
Abstract

Introduction
Transcranial magnetic stimulation (TMS) seems an attractive tool for the study of seizure disorders. It is simple to perform, relatively inexpensive, and generally safe, with the potential to provide noninvasive clinical measurements of neuronal excitability. Applications in patients with epilepsy include investigation of underlying cortical excitability and determination of the effects of antiepileptic drugs (AEDs); preoperative localization of epileptic foci; and functional mapping. Several review articles have been published on the use of TMS for epilepsy (1–5). Most intriguingly, TMS could become a new seizure treatment modality.
The parameters measured by TMS include motor threshold, which is the minimal threshold for motor response in target muscle and motor evoked potential (MEP) amplitude, both measured using single pulses (see Table 1). The cortical silent period (CSP) is a lapse in electromyogram (EMG), when a TMS pulse is given during tonic voluntary muscle contraction; its duration is related to stimulus intensity. Additional parameters are measured with paired-pulse stimulation techniques. For example, intracortical inhibition (ICI), a decrease in MEP amplitude from the first to the second stimulus, is seen when a subthreshold conditioning pulse is followed by a suprathreshold pulse after a 2- to 5-millisecond delay, whereas intracortical facilitation (ICF) occurs when the pulses are 7 to 20 milliseconds apart.
TMS Parameters
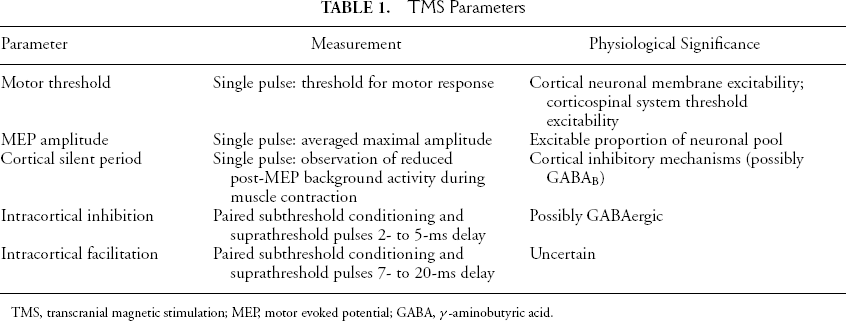
TMS, transcranial magnetic stimulation; MEP, motor evoked potential; GABA, γ-aminobutyric acid.
There is uncertainty concerning the physiologic mechanisms underlying these phenomena. Motor threshold probably reflects cortical and spinal neuronal membrane excitability as well as intracortical synaptic and corticospinal connections (6). MEP reflects the overall pool of potentially excitable neurons; CSP possibly indicates activation of γ-aminobutyric acid (GABAergic) inhibitory interneurons; and ICI and ICF have ill-defined “inhibitory” and “excitatory” mechanisms (4).
The currents generated by TMS and their physiological effects are modulated by a wide variety of factors, including coil construction and positioning, brain conductivity, and neuronal orientation. The brain is not an ideal, uniform, conduction medium. Distribution of field strength and flux as well as effects on cortical excitability may be difficult to predict. Positron emission tomography (PET) blood-flow studies, for example, showed multifocal, bilateral activation from unilateral motor cortex stimulation (7).
Cortical Excitability
Generalized Epilepsies
TMS results suggest that patients with generalized epilepsy syndromes have increased cortical excitability. Patients with primary generalized epilepsy (PGE) show reduced motor threshold and ICI (8,9). Increased facilitation at interstimulus intervals of 200 to 300 milliseconds, but not at 100 to 150 milliseconds, corresponds to the mean interdischarge interval of spike–wave activity on electroencephalogram (EEG) (10,11). MEP suppression to paired stimulation was absent, and ICI was reduced in juvenile myoclonic epilepsy (11,12). Not all studies found hyperexcitability (13,14). A prolonged CSP in PGE may suggest increased intracortical inhibition (14). In an unusual group of patients with PGE and versive, or circling seizures, the interhemispheric difference of the motor-cortical threshold was significantly higher compared with that of PGE patients without circling and with that of normal controls, suggesting an explanation for the clinical phenomena (15).
