
Abstract
Four cats are reported in which cytology smears obtained by ultrasound-guided fine needle aspiration of the liver were interpreted as indicative of hepatic lipidosis. However, histopathology of hepatic tissue samples obtained with Tru-Cut®-like needles or wedge biopsy revealed that the cats had inflammatory or neoplastic hepatic disease causing their clinical signs. Fine needle aspiration and cytology may not detect infiltrative lesions, particularly those that are nodular, multifocal, or localised around the portal regions. Fine needle aspirate cytology is a useful diagnostic procedure with many advantages, but care must be taken to avoid diagnosing hepatic lipidosis as the cause of illness when an infiltrative lesion is responsible.
Definitive diagnosis of the cause of feline hepatic disease typically requires microscopic examination of hepatic tissue. There are different methods of obtaining a specimen of liver (eg, fine needle aspiration, core needle biopsy, laparoscopic biopsy, wedge biopsy) (Meyer 1996), each having advantages and disadvantages. Fine needle aspiration is the simplest, safest, least expensive, and quickest of these methods (Alleman 1997, Kristensen et al 1990). Anaesthesia is not required for tractable patients, and cytology results can be available within minutes of obtaining the sample. However, hepatic fine needle aspiration typically obtains the smallest tissue sample of these biopsy methods. In contrast, hepatic biopsy utilising a Tru-Cut® type needle, laparoscopy, and abdominal surgery are more expensive, take more time, entail more risk to the patient, and require anaesthesia or heavy sedation. Nonetheless, these latter techniques allow the clinician to obtain larger samples of hepatic tissue, which has the advantage of providing a specimen that is more likely to be representative of what is occurring throughout the liver.
The following four case reports demonstrate situations in which fine needle aspiration of the liver produced cytology smears that were interpreted as consistent with hepatic lipidosis (HL), but which had significantly different diagnoses when tissue samples of hepatic tissue were examined histologically. The purpose of this report is to alert practitioners that there may be clinically significant discrepancies between cytologic and histopathologic results when evaluating feline hepatic disease, and particularly that a cytologic diagnosis of HL can be misleading.
Materials and methods
The records of four cats presented to the Texas A&M University College of Veterinary Medicine and admitted by one of the authors (MDW) were reviewed, and pertinent case information recorded. Each cat had been presented for suspected hepatic disease. The diagnostic evaluation of each cat included history, physical examination, serum biochemistry profile, abdominal ultrasonography, ultrasound-guided hepatic fine needle aspirate, and hepatic biopsy. Fine needle aspirates of the liver were obtained using a 25 gauge needle. The needle was inserted into the liver using ultrasonographic guidance, and the operator then repeatedly applied several ml negative pressure at one or more sites in the liver. The slides were air dried and stained with a modified Romanovsky-like stain (Diff-Quick, Dade Behring Ag, Dudingen, Switzerland). The cytology slides were examined by a clinical pathologist, and a written report was generated. For purposes of this study, the original cytology slides were retrieved and reviewed (MJ) in a blinded fashion, if they were available (Cases 1 and 3); otherwise, the original written cytology report was used to describe the findings. When the cytology slides from Cases 1 and 3 were reviewed without knowledge of the prior diagnosis, the interpretation was essentially the same as originally reported.
Samples of liver tissue for histopathology were obtained either by ultrasound-guided core needle biopsy or by a wedge biopsy performed during laparotomy. Core needle biopsies were obtained by using 14 to 18 gauge needles (Biopty, C.R. Bard Inc.) which were guided ultrasonographically. At least two tissue samples were obtained from each cat's liver. The samples of hepatic tissue were fixed in 10% neutral buffered formalin, routinely processed, and stained with haematoxylin and eosin. The findings from the original histopathology report were recorded, and the original histopathology slides were retrieved and reviewed (BW) without knowledge of the prior cytologic or histopathologic findings.
Case reports
Case 1
An 11-year-old, neutered male domestic long haired cat was presented to Texas A&M because of lethargy, weight loss, and a picky appetite. The cat had previously been diagnosed with pulmonary histoplasmosis and was treated with itraconazole (Sporanox; Janssen). During treatment its condition improved with the body weight increasing from 6.4 to 8.6 lbs over a 5-month period. Two weeks prior to admission to Texas A&M, the cat began losing weight despite still being treated with itraconazole. The cat was eating, but with a diminished appetite. At presentation to Texas A&M, it weighed 7.0 lbs and was obviously thin.
