
Abstract
A Persian male cat with a history of lower urinary tract disease was presented because of polydipsia, polyuria, constipation and nasal discharge. Ten weeks before admission, the cat had been treated for lower urinary tract disease by catheterisation and flushing of the bladder. The animal was thin, dehydrated, anaemic and azotaemic. Urine culture revealed Aspergillus species cystitis. Antibodies against Aspergillus nidulans were identified in serum. Fluconazole was administered orally (7.5 mg/kg, q 12 h) for 10 consecutive weeks. The azotaemia was resolved, the kidney concentrating ability was recovered and the cat has remained healthy without similar problems.
Fungal infections of the urinary tract are rare in both cats and dogs (Kirkpatrick 1982, Doster et al 1987, Petersen 1988, Lulich & Osborne 1992). There have been some reports on aspergillosis in cats (Pakes et al 1967, Fox et al 1978, Kirkpatrick 1982, Wilkinson et al 1982, Roudebush 1985, Ossent 1987, Fulton & Walker 1992, Wolf 1994, Osborne et al 1995). In most cases, the infection was systemic, involving mainly the lungs and the intestine, and the diagnosis was made postmortem histologically (Pakes et al 1967, Fox et al 1978, Roudebush 1985, Ossent 1987, Davies & Troy 1996). Aspergillus infection has been associated with orbital cellulitis and sinusitis in a cat (Wilkinson et al 1982), and mycotic cystitis caused by A fumigatus has been reported in the bladder of a cat, diagnosed after biopsy (Kirkpatrick 1982).
Aspergillus species are ubiquitous in almost every environment. As they are prodigious spore formers, their spores are present in the air and are almost continuously inhaled and digested (Petersen 1988). In both humans and mammals, aspergillosis is associated with impaired systemic or local host defences (Petersen 1988, Lulich & Osborne 1992). In man, diseases such as leukaemia, aplastic anaemia and leucopenic disorders, as well as prolonged antibiotic and corticosteroid therapy, are considered to increase susceptibility to aspergillosis (Bolton & Brown 1972, Shalev et al 1977, Fox et al 1978, Petersen 1988).
The objective of this paper is to describe, for the first time in English literature, a case of Aspergillus nidulans cystitis and possibly pyelonephritis in a cat, which responded well to fluconazole administration.
Case report
On 8 March 1999, an 8-year-old intact male Persian cat weighing 2.8 kg was referred to the authors' veterinary medical teaching hospital for a second opinion and evaluation. Ten weeks before admission, the cat had been treated for lower urinary tract disease by catheterisation and flushing of the bladder, and was fed with a urine-acidifying commercial diet (c/d feline; Hill's Pet Products). Three weeks before admission, the cat was examined again by the referring veterinarian for symptoms of upper respiratory tract disease (cough, sneezing and nasal discharge). It was treated with amoxicillin trihydrate (Amoxan; Animedica, for 2 days, im), followed by enrofloxacin (Baytril, Bayer, 15 mg, q 24 h, for 5 days, sc) and eventually doxycycline (Ronaxan; Rhone-Merieux, 50 mg, q 24 h, for 10 days, orally), but the symptoms persisted along with polydipsia, polyuria and constipation, which was apparent for the last 3 days.
On admission, the cat was dehydrated and thin. It had lost almost 2 kg of its body weight over the preceding 2 months, and dehydration was estimated at 7%. The rectal temperature, pulse and respiratory rates were 39.1°C, 300 beats/min and 40 breaths/min, respectively. The mucous membranes were pale and the coat was dull and easily epilated. Routine laboratory evaluation at admission (day 1 of hospitalisation) revealed normocytic, normochromic anaemia (PCV 21.9%, normal range: 24–45%), azotaemia (BUN 60 mg/dl, normal range: 13–39 mg/dl; creatinine 2.8 mg/dl, normal range: 1.2–1.9 mg/dl), hypoglycaemia (70 mg/dl, normal range 80–141 mg/dl) and hyperphosphataemia (12 mg/dl, normal range: 2.2–6.3 mg/dl). Urinalysis of a specimen obtained by cystocentesis included isosthenuria (specific gravity 1·012), aciduria (pH 6), pyuria (leukocytes <100/HPF), yeast buds and hyphae (Fig 1). The hyphae consisted of numerous dichotomous branching, hyalin-like, septate hyphae, that were 2–5 μm wide and oriented in the same direction. These features are characteristic of Aspergillus species (Emmons et al 1964, Petersen 1988). Fungal cystitis was diagnosed. Low urine specific gravity with concurrent polydipsia, polyuria and dehydration were indicative of renal dysfunction. Aspergillus species was isolated in pure culture from a urine sample obtained by cystocentesis on day 2 of hospitalisation. The culture was made in a Sabourauds dextrose agar plate, which was incubated at 28°C for up to 5 days. Green/brown red colour colonies were noticed. An impression smear stained with Giemsa stain revealed the typical Aspergillus species morphology. Findings from thoracic and abdominal radiography, as well as ultrasound examination of the kidneys, revealed no evidence of visceral or pulmonary involvement. A test for feline leukaemia and feline immunodeficiency virus infection (Combo test, IDEXX) was negative. Cytologic examination of the nasal discharge was negative for fungi, as was the blood culture. Serum examined for antibodies against Aspergillus species was positive for A nidulans and thus the A nidulans cystitis and possibly pyelonephritis were diagnosed. For the detection of antibodies against A nidulans, the gel diffusion precipitation test (GDPT) was used (Heska UK Limited, Devon). For this purpose, antigens of A flavus, A niger, A nidulans and A terrens were reconstituted with 1 ml deionised water. The antigens were stored at 4°C before and after reconstitution. For gel preparation, sodium chloride, phenol, 1N sodium hydroxide, 1 N HCl and OXOID agar no. 1 were used. When soluble antigens and homologous antibodies are placed in adjacent wells, they cut into a suitable diffusion media and they will diffuse towards one another and produce a visible precipitation line.
