
Abstract
A retrospective study was undertaken to evaluate the long term survival of eight cats with non-lymphoproliferative nasal tumours treated by megavoltage radiotherapy alone. Adenocarcinoma was the most commonly diagnosed tumour. Megavoltage radiotherapy was given to eight cats in 4–6 fractions of 4–8 Gys over a 16 to 28 day period. Seven cats completed the radiotherapy schedule and only two cases developed mild acute radiotherapy side effects. Median survival time after the completion of the radiotherapy course as calculated by Kaplan-Meier survival analysis was 382 days. The 1 year survival rate was 63%. All cats were euthanased because of either a poor response to radiotherapy or recurrence of the nasal tumour. This study demonstrates that a coarse fractionation regime of megavoltage radiotherapy can provide effective long-term palliative treatment for feline nasal tumours. The coarse fractionation schedule has the advantages of requiring only four to six treatments.
Tumours of the sinonasal cavities account for around one to five per cent of all feline neoplasms (Madewell et al 1976, Cox et al 1991). Carcinomas and malignant lymphoma (lymphosarcoma, lymphoma) are more commonly diagnosed with fibrosarcoma and chondrosarcoma less frequently observed (Madewell et al 1976, Cox et al 1991, O'Brien et al 1996). Clinical signs include nasal discharge, sneezing, epistaxis, facial and/or oral deformity, epiphora, stertor, exophthalmos and central neurological signs usually due to expansion of the tumour through the cribiform plate (Straw et al 1986, Smith et al 1989, Cox et al 1991, Theon et al 1994). Whilst clinical signs and diagnostic imaging techniques such as radiography, computer tomography and magnetic resonance imaging maybe highly suggestive of neoplasia, a definitive diagnosis of intranasal neoplasia requires a biopsy (Voges & Ackerman 1995, O'Brien et al 1996, Davidson et al 2000).
Treatment options for feline intranasal neoplasia include surgery (Legendre et al 1975, Cox et al 1991), surgery and megavoltage radiotherapy (Cox et al 1991), megavoltage radiotherapy (Cox et al 1991, Theon et al 1994) and orthovoltage radiotherapy (Lord et al 1982, Theon et al 1994). A large number of studies have evaluated the efficacy of various treatment modalities for canine nasal tumours (Laing & Binnington 1988, Theon et al 1993, Thrall et al 1993, Adams et al 1987). In dogs, surgery, even with post-operative radiotherapy, has not been shown to greatly improve long-term survival compared to radiotherapy alone (Morris et al 1994). Consequently, megavoltage radiotherapy is the most commonly employed technique to treat canine nasal tumours (Davidson et al 2000). However, radiotherapy is often palliative and local recurrence of the tumour is common (Thrall et al 1993, Morris et al 1994). In the cat there have been fewer studies on the efficacy of radiotherapy on non-lymphproliferative neoplasms and there appears to be no clear consensus on the optimum treatment strategy (Straw et al 1986, Evans & Hendrick 1989, Theon et al 1994).
The aim of this study was to assess the long-term survival of cats with nasal tumours that were accurately staged, treated by megavoltage radiotherapy without adjunct chemotherapy and surgery who were all followed-up until euthanasia or death.
Materials and methods
The radiotherapy records of the Queen's Veterinary School Hospital, Cambridge were reviewed from 1990 to 1999. Criteria for inclusion in the retrospective study were:
Complete medical records
Histopathologically diagnosed nasal tumour of non-lymphoproliferative origin
Lateral skull, intraoral and thoracic radiographs taken at the time of diagnosis
Treatment by a coarse fractionation of mega-voltage radiotherapy
Follow-up until euthanasia or death
Eight cats were suitable for inclusion in this study.
Details of each patient's signalment, historical complaints and physical examination were obtained from the medical records written at the time of the initial evaluation of the patient. Six cats were tested for feline leukaemia antigen and feline immunodeficiency antibody.
All cats were treated by megavoltage radiotherapy from a 4 MeV linear accelerator using a coarse fractionation regime. Four patients were placed in sternal recumbency and the radiation beam was angled at 10–15° to the vertical so that it passed obliquely through the frontal sinus and nasal chambers. The four other cats were placed in sternal recumbency and the radiation beam was directed vertically onto the nose. The eyes were protected from the beam by blocks of lead in the latter four cases.
Five cats were treated with an intended protocol of six doses of 6 Gy (one cat received a total dose of 31 Gy) and three cats were treated with four doses of 8 Gy (of which one required euthanasia despite dose modification). The efficacy of the radiotherapy treatment was evaluated in all cases after the final fraction of radiotherapy had been given by clinical examination of the patient and after discussion with the owners about whether the presenting clinical signs had resolved. All cases were followed until euthanasia or death by re-examination and follow-up telephone calls to the referring vets and owners.