A serum biochemistry panel obtained after admission revealed an increased ALT (891 U/l, reference range=26–84), increased SAP (632 U/l, reference range=20–109), increased GGT (21 U/l, reference range <12), and hypoalbuminaemia (2.4 gm/dl, reference range=2.5–3.3). Abdominal ultrasonography revealed slightly increased hepatic size with a mildly decreased echogenicity. Fine needle aspirates and two core biopsies of the liver were obtained.
Examined smears made from the hepatic fine needle aspirates (Fig 1) were highly cellular, containing many individual and small clusters of hepatocytes in a background of peripheral blood and protein. The hepatocytes had abundant light grey to blue cytoplasm that frequently contained a few to many small discrete vacuoles typical for those seen for lipid accumulation. These vacuoles were occasionally larger in size and arranged in small clusters. A few blue-black granules were present in some hepatocytes. The hepatocytes were uniform in size and had round to oval nuclei with a small nucleolus. Rare cells displayed mild anisocytosis and anisokaryosis. A few non-degenerate neutrophils, small lymphocytes, and eosinophils were present, compatible with peripheral blood contamination. An infectious aetiologic agent was not observed. The cytologic diagnosis was vacuolar hepatopathy.

Photomicrograph of a cytology smear from Case 1. This smear contains many hepatocytes which have small, discrete vacuoles consistent with lipid accumulation. The cytologic diagnosis was mild vacuolar hepatopathy Original magnification= × 1200, bar=10 μm, Diff-Quick stain.
Histologically, hepatocytes exhibited diffuse mild to moderate cytoplasmic swelling, with multifocal mild to moderate vacuolation by lipid, and occasionally glycogen (Fig 2). Most portal tracts were surrounded by a dense accumulation of mixed inflammatory cells, predominately well-differentiated lymphocytes, with lesser numbers of plasma cells, macrophages, and occasional small numbers of neutrophils. The morphologic diagnosis was a moderate, multifocal lymphoplasmacytic chronic pericholangitis.
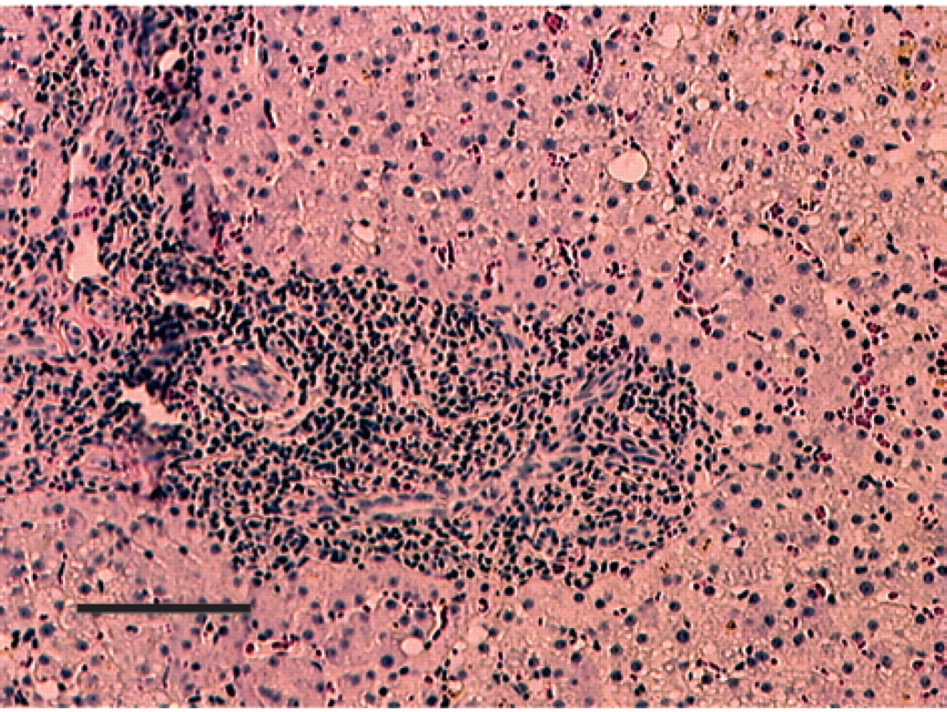
Photomicrograph of a hepatic biopsy from Case 1. The hepatocytes exhibit multifocal, mild to moderate vacuolation by lipid. The portal tract is surrounded by a dense accumulation of mixed inflammatory cells which is predominately composed of well-differentiated lymphocytes. Original magnification = × 400, bar=100 μm, haematoxylin and eosin stain.
