
Abstract
A peri-parturient fifteen-month-old female Maine Coon cat was presented with extreme weakness and depression, profound hypovolaemia and hypothermia. Severe hyperkalaemia, hyponatraemia and anaemia were detected. Disseminated intravascular coagulation was suspected due to marked prolongation of activated partial thromboplastin time. Uterine torsion was diagnosed at exploratory laparotomy. The cat made a full recovery following ovariohysterectomy and intensive supportive therapy.
Uterine torsion is an uncommon complication of pregnancy in the cat. Fifteen cases have been reported in the veterinary literature with a successful outcome following ovariohysterectomy in 12 out of 15 cases (Freeman 1988). This report describes the successful management of uterine torsion in a cat with severe metabolic and haemostatic abnormalities.
A fifteen-month-old female, full-term Maine Coon cat, weighing 7.2 kg, was referred to the University of Edinburgh Hospital for Small Animals with a 6-h history of weakness and ataxia. There had been no signs of impending parturition other than a mild reduction in appetite over the preceding 24 h. Initial laboratory investigation by the referring veterinary surgeon had revealed marked anaemia and leucocytosis. Platelets were mildly reduced. Serum biochemical abnormalities included marked elevation in alanine transferase (ALT), hyperphosphataemia, hyperkalaemia, hyponatraemia, a mild elevation in urea, and mild hypoproteinaemia. Abdominal radiography revealed the presence of a gravid uterus (seven kittens in total) with one foetus engaged in the pelvic canal. There was no radiographical evidence of foetal death. Intravenous fluid therapy had been initiated with 0.18% sodium chloride and 4% glucose (Aquapharm No 18; Animalcare).
On arrival presentation the cat was extremely depressed and unresponsive. Rectal temperature was markedly subnormal at 35.2°C. Femoral pulse quality was poor and the extremities were cold, consistent with hypovolaemic shock. Oral mucous membranes were very pale. Cardiac auscultation revealed a heart rate of 160 beats per min with occasional ectopic beats. The abdomen was grossly distended consistent with full-term gestation. There was a blood-tinged vulval discharge and an amniotic sac was visible within the vagina.
