
Abstract
One of the most frequent motivations for seeking veterinary attention for a cat is when the owner recognises a loss of normal appetite in his pet. The medical term for a lack of appetite for food is ‘anorexia’, and it may be partial or complete. While anorexia is a common manifestation of disease, the mechanisms underlying decreased food intake are complex and not completely understood. The regulation of appetite involves interaction of external stimuli with signals from the gastrointestinal tract and central nervous system. Aberrations in any of the internal control systems for hunger and satiety, or changes in external factors such as diet or feeding environment, can result in partial or total anorexia. The challenge for the practitioner is not only to diagnose and treat the underlying condition, but to recognise at what point inadequate food intake has or will impinge on the patient's nutritional status to the extent that it might deleteriously affect clinical outcome. It is also important to bear in mind the significance that the patient's appetite and food intake has for the cat owner in his overall perception of his pet's condition and quality of life.
The regulation of food intake
In simplistic terms, satiety is associated with the absorptive state and hunger is associated with the post-absorptive state. Plasma concentrations of amino acids, glucose and fatty acids will modulate the secretion of various hormones that act centrally and possibly peripherally via the gastrointestinal tract to stimulate or control appetite. Some nutrients may also act directly on receptors in the central nervous system (CNS) including centres in the hypothalamus that have been shown to regulate hunger (lateral hypothalamus) and satiety (ventromedial hypothalamus) (Anand & Brobeck 1951). A number of hormones released in response to the digestion and absorption of a meal (eg, insulin, cholecystokinin) stimulate satiety while others released in the fasting state (eg, corticosteroids) are known to stimulate appetite. Leptin, a recently identified peptide, is synthesised by adipose tissue and is believed to play a role in maintaining nutrient reserves through a feedback mechanism on satiety centres in the CNS. Leptin has been measured in cats and feline plasma levels are correlated with adipose tissue mass (Appleton 2000).
Distension of the gastrointestinal tract, in particular the stomach and duodenum, signals satiety, while the nutrient content of the ingesta appears to be the more important stimulus for cessation of intake at the level of the small intestine (Smith 1999). Psychological state, learned behaviours, circadian rhythm and external factors such as the patient's environment also have significant influence on food intake, even to the extent that they may over-ride physiological signals governing appetite.
A meal can be thought of as having three distinct phases: initiation, maintenance and termination. To some extent, different stimuli and mechanisms are involved in each phase. The initiation phase, while clearly influenced by internal hunger signals, is also strongly influenced by external stimuli. These stimuli include visual, olfactory, tactile and auditory stimuli associated with food. Meal termination is primarily influenced by post-ingestional stimuli such as gastric distension or nutrient absorption. Once initiated, the size of a meal will be determined by the mechanisms that maintain and terminate eating. These mechanisms involve a balance between positive and negative feedback. For example, a particularly palatable food may provide, via orosensory stimuli, positive feedback that will over-ride the negative feedback activated by ingested food via gastric distension and the release of satiety-inducing hormones.
It is useful to have an understanding of what aspects of food influence palatability and acceptance from the feline standpoint. Studies of the flavour preferences of cats have found that while cats show very little interest in ingredients with sweet flavours, foods that are, or have been, acidified have a strong appeal (Beauchamp et al 1977, Boudreau & White 1978). Cats also respond to certain amino acids, peptides and nucleotides that, when perceived at all by humans, taste bitter or acidic (Boudreau & White 1978). In recognition of these aspects of feline tastes, many commercial cat foods contain digest (enzymatically digested animal tissues) as flavour enhancers or, in the case of dry foods, the kibbles are coated with digest or acidic compounds. In addition to taste, aroma is a significant component of palatability for humans, and given that the feline olfactory system is considerably more developed than the human system it is likely that scent is a very important aspect of food appeal for cats (Dodd & Squirrell 1980). Finally, the nutrient content of the diet will also have an impact on palatability. Generally speaking, increasing moisture content improves palatability. Similar trends are seen for increasing the protein or fat content of a diet (Macy & Ralston 1989).
One extremely significant factor influencing dietary preference in cats is food texture or what is referred to as ‘mouth feel’. In general cats do not care for sticky foods or foods that are ground to small particles or powders (Kane et al 1987). The pet food industry has invested a fair amount of research into finding out what types of shapes and textures are appealing to cats. Dry cat foods come in many shapes and sizes, and canned cat foods are being increasingly marketed in a variety of textures including flaked, sliced and chunky, in addition to the traditional ground consistency. It is important to recognise that not only a change in the form of diet (canned vs dry) but a more subtle change in kibble shape or food consistency could have a profound impact on a cat's acceptance of a new food.