Patients with progressive myoclonic epilepsy (PME) have reduced motor threshold as well as an exaggerated facilitatory effect of peripheral stimulation on MEP, suggesting an exaggerated influence of afferent input on motor cortical excitability (16). Digital stimulation markedly facilitated conditioned motor evoked potentials, suggesting cortical and subcortical components of abnormal sensorimotor integration in addition to hyperexcitability of the sensory and motor cortex (17).
Interestingly, drug-free patients tested within 48 hours of a first generalized tonic–clonic seizure (GTCS) had significantly increased motor thresholds with normal amplitudes of MEPs, suggesting decreased cortical excitability (18). Cortical silent periods were not significantly different from those of normal subjects. The subsequent period of MEP facilitation found in normal subjects (ISIs of 6–20 msec) was markedly reduced in patients. This suggests the existence of abnormally prolonged intracortical inhibition or deficient intracortical excitation, possibly representing a postictal “protective effect.”
Focal Epilepsy
Alterations in motor threshold and CSP ipsilateral to the focus are more likely to occur in patients with lesions in the motor cortex than those with mesial temporal foci (19–25). Patients with focal cortical dysplasia, very frequent partial seizures, or secondarily generalized discharges may be more likely to show decreased inhibition (26,27). Studies of ICI and ICF have led to inconsistent findings that may be due to subject heterogeneity and AED fluctuations. Patients with benign childhood epilepsy and centrotemporal spikes had normal excitability (19). Perhaps paradoxically, CSP values have been reported to be longer in patients with poor seizure control compared with those with well-controlled seizures (28). Additional studies will be needed to see whether differences in patterns of cortical excitability can have diagnostic implications for patients with partial epilepsy syndromes of uncertain origin. So far, TMS data do not appear to be able to identify focal epileptogenicity in regions outside primary motor cortex.
TMS and Antiepileptic Drugs
TMS has been used in an attempt to elucidate the mechanisms of action of several AEDs (29–31). Motor threshold is increased by phenytoin (PHT), carbamazepine (CBZ), lamotrigine (LTG), and losigamone (LSG)—all drugs that stabilize active sodium channels. Valproic acid (VPZ) also increased motor threshold (19). However, benzodiazepines (BZDs), vigabatrin (VGB), baclofen, and ethanol, which enhance GABAergic transmission, had no effect on motor threshold. Levetiracetam (LEV) reduced MEP amplitude at high but not low stimulus intensity, suggesting an effect on less excitable neurons (31). The CSP was increased by CBZ, gabapentin (GBP), loreclazole (LCZ), and ethanol, but decreased by diazepam (DZP). ICI was enhanced by GBP, LCZ, baclofen, and ethanol, and ICF was suppressed by the same drugs (29). PHT, CBZ, LTG, and LSG had no effect on these parameters.
The effects may be dose and time dependent. Increasing doses of LTG up to 200 mg/day progressively increased motor threshold over 5 weeks (32). There have been relatively few studies of the relation of AED levels and dosing schedules. Prolonged but not single-dose VPA increased motor threshold (2,18). GBP (800 mg) strengthened ICI and suppressed ICF at 3 hours but not at 5 hours after dosing (33).
Thus a rough division exists between “GABAergic” drugs, which affect CSP and possibly ICI and ICF, and “sodium channel” agents, affecting motor threshold. However, the distinction is inconsistent, as CBZ, but not PHT or LTG, increased CSP (4). TMS might be a means of screening patients before starting therapy to choose the most effective agent, but it is unclear whether the choices made would be superior to those based on clinical grounds or whether differences in effects on TMS parameters have any therapeutic implications. Moreover, it is important to remember that AEDs may have several mechanisms of action, potentially influencing cortical excitability, but not all relate to their antiseizure effects.