Case 2
An 11-year-old, spayed female domestic short-haired cat was presented to Texas A&M because of icterus. Three months prior to presentation at Texas A&M, the cat was icteric and lethargic, and was diagnosed as having hepatic disease by the referring veterinarian. Between being seen at the referring veterinarian and coming to Texas A&M, it lost 2 lbs. The cat's appetite was near-normal. Upon physical examination, the cat was icteric.
A serum biochemistry panel obtained after admission revealed an increased ALT (365 U/l), increased SAP (301 U/l), increased GGT (19 U/l), and increased bilirubin concentration (3.3 mg/dl). Abdominal ultrasound examination revealed marked hepatomegaly with normal to slightly decreased echogenicity and no obvious masses. Ultrasound-guided fine needle hepatic aspirates were performed. Later, abdominal surgery was performed to obtain three wedge biopsies of the liver.
The first attempt at aspirating the liver resulted in several cytology slides which had a similar microscopic appearance, consisting of rafts of hepatocytes having abundant cytoplasm that was acidophilic to mildly basophilic and containing moderate amounts of fat vacuoles and blue granular pigment. Clumps of green staining pigment were also present in foci. Non-degenerate neutrophils were mildly increased in number, but no infectious agents were seen. Some foci had markedly increased vacuolation with mild hepatocyte degeneration. A few small lymphocytes were also present. The cytologic diagnosis was vacuolar hepatopathy. The second fine needle aspirate had similar findings, except that one island of hepatocytes had inflammatory cells interspersed within the extracellular matrix. A third fine needle aspirate of the liver produced slides in which there were mildly increased numbers of lymphocytes.
Histologically, the wedge biopsy of liver exhibited broad, interlacing bands of dense hypercellularity which divided the remaining hepatic parenchyma into large nodules (Fig 3). The regions of hypercellular infiltrate consisted of predominately lymphocytes, macrophages, and plasma cells with occasional neutrophils. In remaining hepatocytes, mild intracytoplasmic accumulations of grainy golden pigment, cytoplasmic swelling, and occasional intracytoplasmic accumulation of lipid and/or glycogen were noted. The morphologic diagnosis was chronic, severe, non-suppurative cholangiohepatitis.

Photomicrograph of a hepatic biopsy from Case 2. There are broad bands of infiltrates that divide the remaining hepatic parenchyma into large nodules. Original magnification = × 100, bar=100 μm, haematoxylin and eosin stain.
Case 3
A 9-year-old, neutered male domestic short haired cat was presented to Texas A&M because of vomiting and weight loss. The cat was presented to Texas A&M initially because of a diminished appetite. At that time it had an increased ALT (202 U/l), increased SAP (427 U/l), and a normal GGT (12 U/l). It was readmitted 6 weeks later, at which time it had lost 5 lbs so that it weighed 13.2 lbs. The cat was still eating a little, but its appetite was worse than before.
A serum biochemistry panel obtained after the second admission revealed an increased ALT (287 U/l), increased SAP (163 U/l), and a normal GGT (9 U/l). Ultrasonography of the liver revealed a ‘fatty appearing liver’, and fine needle aspirates and three core needle biopsies were obtained with ultrasonographic guidance.
Examined cytology slides contained many individual and small aggregates of hepatocytes interspersed in a background of peripheral blood and protein. The hepatocytes had granular, light blue, frequently vacuolated cytoplasm, which was consistent with lipid accumulation. Most of the vacuoles were small and distinctly round with crisp margins. Fewer large vacuoles with indistinct margins were also evident. A few non-degenerate neutrophils and small lymphocytes were present, compatible with blood contamination during aspiration. The cytologic diagnosis was vacuolar hepatopathy.