To some extent, what a given cat finds acceptable as a diet depends on past experience (Kane 1989). Cats are known for a tendency to form fixed food preferences and therefore may refuse a novel food item in the face of internal stimuli that would normally elicit food intake. It is important to bear this in mind when circumstances warrant dietary change for diagnostic or therapeutic purposes. The acceptance of food is also influenced not only by what type of food the cat is used to eating, but also by the environment in which the cat is used to being fed. This includes the timing and location of meals, the type of bowl or dish the food is offered in, and social stimuli such as the presence or absence of other household members and pets.
Pathophysiology of anorexia
From the preceding discussion of the mechanisms involved in the regulation of food intake, it should be clear that anorexia can result when circumstances interfere with the initiation of food intake, or act to promote negative stimuli during a meal so that food intake is terminated. Changes in the diet, feeding environment or psychological state of the patient may be at least partly involved.
Anorexia is also one of the more common systemic effects of conditions such as uraemia, neoplasia, diabetic ketoacidosis and conditions resulting in inflammation and fever. Anorexia in such circumstances may be secondary to the effects of circulating mediators, such as hormones or cytokines (tumour necrosis factor-α, interleukin-1, interferon), on appetite and satiety centres in the CNS. Abdominal tumours or organomegaly can limit gastrointestinal distension and lead to cessation of intake. Conditions resulting in chronic pain are often associated with a reduction in appetite.
Anorexia is also common with diseases of the gastrointestinal tract and liver, and is often the principal clinical sign in cats with inflammatory bowel disease or pancreatitis. Cats suffering from dyspnoea secondary to cardiac disease or respiratory disorders will also often exhibit reduced food intake. Anorexia, nausea and vomiting can be seen with the use of certain drugs including many chemotherapeutic agents and antibiotics (Table 1). In many cases, the effects of these drugs are mediated by the chemoreceptor trigger zone in the CNS. The chemoreceptor trigger zone also plays a role in some of the clinical signs associated with metabolic disturbances such as uraemia. Diseases that impair olfaction or might alter perception of odours or tastes could have an impact on food intake. Human patients with certain endocrinopathies or forms of neoplasia report altered senses of smell or taste (Mattes 1999). Finally, with conditions where patients experience adverse sensations in association with food consumption such as pain or nausea, anorexia is to be expected.
Medications which may cause anorexia, nausea or vomiting in cats

One very important potential outcome of the unpleasant side effects of the underlying disease, and in some cases the treatment, is that the patient may associate the nausea, the indisposition or the pain with the act of eating or even the sight or scent of food. This is called learned food aversion and is a well-recognised phenomenon in human patients. Everyone has experienced an occasion when they have become ill after eating a particular food. Whether or not that food was responsible for the illness, it becomes associated with the illness in our minds. This association can linger long after the underlying illness has resolved. Although it is difficult to prove that cats develop food aversions, there is indirect evidence that they do. In an investigation of feline hepatic lipidosis, cats that developed clinical signs of hepatic lipidosis after a prolonged fast recovered spontaneous appetite sooner when they were tube fed exclusively after diagnosis, than cats that were first offered food and were subsequently tube fed because they would not eat consistently (Biourge 1997). The speculation is that the cats that were offered food became nauseous or otherwise indisposed after eating, and associated those feelings with voluntary food intake. Therefore, one of the greatest challenges of feeding the anorectic cat may be avoiding the development of learned food aversion or dealing with this condition when it does occur.
Diagnostic work-up
Due to the many pathological conditions that can result in anorexia, it is important to do a thorough work-up to pinpoint the underlying cause in an individual patient. Perhaps the most critical step is to obtain a comprehensive medical and dietary history, paying particular attention to any changes in the patient's diet and household environment including routine and occupants. This approach will aid in differentiating between anorexia resulting directly from a dietary change or other external factors, and anorexia secondary to an underlying physical condition. In cases of suspected partial anorexia, it is useful to quantitate just how much food the patient is consuming. This calorie count should be compared to the patient's predicted maintenance energy requirement (MER). One common formula for predicting MER for cats is 60 × Wt (kg) (National Research Council 1986). Remember when using this formula for overweight cats to use an approximation of lean body weight. This is because the excess adipose tissue does not contribute a significant amount to the cat's energy needs, so using the actual body weight will result in an over-prediction of MER.