Presenting signs of cats with nasal tumours (n = 8)

Statistical methods
The end point of this study was defined as death. Survival time was calculated (in days) from the data of the first radiotherapy treatment to date of death due to tumour. Survival times were drawn with the Kaplan-Meier method. As all animals reached the end point and in all cases death was deemed to be tumour related, no cases were censored in this analysis.
Results
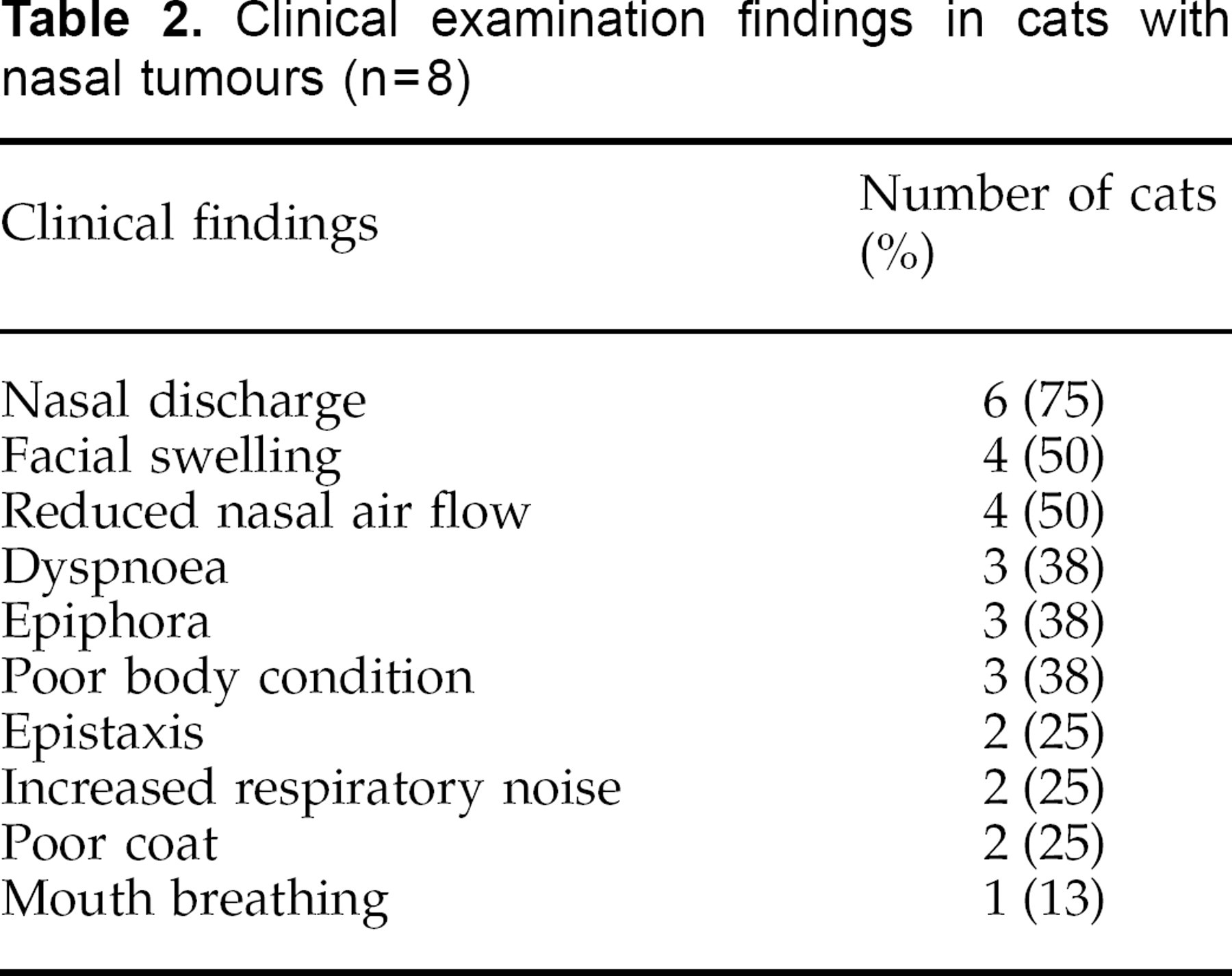
Eight cats met the inclusion criteria of this study. The mean and median age was 12.1 and 12.5 years respectively (range 6 to 17 years). Six cats were domestic short hairs, one was a domestic long hair and the final cat was a Burmese. Five of the eight cats were male. The mean and median interval between the onset of clinical signs and presentation was 4.5 and 3.4 months respectively (range 5 weeks to 11 months). Sneezing, epistaxis, epiphora and nasal discharge were the most common historical complaints (Table 1). The most commonly recorded clinical findings were nasal discharge, reduced nasal air flow and facial swelling. Dyspnoea, epistaxis and poor body condition were also commonly recorded (Table 2). Five cats had been treated with antibiotics which had failed to resolve the clinical signs. Six cats were tested for feline leukaemia virus antigens and feline immunodeficiency virus antibodies. All were negative for both viruses.