Histologically, hepatocytes exhibited diffuse mild cytoplasmic swelling, with multifocal mild to moderate vacuolation. Portal regions were surrounded by moderate accumulations of plasma cells and lymphocytes, which occasionally extended into the hepatic parenchyma. Diffuse, mild accumulation of neutrophils and occasional macrophages were noted in most sections. The morphologic diagnosis was moderate, diffuse cholangiohepatitis.
Case 4
A 9-year-old, spayed female mixed breed cat was presented to Texas A&M because of fever, weight loss, and poor appetite. The cat had been losing weight for 4 weeks. Two weeks before admission, the cat was noted to have fever and a poor appetite. At admission, the cat was febrile (103.1 F) and had splenomegaly and icterus. The cat had lost approximately 4 lbs so that it now weighed 7.4 lbs.
A serum biochemistry panel obtained after admission revealed an increased ALT (125 U/l), increased SAP (127 U/l), increased GGT (16 U/l), and hyperbilirubinaemia (2.9 mg/dl). Abdominal ultrasonography revealed a liver that was slightly enlarged with a uniformly echogenic parenchyma. Ultrasound-guided fine needle aspirates were obtained, and two ultrasound-guided core biopsies were performed the following day.
Examined cytology slides contained occasional small clusters of hepatocytes and peripheral blood. The hepatocytes were mildly to moderately vacuolated, and many contained bile. No significant inflammatory cell population was present. There was no evidence of neoplasia. The cytologic diagnosis was hepatocellular vacuolar change plus cholestasis.
Histologically, all tissue samples exhibited multifocal replacement of normal hepatic architecture by accumulations of moderately pleomorphic, round to oval pale-staining cells having single, oval and occasionally slightly indented nuclei. Hepatocytes surrounding the nodules were moderately vacuolated by lipid and glycogen. The morphologic diagnosis was lymphosarcoma.
Discussion
There was discordance between the results of histopathologic examination of hepatic tissue and cytologic examination of fine needle aspirates in these four cats. While the possibility of such discrepancy between cytologic and histopathologic results is well recognised, there is an additional facet to this problem when evaluating the feline liver. In cats, hepatic cytology may not only fail to reveal the correct diagnosis, but may suggest a plausible, albeit incorrect, alternative diagnosis of HL.
Hepatic lipidosis is often anticipated in cats with an appropriate history (ie, anorexia preceding weight loss, followed by jaundice or increased hepatic enzymes) because it is a commonly diagnosed (if not the most commonly diagnosed) feline hepatic disease (Center 1996). Fine needle aspiration of the liver is often performed to diagnose HL because it is recognised as a diffuse parenchymal disease that one expects will be detected by fine needle aspirate cytology (Stockhaus & Teske 1997, Blue et al 1999). Finding vacuolated hepatocytes is often considered confirmatory of HL. However, diagnosing HL as the cause for a cat's clinical illness via fine needle aspiration has the potential to be misleading (Dimski & Taboada 1995). First, one must decide whether the hepatic vacuolation is severe enough to make it likely that HL is causing signs of hepatic failure, or if the lipidosis is likely to be asymptomatic. A cat may lose weight, mobilise fat, and consequently accumulate lipid in its hepatocytes without having HL severe enough to cause clinical signs (Armstrong 1989). Mild to moderate accumulation of lipid in feline hepatocytes is a common finding in cats that do not seem to be suffering from hepatic failure caused by HL (Center et al 1993). Finding vacuolation so marked that almost the entire cytoplasm is replaced and the nucleus is pushed to the side of the cell is consistent with HL severe enough to be causing hepatic failure (Meyer 1996, Blue et al 1999). The fact that the vacuolation seen in the cytologic preparations of these cats (ie, Fig 1) was not that severe was an indication to question whether the HL was severe enough to cause the observed clinical signs.