Do a thorough oral, dental and cranial examination. Try to evaluate the patient's ability to smell and to swallow. Look for evidence of systemic disease or conditions associated with chronic pain. Further diagnostic work-up will be dictated by the history and findings on physical examination; however, if the history is vague and no significant physical abnormalities are found, a minimum database should be performed. This should include serum chemistry, a complete blood count, tests for FIV and FeLV, and a urinalysis. Further work-up may be indicated including thoracic and abdominal radiography, ultrasonography and gastrointestinal endoscopy.
Therapeutic approach
The goals for managing the anorectic cat are to treat the underlying disease while providing supportive care. Supportive care that addresses problems involving hydration and electrolyte status, pain, body temperature, vitamin B deficiencies and nausea will result in normal appetite being re-established in many patients.
As one has to guess what a cat is experiencing when it refuses food, it can be very hard to judge how best to proceed. On the one hand, efforts can be made at coax feeding a pet with palatable or novel food items, with the hope of finding something that will be eaten voluntarily. On the other hand, it might be best to back off and rely on assisted-feeding techniques such as tube feeding, or to not feed at all for a time, because of the risk of causing or exacerbating a learned food aversion. Just how long it is safe to withhold food from a cat depends upon a number of factors, including the patient's nutritional status and body condition. The typical recommendation is to initiate assisted feeding within 3–5 days of cessation of food intake. However, in the case of a severely malnourished cat or a cat exhibiting clinical signs consistent with idiopathic hepatic lipidosis, assisted feeing should be initiated as soon as safely possible.
It is probably best to resist the temptation to coax a cat to eat when it is showing overt signs of nausea and discomfort. Cats that gulp or drool at the sight or scent of food, who turn their heads away from the food, spit it out when it is put in their months, or try to get as far away from the food as possible should be left alone. Pushing food on a patient who clearly does not want it may risk inducing a learned food aversion.
For cats that are showing some interest in food, there are many things that can be tried to increase their inclination to eat. While it is true that cats are strongly influenced by habit in their selection of foods, if a learned food aversion has developed it is reasonable to try novel food items. The assumption is that the cat has begun to associate a previously favourite food with unpleasant sensations, so perhaps introducing a very different type of food can overcome the aversion to eating. This can backfire if the patient is still unwell since it is very possible that the cat will simply transfer the aversion to the new food. Any type of food can be used including meat-based baby foods and palatable table foods. Although these types of foods will not provide all of the nutrients that a cat needs, calories are the most important over the short term (2–3 weeks). If necessary, a balanced diet can be built around the preferred foods for longer term feeding. Also bear in mind that baby foods containing onion powder have been proven to cause Heinz body anaemia in cats (Robertson et al 1998).
One can try offering food in a novel setting or have someone different do the feeding. Sometimes an animal will associate its surroundings with past unpleasant experiences. Make mealtimes as comfortable and unstressful as possible. Try to offer food in a quiet setting. Try not to schedule feedings at a time that involves other treatments such as pilling. Avoid pushing food on the pet. However, sometimes a cat will be stimulated to eat if a small amount of food is placed in the mouth or on the lips or paws. Stroking and talking to a cat with the food nearby often will stimulate interest and intake. Early satiety (premature termination of a meal) is common in anorectic patients, so divide the day's food up into as many small fresh meals as possible. Feed in wide shallow bowls or flat dishes so the cat's whiskers are not interfered with during eating.
It is important to keep in mind that ‘mouth feel’ is very important to cats, and something as simple as an unfamiliar kibble shape may be responsible for a cat's inappetence. Remember that the nutrients that increase palatability for most cats are moisture, fat and protein, and that cats prefer foods with an acidic flavour and strong aromas. Adding water to a dry cat food or switching to a canned food may improve food acceptance. It should be noted that trying foods with increased fat or protein content should be done with consideration of the patient's tolerance of these nutrients. Cats with kidney or liver dysfunction may not tolerate high protein intake, and cats with some types of gastrointestinal disease cannot tolerate large amounts of dietary fat.