On elecrocardiography the heart rate varied between 139–159 beats per min. An absence of p-waves may have been due to hyperkalaemia, although the rate is relatively high for atrial standstill. Intermittent ventricular premature complexes were also observed. Ultrasonographic examination of the abdomen revealed a gravid uterus with multiple foetuses. A small amount of free abdominal fluid was also detected. Foetal heart movements were not observed.
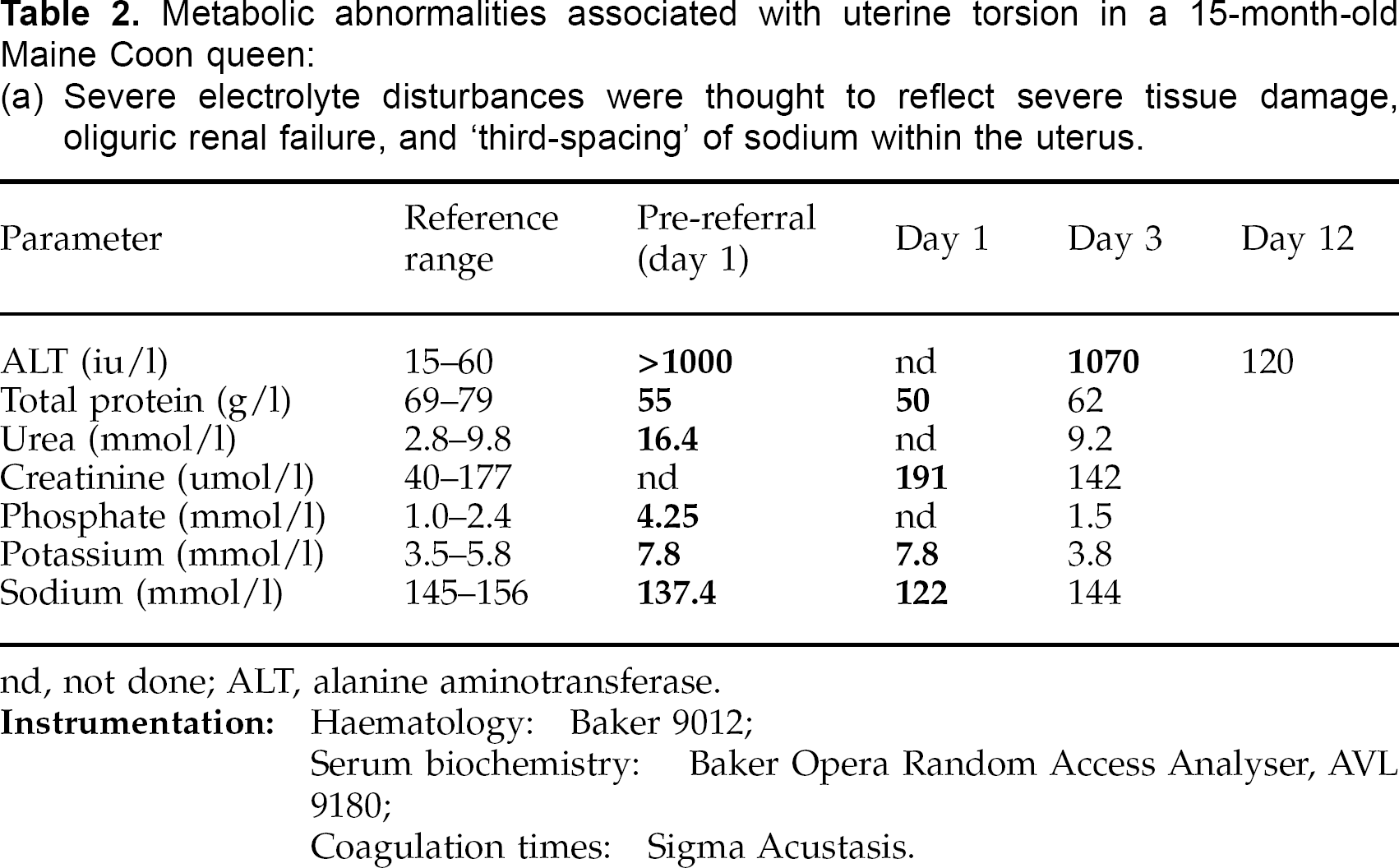
Further laboratory evaluation of the blood (Table 1) confirmed the presence of severe, mildly regenerative anaemia, with a total erythrocyte count of 1.6 × 1012/l (PCV 9%), absolute reticulocyte count of 64 × 109/l, and 0.24 × 109/l circulating normoblasts. Leucocyte parameters were consistent with an inflammatory response, with a mature neutrophilia (27.1 × 109/l) and mild left-shift (1.8 × 109/l band neutrophils). Platelet count and prothrombin time (PT) were normal, however, activated partial thromboplastin time (APTT) was markedly prolonged at 79.4 s (normal range 14–25 s). Electrolyte imbalances were still present (Table 2), with a serum potassium of 7.8 mmol/l and sodium of 122 mmol/l at admission. Initial urine specific gravity was 1.076 consistent with hypovolaemia.
Haematological findings in a 15-month-old Maine Coon queen with severe haemostatic complications associated with uterine torsion (bold type indicates abnormal values):
Prolongation of APTT was supportive of DIC; Neutrophilia was indicative of an inflammatory response. The leucocyte values have been corrected for 8% circulating normoblasts on day 1; Severe, mildly regenerative anaemia on day 1, followed by marked regeneration by day 3, was consistent with acute blood loss; Thrombocytopenia was encountered on day 3. Platelet clumping was not observed on examination of a blood smear.