In addition to evaluating the severity of the vacuolation of the hepatocytes, one must consider whether other concurrent hepatic diseases (eg, inflammatory or neoplastic infiltrates) may be present but undetected, such as were found in these four cats. The discordance between cytology and histopathology results found in these cats is not reason to stop performing hepatic fine needle aspirates. However, one must recognise that unless cytologic examination reveals neoplastic cells (eg, lymphosarcoma, carcinoma) or an aetiologic agent (eg, histoplasmosis) that is always definitive when present, fine needle aspirate cytology results may be misleading. The reason that hepatic aspirate cytology can sometimes incorrectly suggest HL is illustrated in Fig 2 and 3. In both figures, the inflammatory infiltrate is localised around the portal regions, leaving relatively large areas of hepatocytes without any associated infiltrate. Thus, even though these infiltrates were diffuse in the sense that they affected hepatic lobules throughout the entire liver, they were ‘focal’ in that they only affected a portion of each of the hepatic lobules. As others have noted, focal and multifocal hepatic lesions (and these lesions were ‘multifocal’ in that they were present in lobules throughout the liver) have the potential to be missed by fine needle aspiration (Kristensen et al 1990). Further examination of Fig 2 reveals that many hepatocytes in the non-infiltrated areas have cytoplasmic vacuoles, ostensibly due to lipid accumulation. This lipid accumulation is probably secondary to anorexia caused by the primary hepatic infiltrative disease and is what was found by aspirate cytology.
In the first three cases, cytologic examination revealed ‘a few’ neutrophils or lymphocytes in addition to hepatocytes. It is possible that these ‘few’ cells originated from the hepatic infiltrates. However, without being able to assess where these cells came from in the hepatic parenchyma and whether they were closely associated with other such inflammatory cells, their significance could not be determined. These inflammatory cells were present in such small numbers on the cytology slides that they seemed to best represent contamination of the aspirate with peripheral blood. Thus, an obvious benefit of histopathology besides obtaining larger samples of tissue (which should be more representative of what is occurring in the liver) is the ability to ascertain where particular cells originated from and their significance.
Recently, a modification of the traditional negative pressure needle aspiration technique has been proposed (Menard & Papageorges 1998a), and has been suggested to produce better samples for cytologic analysis. These authors further report a series of 501 cats on which this technique was used to aspirate the liver (Menard & Papageorges 1998b). Hepatic lipidosis and hepatitis were both common diagnoses; however, the authors do not mention comparing the cytologic results with histopathology findings. Therefore, while this new aspiration technique may represent an improvement over prior aspiration techniques, it is not clear whether or not it will prevent such discordance as noted in this report.
How frequently cytology obtained from fine needle aspiration of the liver and histopathology fail to agree cannot be determined from our records. These four cases were discovered and reported because they were all supervised by one of the authors (MDW). It is not possible to determine the frequency with which this discrepancy occurs at the authors' institution because of the way in which fine needle aspirate cytology slides of livers from cats with hepatic disease are usually handled there. Such slides are typically examined by the clinician immediately after obtaining them, and often they are submitted to the clinical pathologist for further evaluation and generation of a report only if there appears to be evidence of a neoplastic or inflammatory cellular infiltrate. If the only cytologic finding is HL, the slide is often not submitted to the clinical pathologist, and hence a formal cytology report is not generated and the slides are not saved. Therefore, the authors cannot state how commonly this discrepancy between fine needle aspirate cytology of the liver and histopathology occurs. However, we hypothesise that it is not rare.
Recommending that all cats with clinically significant hepatic disease have biopsy and histopathology of the liver may sound controversial. Obviously, if a cat that has a cytologic diagnosis of HL has an inconsistency in the history, physical examination, or clinical pathology data with such a diagnosis, biopsying the liver by another technique is prudent because histopathology is more definitive than cytology (Dimski & Taboada 1995). Along these lines, one can argue that Cases 1, 2, and 4 had features in the history (eg, adequate appetite, splenomegaly, fever) that strongly suggested that HL was not responsible for the cats' clinical signs. However, Case 3 had a history, physical examination, serum biochemistry panel, and hepatic ultrasound examination that were all compatible with HL. Therefore, one must be cautious about accepting a cytologic diagnosis of HL even when other data are consistent with the diagnosis.