The standard advice for getting anorectic pets to eat has been to warm the food to just below body temperature. This is believed to increase the aroma of the food, which in turn will enhance the palatability. However, this practice has been found to be counterproductive in some human patients with acquired food aversion, as an association has been made between certain smells or flavours and feeling unwell. In some cases, food chilled from the refrigerator is more acceptable to these patients since is has less aroma and flavour. Therefore, with cats showing interest in food but an unwillingness to eat one might try offering chilled food.
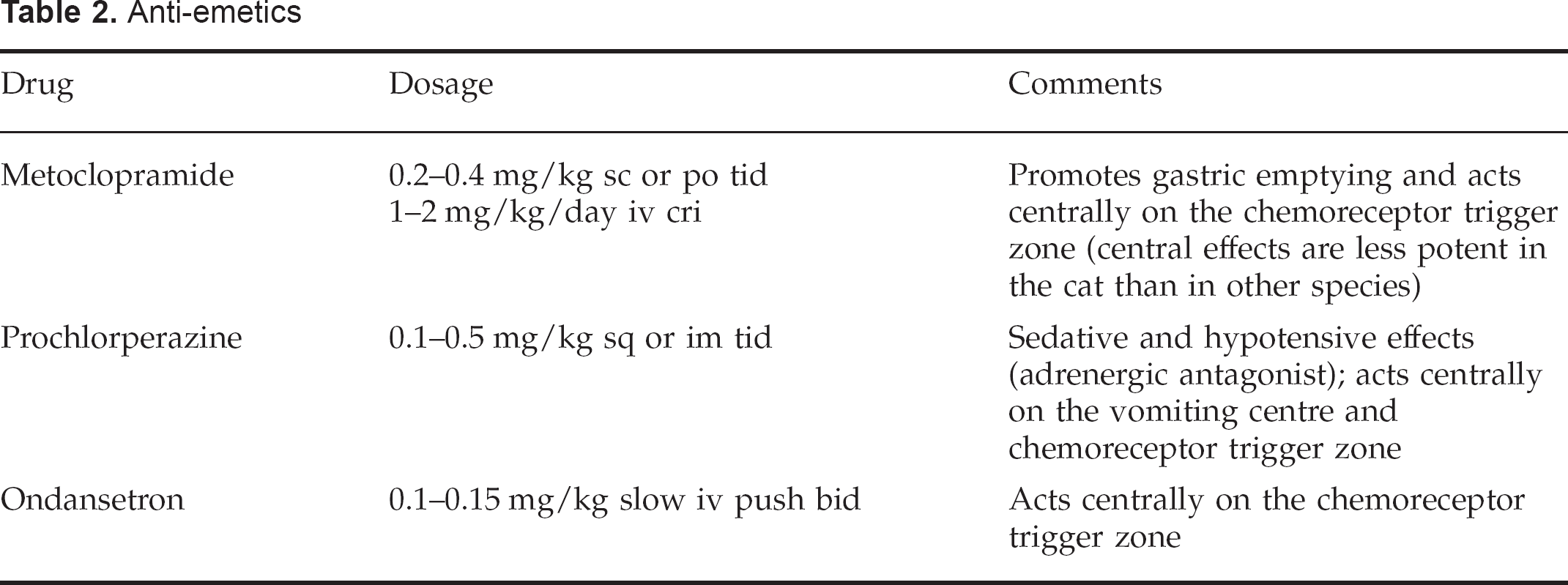
Every patient will be different and it will be necessary to try and read any clues that a patient may give by its behaviour around food in order to determine how best to proceed. The use of anti-emetic drugs should be considered in cats where vomiting and nausea are a problem (Table 2). Metoclopramide, in addition to having some anti-emetic effects, may be beneficial in patients where delayed gastric emptying is a problem.