Intraoral radiography revealed a soft tissue opacity unilaterally in seven cats and bilaterally in one cat (Table 3). Unilateral loss of nasalturbinate structure was seen in six cats and nasal septum deviation was seen in five cases. Four of the nasal tumours were adenocarcinomas, two were undifferentiated carcinomas, one was a squamous cell carcinoma and one was an osteosarcoma. The submandibular lymph nodes were not palpably enlarged in any of the eight cats.
Clinical examination findings in cats with nasal tumours (n=8)
Radiological findings in cats with nasal tumours (n=8)

One cat was euthanased 48 h after its second fraction of radiotherapy because of persistent vomiting and depression. A post mortem was not undertaken so the exact cause of the cat's sudden decline in health remains unclear. The seven cats which completed the radiotherapy course had no acute side effects apart from anorexia in one case and an increase in the ocular and nasal discharges in a second cat. Over the 3 months following completion of the radiotherapy the clinical signs resolved in one cat, improved but not resolved in four cats, were unchanged in one case and worse in the final cat. No long-term side effects of radiotherapy were observed apart from local alopecia.
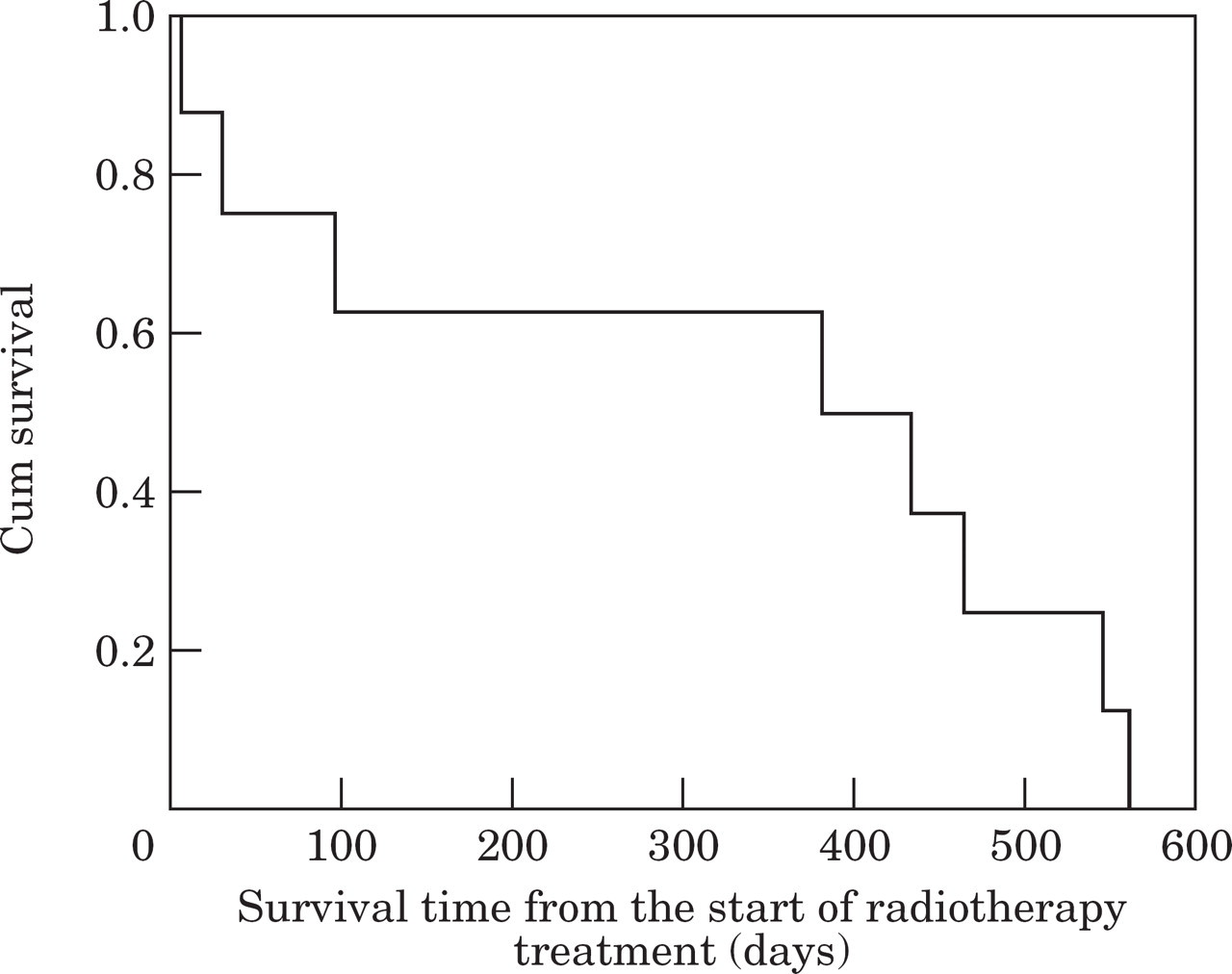
Kaplan-Meier graph of survival from the start of radiotherapy treatment (n=8).