Seizure Focus Activation
Although seizures in patients with epilepsy occasionally have been evoked with single pulses, multiple stimuli are more effective (34). Seizures may be more likely in patients with craniotomy defects and subdural electrodes or when patients are being withdrawn from AEDs for presurgical monitoring. However, generally, it has proved difficult to “activate” seizure foci, and repetitive transcranial magnetic stimulation (rTMS) is less effective than other methods, such as hyperventilation (35–37). Alterations in spike patterns or focal slowing may occur, but seizures are rarely induced, and the localizing value of rTMS seems limited (34,35,38–41). Some coil configurations, such as the figure of eight, may be superior, and it is possible that more rapid stimulation rates may be more likely to induce seizures (42,43). However, there is a risk that activation may not be specific to the focus (44).
Sleep deprivation, which can provoke seizures in many patients, did not alter motor threshold or the CSP on TMS. However, paired-pulse stimulation showed a significant reduction in intracortical inhibition and facilitation in sleep-deprived subjects. This finding suggests changes in the inhibition–facilitation balance in primary motor cortex, which might be related to the “activating” effects of sleep deprivation (45).
Preoperative Functional Mapping
In planning surgery for epilepsy, it is important to be able to map cortical regions crucial for normal function. Traditional methods include electrocortical stimulation (ECS), either intraoperatively or via permanent subdural electrodes, and the Wada or intracarotid sodium amytal test. More recently, functional magnetic resonance imaging (fMRI) has been used (46). One potential disadvantage of fMRI is that it may identify all regions participating in a task, rather than just those essential for it. TMS shares the “inhibitory” approach of ECS and the Wada test. Some studies have shown general agreement between fMRI and TMS for motor mapping (47). Other investigators suggest that fMRI identifies all cortical areas activated by the motor task, but TMS, only those regions with corticospinal projections (48).
Several studies have investigated the effect of epilepsy surgery on motor excitability. After hemispherectomy, no correlation was found between the degree of hemiparesis and inducibility of the MEP; the pattern of reorganization of ipsilateral motor control was extremely diverse (49,50). Preoperative TMS studies in a 12-year-old with unilateral cortical dysgenesis showed hyperexcitability in the affected motor cortex, including abnormally prolonged muscle responses to TMS, and a wide cortical motor map (51). These features were markedly reduced after multiple subpial transection. Intracortical inhibition in the affected motor cortex was also disrupted preoperatively and improved after surgery. The patient showed fair postoperative motor recovery and good seizure control. Eventually, these data might be useful for preoperative motor cortex mapping and surgical planning.
Attempts at higher cortical function mapping with TMS have been less successful. Single-pulse stimulation generally has little observable language effect. Negative rTMS experiments have been attributed to coil type and position as well as stimulus rate and intensity. One problem in interpreting the results of experiments that show interruption of responses is determining whether true language processing or simply motor-speech output is being affected (52–56). Different language modalities may be affected in different ways. Patients with uncontrolled seizures and left temporal foci had significantly more errors for picture naming, but not word reading, during left frontal, posterior, and superior temporal stimulation in the group as a whole (57). However, the results were too variable on an individual basis to be reliable for use in clinical decisions.
Several studies have compared rTMS with the Wada test. Jennum et al. stimulated each side of the temporal and frontal cortex at a frequency of 30 Hz for 1 second and increased the intensity until speech was inhibited. Patients had a 95% agreement between rTMS and Wada lateralization of speech. At 16 to 25 Hz, stimulation of seven of 14 patients with left lateralization on the Wada test had left-side language effects, and seven had bilateral language effects (53). Twelve of 17 patients with left Wada lateralization had purely left lateralization on rTMS, whereas five had bilateral effects (58). Lateralization of speech arrest induced by rTMS in six patients correlated with IAT results (52).
Memory is more difficult to study than language. Effects on verbal working memory have been found on stimulation in a variety of cortical regions, including bilateral frontal and temporal sites (59–61). It is difficult to use these data for clinical purposes.
The evidence suggests that rTMS probably is useful for motor cortex functional mapping. For individuals being considered for surgery, rTMS seems to reveal significant bilateral language function in patients with uncontrolled partial seizures. It is not clear whether this is an artifact of the technique or a true physiologic phenomenon that needs additional investigation. However, rTMS cannot be used clinically for language or memory lateralization at the present time.
