomas in humans and 47% in dogs (Rosai & Levine 1976, Aronsohn et al 1984, Suster & Rosai 1991b, Klebanow 1992). In one human study, association of myasthenia gravis to thymoma reached 63.4% and correlated well to different histologic types (Kuo & Lo 1993). Rare cases have been reported in cats, and one of the cats had cystic changes in the thymoma (Joseph et al 1988, Scott-Montcrieff et al 1990, O'Dair et al 1991). Clinical signs of myasthenia gravis were observed in two cats, 2 weeks after surgical removal of thymoma (Gores et al 1994); but serum contained a high titre against acetylcholine receptors, both before and after surgery (6.5 and 10.5 nmol/l, respectively). One cat responded to appropriate treatment. The other cat developed oesophageal dysfunction 10 days after surgery; this cat responded to treatment, but the serum titre against acetyl-choline was not evaluated. In our series, one cat with cystic thymoma and lymph node metastasis developed myasthenia gravis 8 months after surgery without radiographic evidence of recurrence or metastasis. The cat responded to treatment. It is likely that there was undetectable recurrence or late antibody reaction.
Various other paraneoplastic syndromes described in humans, dogs, and cats with thymoma were not observed in the cats of this study (Rosai & Levine 1976, Carpenter & Holzworth 1982, Harris et al 1991).
Several immunohistochemical studies of thymoma in humans have been done to characterize the epithelial and lymphocytic cells in order to differentiate between the different histologic types and their biologic behaviours (Kodama et al 1986, Sato et al 1986, Eimoto et al 1990, Fukai et al 1992a, Fukai et al 1992b, Tateyama et al 1997). A few immunohistochemical studies that used intermediate filaments have been done in dogs and cats (Vos 1990, Gonzalez et al 1997). In the dogs, the neoplastic cells stained with a wide spectrum keratin and vimentin, thus suggesting a bimodal differentiation (Vos et al 1990). In our series, the epithelial cells of the cystic thymomas stained in different intensities with a broad-spectrum keratin (AE1/ AE3). None stained with vimentin, SMA, or factor VIII antigen confirming epithelial origin. Vimentin, SMA, and factor VIII antigen clearly demonstrated the blood vessels in the centre of the cysts (peripherally lined by epithelial cells), thus defining the pathogenesis of the cystic changes.
The electron microscopic studies in two of the cases confirmed that the walls of the cysts were composed of thymic epithelial cells that were joined by desmosomes, contained tonofilaments, and were separated from the cystic spaces by a continuous basement membrane. The clear cells seen by light microscopy contained aggregates of glycogen particles. True squamous differentiation, ie, cells containing numerous tonofilaments, were not seen in the examined materials (Erlandson 1994).
In one study of cats with cystic thymoma, the cats lived up to 1860 days after diagnosis (Gores et al 1994). In our series, even though two cats lived 500 and 2520 days, respectively, most of the cats were euthanized immediately after diagnosis. This does not add to the available information regarding prognosis.
In conclusion, cystic thymoma in cats is not uncommon compared with prevalence in humans and dogs. This neoplasm has clinical, morphologic, immunohistochemical, and ultrastructural features similar to those of cystic thymoma in humans. The perivascular spaces are the source of the cystic spaces. It is essential to differentiate this neoplasm from thymic branchial cysts and thymoma with multilocular cysts. We also describe a case of ectopic thymoma in the pericardial sac.
Footnotes
Acknowledgements
The authors would like to acknowledge the help of Juan Rosai, MD for confirming the diagnoses, Christine MacMurray, MA for editing the manuscript, and Rosemarie Petter for typing the manuscript.