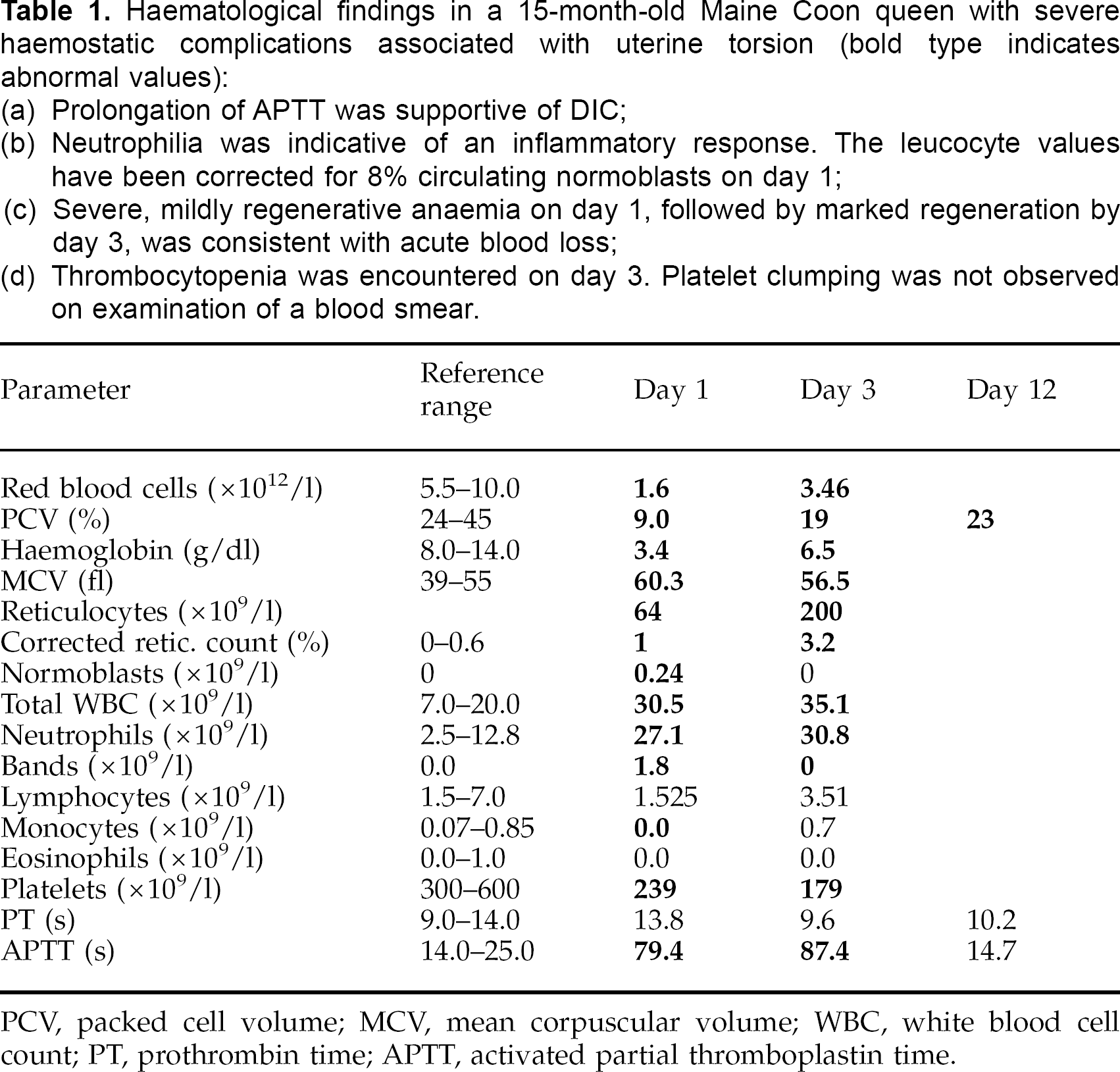
PCV, packed cell volume; MCV, mean corpuscular volume; WBC, white blood cell count; PT, prothrombin time; APTT, activated partial thromboplastin time.