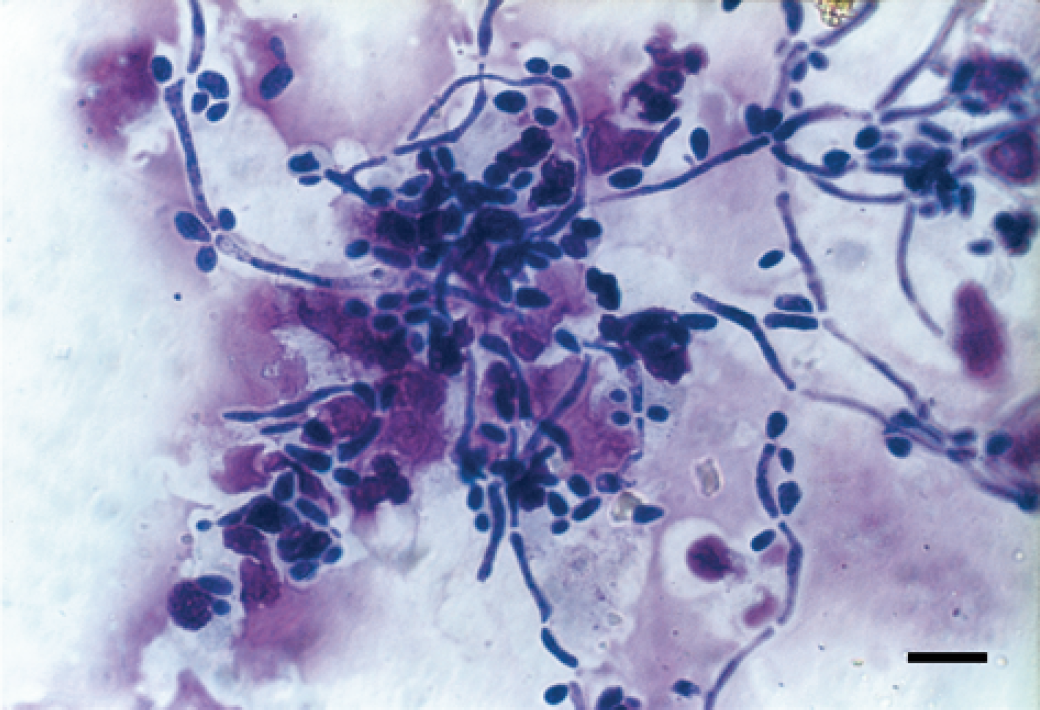
Photomicrograph of Giemsa-stained urine sediment of a cat depicting a large number of yeast forms and hyphae. Dichotomous, branching, septate organisms characteristic of Aspergillus species are seen (bar=7 μm).
Treatment and outcome
Intravenous fluids were initiated with lactated Ringer's and 35% dextrose at a ratio of 9:1 (16 ml/h reduced to 10 ml/h on day 2) along with antibiotics [amoxycillin (Amoxil); Smith-Kline Beecham, 400 mg, q 24 h] for 3 consecutive days. Also administered were aluminum hydroxide (Pepsamar; Sterling Health, 130 mg, q 12 h, orally) in order to treat hyperphosphataemia, and cisapride (Alimix; Janssen-Cilag, 2.5 mg, q 12 h, orally) for constipation.
On day 4, fluconazole (Fungistatin; Pfizer, 7.5 mg/kg, q 12 h, orally) was administered. A CBC count revealed a normocytic, normochromic non-regenerative anaemia (PCV 19%, Hb 6.3 g/dl, reticulocyte count 0.27), moderate leucocytosis (21,800/μl) and neutrophilia (14,388/μl) with a regenerative left shift (bands 3988/μl). Laboratory results indicated azotaemia (BUN 56 mg/dl, creatinine 2.6 mg/dl) and hyperphosphataemia (11 mg/dl).