Median survival time after the completion of the radiotherapy course as calculated by Kaplan-Meier survival analysis was 382 days (Fig 1). The mean survival time was 315 days (C.I. 153–477 days). The 1 year survival rate was 62.5 per cent. All cats were eventually euthanased due either to a poor response to radiotherapy or because of recurrence of the nasal tumour.
Discussion
This retrospective study demonstrates that a coarse fractionation regime of megavoltage radiotherapy is an effective palliative treatment for feline non-lymphoid nasal tumours. These results are difficult to compare to the few other studies which have evaluated the efficacy of radiotherapy on feline nasal tumours because of the small number of cases in each study. Three cats with intranasal chondrosarcoma, undifferentiated carcinoma and adenocarcinoma were treated by 9 or 10 fractions of 3.5 to 4 Gy. They had a survival time after the completion of radiotherapy of 6, 41 and 2 months (Straw et al 1986). One case of an intranasal carcinoma which was treated by orthovoltage radiotherapy given over 10 fractions to a total dose of 45 Gy had a survival time of 39.8 months (Evans & Hendrick 1989). Evans & Hendrick (1989) reported on the long-term outcome in five other cats with non-lymphoproliferative nasal tumours. However, additional treatment, including rhinotomy were given in four cases and leukeran and prednisolone in the final case. Four of the cats had survival times of 5.0, 62.3, 5.3 and 20.8 months and one was still alive at follow-up. Cobalt 60 irradiation of an intranasal carcinoma failed to prevent the local extension of the tumour which lead to the euthanasia of the cat 3 weeks after therapy (Cox et al 1991). Partial surgical excision and orthovoltage radiotherapy was used to treat an osteogenic sarcoma of the nasal cavity in a cat resulting in a disease-free interval of 2 years (Lord et al 1982).
The largest study of the efficacy of radiotherapy as a treatment of feline nasal tumours was undertaken by Theon et al (1994). They reported on 16 cats with non-lymphoproliferative intranasal neoplasms which were treated with megavoltage (13 cats) and orthovoltage (three cats). The radiotherapy schedule consisted of a planned radiation dose of 48 Gy given in fractions of 4 Gy over 28 days on a Monday/Wednesday/Friday basis. Two cats also had pre-radiotherapy surgical debulking of the intranasal tumour. The 1 and 2 year survival times were 44.3 per cent and 16.6 per cent respectively. In summary, although comparisons with other studies are difficult, the disease-free intervals achieved by this radiotherapy schedule compare favourably with the few other previous reports.
There are several papers which review the efficacy of radiotherapy on canine intranasal tumours (eg, Adams et al 1987). The survival times for feline nasal tumours are comparable to canine nasal tumours and it appears that both in dogs and cats, local recurrence of the intranasal tumour occurs in the majority of cases (Thrall et al 1993, Theon et al 1994). Surgery and radiotherapy does not appear to improve the survival times significantly when compared to dogs treated by radiotherapy alone (Morris et al 1994). However, the role of chemotherapy as an adjunct to radiotherapy has undergone only limited evaluation (Hahn et al 1992, Lana et al 1997). The role of both surgery and chemotherapy as an adjunct to radiotherapy in the treatment of feline intranasal tumours warrants further investigation. It remains unclear whether orthovoltage or megavoltage is the superior type of radiotherapy for the treatment of feline nasal tumours. The radiotherapy schedule also requires further evaluation to assess which fractionation regime offers the longest disease-free interval with the lowest incidence of acute and long-term radiotherapy side effects. This is the first report of the efficacy of a coarse fractionation schedule of megavoltage radiotherapy on feline nasal tumours. This study demonstrates that a coarse fractionation regime of megavoltage radiotherapy can be successfully used to palliate treat nasal tumours. The coarse fractionation schedule has the advantage of requiring only four to six treatments.
Footnotes
Acknowledgements
Richard Mellanby would like to thank the Alice Noakes Trust for sponsoring his residency. The authors would like to thank all the staff and students at QVSH for the care given to the patients involved in this study. Thanks also to the owners and referring vets for their assistance in providing follow-up information.