Metabolic abnormalities associated with uterine torsion in a 15-month-old Maine Coon queen:
Severe electrolyte disturbances were thought to reflect severe tissue damage, oliguric renal failure, and ‘third-spacing’ of sodium within the uterus.
The cat was treated initially with the administration of 50 ml of whole blood (type A, as determined by Rapid Vet™-H; dms laboratories), 0.9% sodium chloride with 5% glucose (Intraven®; GRL Ltd) and colloid (Gelofusine®; Braun Medical Ltd). Cefazolin (Kefzol; Lilly) was given at a dose of 20 mg/kg. The urinary bladder was catheterised to monitor urine output, which was negligible despite fluid therapy. Serum potassium levels continued to increase (to 8.2 mmol/l), and hyponatraemia worsened (117 mmol/l).
Anaesthesia was induced with intravenous propofol (Rapinovet™; Schering-Plough Animal Health) and maintained with isoflurane (Isoflurane-RM®; Rhone Merieux) in oxygen and nitrous oxide, administered via endotracheal intubation and a non-rebreathing system. Morphine was administered intravenously at a dose of 100 ug/kg.
A ventral midline coeliotomy was performed, revealing the presence of a gravid uterus with a 540° torsion of the left uterine horn along its longitudinal axis (Fig 1). The affected section of uterus was grossly distended and ischaemic. One foetus was engaged in the pelvic canal. A ventral midline incision was made into the body of the uterus to remove the engaged foetus. An ovariohysterectomy was then performed using a standard technique. The torsion was not corrected at the time of surgery All kittens were confirmed dead. The abdomen was extensively lavaged with 0.9% sterile saline and a standard closure of the midline was performed. A further 30 ml of type A whole blood was administered during surgery.

540° torsion of the left horn of a gravid uterus. A ventral midline incision into the uterine body was required to disengage one kitten (pictured) from the pelvic canal prior to ovariohysterectomy.
The cat was placed in the intensive care unit post-operatively. Fluid therapy was continued with 0.9% sodium chloride with 5% glucose at 20 ml/h until adequate urine output resumed (approximately 2 h post-operatively). Laboratory evaluation of blood 6 h post-operatively revealed a PCV of 20%, with total protein 55 g/l, and normalisation of serum electrolytes. Fluid therapy was changed to compound sodium lactate solution (Isolec; Ivex Pharmaceuticals) administered at a rate of 12 ml/h. Twelve hours after surgery the cat was bright and alert and eating. Cephalexin (Ceporex™; Schering-Plough Animal Health) was continued orally for 7 days post-operatively. The cat made an uneventful recovery from surgery.
Gross inspection of the uterus revealed marked distension of the affected horn, with a grossly distended, thrombosed vein within the mesosalpinx. The distension was due, in part, to a large quantity of altered blood. Histopathological examination of the uterus revealed vascular congestion and oedema through all layers of the uterine wall, with early thrombosis formation of the mural veins. The uterine mucosa was largely absent or necrotic where present. No bacteria were cultured from uterine fluid.
Further laboratory evaluation of blood 48 h post-operatively (Table 1) indicated an appropriate regenerative response to the anaemia (RBC 3.46 × 1012/l), with a reticulocyte count of 200 × 109/l. Activated partial thromboplastin time (APTT) was still markedly prolonged at 87.4 s, with normal PT. Platelet count was mildly reduced at 179 × 109/l. Re-evaluation of clotting times 10 days later revealed normalisation of APTT, at 14.7 s (Table 1). Alanine transferase had also returned to normal. Evaluation of factors XII, XI, IX and VIII, using a standard fibrometer, found them all to be within normal limits, at greater than 100%. This excluded the possibility of a pre-existing coagulation factor deficiency.