Anti-emetics
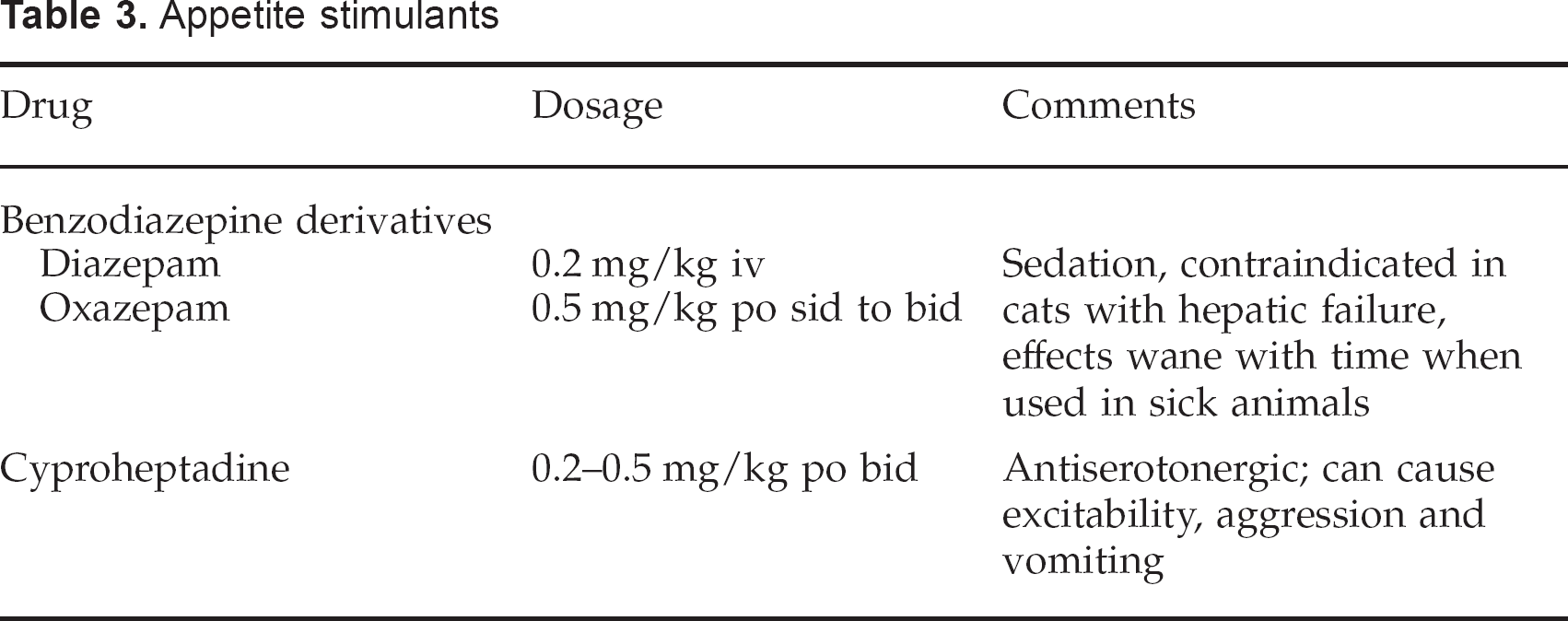
There are a few drugs that have been used to stimulate appetite in feline patients (Table 3). There are a number of adverse effects associated with these medications and they generally only stimulate a momentary increase in appetite. Therefore, these drugs are unreliable for ensuring resumption of adequate food intake, and perhaps they are better thought of as an aid for helping patients get over learned food aversion once they are convalescent rather than as a panacea for anorexia.
Appetite stimulants
For the cat that is not a good candidate for coax feeding, regardless of the reason, the use of tube or parenteral feeding should be a consideration. This is especially important with obese cats that are believed to be at increased risk of developing idiopathic hepatic lipidosis. Furthermore, coax feeding is very time consuming and labour intensive, so it is problematic to sustain that level of nursing care for more than a few days. It is beyond the scope of this review to detail the many methods available for providing assisted feeding in feline patients. However, the decision to initiate assisted feeding should balance the potential risks of whatever method is chosen with the potential benefits to the patient. The patient's duration of anorexia, nutritional status, underlying condition and prognosis should be taken into consideration. Ultimately, it is a question of whether any further deterioration in nutritional status will have a significant impact on the patient's clinical outcome. If it is suspected that this will be the case, it is important to get the patient on an adequate and consistent plane of nutrition.
Finally, one last issue involving the anorectic feline patient is the perception that the cat's owner has of his pet's condition and quality of life. Food and the act of eating are of fundamental and universal significance. The pet owners may not have a grasp of their cat's condition or how it is being treated; however, they do understand food and the importance of proper nourishment. Therefore, a pet's lack of appetite can be particularly distressing and often perceived as evidence that the pet is suffering. By addressing a cat's anorexia, the practitioner will, in addition to maintaining the patient's nutritional status and, in all likelihood, diagnosing and treating the primary disease, reassure the owner with regard to some of his most basic concerns and fears for his pet.