On day 5, the cat was released. The owner was instructed to administer fluconazole (7.5 mg/kg, q 12 h, orally) and aluminum hydroxide (130 mg, q 12 h, orally) until re-examination. Enrofloxacin (25 mg, q 12 h, orally) was also prescribed for 15 days and the cat was placed under a diet for renal failure (k/d feline; Hill's Pet Products).
The cat was re-examined 6 weeks after discharge. It weighed 3.3 kg and its PCV was 22%. Results of serum BUN, creatinine and phosphorus were within normal limits. The urinalysis of a specimen obtained with cystocentesis revealed that the urine specific gravity was 1·024. The urine culture for fungi was negative. A third urine culture for bacteria and fungi was performed 15 days later and it was also negative. The fluconazole was discontinued 15 days after the third urine culture. The animal's body weight returned to 5 kg and the owner reported that the cat was healthy 16 months after discharge without any similar problem.
Discussion
Risk factors predisposing to aspergillus urinary tract infections in the cat are thought to be diabetes mellitus, antibacterial therapy, uroliths, urine stasis or obstruction, indwelling urinary catheters (Kirkpatrick 1982, Doster et al 1987, Petersen 1988, Fulton & Walker 1992, Lulich & Osborne 1992) and aciduria (pH 5.1–6.4) (Osborne et al 1995). Although feline immunodeficiency virus and feline leukaemia virus infections, due to their immunosuppressive effects (Wilkinson et al 1982, Petersen 1988, Fulton & Walker 1992), were found to be the predisposing diseases in other cases (Petersen 1988, Lulich & Osborne 1992), it was not evident in this cat. According to the case history and clinical data, the urine obstruction and stasis, the use of indwelling urinary catheters, the long-term administration of several antibiotics and perhaps the aciduria predisposed this cat to A nidulans cystitis (Petersen 1988, Fulton & Walker 1992, Lulich & Osborne 1992). The most probable route of A nidulans infection was thought to be through urethral catheterisation. Moreover, fungal pyelonephritis, although strongly suspected, cannot be confirmed or excluded from these findings. A kidney biopsy might have helped but the owner declined to have this performed. On the contrary, renal dysfunction could have been due to the complication of preceding lower urinary tract infection or other unrelated reasons (Kirkpatrick 1982, Petersen 1988, Fulton & Walker 1992, Lulich & Osborne 1992). Nevertheless, the resultant normal renal function 6 weeks after fluconazole administration is strongly suggestive for A nidulans pyelonephritis that had undergone remission. In addition, aspergillus rhinitis cannot be excluded from the negative results of nasal discharge cytology examination alone. It is well known that the diagnosis is confirmed by the combination of nasal discharge culture, nasal mucosa biopsy and detection of serum antibody titre results (Van Cutsem & Rochette 1991). Although chronicity and persistence despite antibacterial therapy might have been indicative of fungal rhinitis, it is postulated that several bacterial or viral conditions in the cat could have the same biologic behaviour (Petersen 1988, Van Cutsem & Rochette 1991).
Aspergillus organisms found in urine indicate either sample contamination or infection of the urinary tract. In healthy animals, urine fungi are not detected. Fungi detected in an asymptomatic animal, when urine samples are properly collected, are thought to be abnormal (Osborne et al 1995). When the presence of fungi is determined by urinalysis, the samples ought to be taken by cystocentesis and a culture should be performed so that an accurate diagnosis can be made (Kirkpatrick 1982, Petersen 1988, Fulton & Walker 1992, Lulich & Osborne 1992).
Treatment of A nidulans cystitis involved the administration of an antifungal agent and the initial supportive therapy of the concurrent renal dysfunction. Due to the poor nutritional state of this cat, it was imperative that an antifungal agent was administrated (Fulton & Walker 1992, Lulich & Osborne 1992, Wolf 1994). In this case, fluconazole was selected because it is highly water-soluble and only weakly protein-bound, and thus highly concentrated in all body tissues (Wolf 1994). It appears to be the superior choice for the treatment of mycotic infections of the urinary tract. Fluconazole is usually considered to have greatest efficacy against yeasts and is not always a good choice for filamentous fungi; although it worked well in this case (possibly because of high concentrations obtained in urine), it may not be effective in all cases involving filamented fungi. Moreover, it has minor adverse effects (Wolf 1994), a vital criterion in the present case, considering the poor status of the animal. Some authors believe that alkalinisation of the urine is restrictive for the growth of fungi (Fulton & Walker 1992, Lulich & Osborne 1992), but in this case, the cystitis resolved successfully without its usage. The duration of the drug administration must be prolonged, and should be discontinued 15 days after two consecutive negative urine culture results (Osborne et al 1995).
As proved in this case, A nidulans, although ubiquitous, can cause fungal infection. The treatment of feline lower urinary tract disease represents significant predisposing factors for fungal infections (Osborne et al 1995). Thus, when lower urinary tract disease persists, the clinician has to suspect a possible fungal infection, because the incidence of mycoses appears to increase (Ossent 1987). This cat responded well to the antifungal agent selected. Fluconazole may be a relatively safe drug with good results against aspergillosis of the urinary tract.