Uterine torsion occurs uncommonly in the cat and the aetiology has not been established. Proposed contributing factors include excessive foetal movement, uterine contraction, rough handling during pregnancy, lack of tone in the pregnant uterus, lack of foetal fluids and previous stretching of the broad ligament in multiparous individuals (Biller & Haibel 1987). Previous reports have involved torsion of one or both uterine horns, with the degree of torsion ranging from 180° to 900° (Freeman 1988). In this case it was thought that dystocia, probably arising from a relative foeto-maternal disproportion and uterine inertia, had resulted in the uterine torsion.
Compromise of the uterine vasculature, as a consequence of uterine torsion, was demonstrated on gross and histopathological examination of the uterus. The associated necrosis of uterine tissue and placental detachment are thought to have been responsible for the various metabolic and haematological derangements documented in this case. Hyperkalaemia was thought to have arisen from a combination of massive tissue breakdown and reduced renal excretion of potassium due to oliguria (Dibartola & Autran de Morais 1992). In the absence of excessive renal loss, hyponatraemia was most likely to be due to ‘third-spacing’ of sodium within the uterus. Intracellular redistribution of water, as a consequence of rapid onset hyponatraemia, may have been responsible, in part, for the depression seen in this case (DiBartola 1992). Ovariohysterectomy and re-establishment of urine output led to rapid resolution of the electrolyte abnormalities.
The most likely cause of prolongation of APTT in this case was disseminated intravascular coagulation (DIC). However, in the absence of other coagulation tests (fibrinogen, fibrin degradation products, AT III levels) we were unable to confirm this diagnosis. Demonstration of normal PT does not preclude this diagnosis (Slappendel 1988). Massive tissue destruction, vascular stasis and tissue hypoxia are all well-documented causes of disseminated intravascular coagulation in man and domestic species. In humans, disseminated intravascular coagulation also occurs as a result of various obstetric complications, such as placental rupture, foetal death and amniotic fluid embolisation (Penner 1998). Disseminated intravascular coagulation has recently been reported as a complication of uterine torsion and septic peritonitis in the bitch (Ritt & Fossum 1997). In humans, prolongation of APTT also occurs following pregnancy, as the result of production of anticoagulant autoantibodies directed against coagulation factors VIII and IX. This direct inhibition of the intrinsic coagulation cascade results in a prolonged APTT, with normal thrombin time and near-normal PT (Jandl 1996). Although providing an alternative explanation for prolonged APTT in this case, direct inhibition was thought unlikely as antibodies tend to persist for prolonged periods, whereas in this case APTT normalised within 10 days of surgery. To the authors’ knowledge there is only one other report of abnormal haemostasis associated with dystocia in the cat. In this case prolonged PT, APTT, low platelet count and elevated FDPs, indicating DIC, were found in a cat that underwent successful en bloc ovario-hysterectomy for the treatment of dystocia (Robbins & Mullen 1994).
Anaemia has been reported previously as a complication of uterine torsion in the cat (Pankhurst & Newman 1961, Young & Hiscock 1963, Freeman 1988). Pankhurst and Newman (1961) suggested that primary occlusion of the uterine veins following torsion resulted in engorgement and subsequent rupture of the zonal blood vessels. Although normocytic, normochromic anaemia, with a corresponding reticulocytosis, is known to occur in the last trimester of gestation in the cat (Berman 1974), the profound anaemia observed in this case was consistent with sequestration of blood and haemorrhage into the uterus. Inadequate haemostasis may have contributed to uterine haemorrhage in this case.
The prognosis for uterine torsion in the cat is favourable based on the outcome of the cases reported, where 12/15 cats survived following ovariohysterectomy (Freeman 1988). However, the severity of metabolic and haematological derangements documented in this case, and the inability to resolve them pre-operatively, highlights the need for prompt surgical intervention. Ovariohysterectomy should be carried out, as in this case, without correction of the torsion, as release of endotoxins and inflammatory mediators into the systemic circulation may lead to further compromise of vital organs. In those cases where the torsion was corrected intraoperatively, an unsuccessful outcome was reported (Pankhurst & Newman 1961, Young & Hiscock 1963).