Risks and Side Effects of TMS
Wasserman (62) reviewed the safety of TMS and found that the procedure usually is well tolerated. Minor local discomfort, skin irritation, and dysesthesiae may occur. Seizures after single stimuli have been reported in patients who had no history of epilepsy but had large structural lesions or infarcts. Rare seizures have occurred during rTMS in normal volunteers. The effect of rTMS is a combination of stimulus frequency, intensity, and train duration. A National Institutes of Health (NIH) Consensus Conference outlined safe stimulation parameters (62).
In patients with epilepsy, seizures may occur by chance during TMS studies. The risk of inducing unwanted seizures during rTMS functional mapping is low, especially when AEDs are kept at therapeutic levels (38,63). It actually has been hard to elicit seizures for preoperative mapping, as discussed earlier. A transient surge of prolactin and luteinizing hormone was found in only one patient in whom a complex partial seizure was induced, but no increases in adrenocorticotropic hormone (ACTH) have been found after rTMS (64,65). No histologic changes attributable to rTMS were found in two patients who had temporal lobectomy (66). However, clinical experience is limited and the long-term side effects of rTMS are unknown (62).
Therapeutic TMS
Despite the recent introduction of several new AEDs, a substantial proportion of patients continue to have uncontrolled seizures. Not all are surgical candidates. Brain stimulation has been proposed as an alternative therapeutic approach. Stimulation targets include the cerebellum, caudate, thalamus, vagus nerve, and epileptic focus itself. The concept of stimulating the brain to treat seizures is not new. The electric torpedo fish was said to have been used by Dioscorides in 76 AD, and Leyden jars were tried in the eighteenth century to treat seizures (67).
Homosynaptic long-term depression (LTD) and long-term potentiation (LTP) are persistent changes in synaptic strength that can be induced by electrical stimulation. Generally, low-frequency stimulation is inhibitory and high frequency, facilitatory. LTD can be induced by low-frequency stimulation in hippocampus (68). Ictal discharges in entorhinal cortex were prevented by stimulation at 1 Hz in hippocampal–entorhinal cortex slices in adult mice (69). Akamatsu et al. (70) reported that 0.5-Hz rTMS stimuli increased the latency to pentylenetetrazole-induced seizures in rats. Interestingly, the opposite effect was shown with 50-Hz rTMS, which reduced the latency to pentylenetetrazole-induced clonic seizures (71). The effects may depend on the order of stimulation, as low-frequency stimuli by themselves led to synaptic facilitation in rat amygdala but to inhibition when preceded by a conditioning high-frequency stimulus (72). Fifteen minutes of 1-Hz stimulation applied after 60-Hz kindling stimulation suppressed afterdischarge duration and seizure stage throughout the course of kindling in immature rats, suggesting a strong antiepileptogenic effect (73). A similar phenomenon has been observed in resected human temporal cortex (74). Several clinical studies suggest that rTMS may have analogous depressant effects on neuronal function. Low-frequency rTMS reduces motor cortex excitability (75). On PET, 1-Hz left prefrontal cortex rTMS decreased cerebral blood flow in right prefrontal cortex, left medial temporal cortex, left basal ganglia, and left amygdala (7).
A small number of patients treated with rTMS for seizures or myoclonus have been reported. A patient with partial seizures and focal cortical dysplasia was treated with 100 stimulations at 0.5 Hz, 5% below motor threshold, twice a week for 4 weeks (76). There was a 70% decrease in seizure frequency compared with the months before stimulation. Interictal spikes were reduced 77% after the first 100 stimulations. Three patients with myoclonus showed transient improvement, and a small cumulative effect was noted over several days (77). However, additional studies did not confirm a therapeutic effect in myoclonus (58). In an open study, eight of nine patients had a reduction in seizure frequency or severity after rTMS on 5 consecutive days, using a round coil with two pulse trains of 500 stimulations each, given at 0.33 Hz (78). Seizures were counted for 4 weeks before and after the week of stimulation, while patients were taking constant AEDS. Mean seizure reduction was 38.6% ± 36.6%.
Nonblinded, uncontrolled therapeutic trials in epilepsy can be difficult to interpret and are particularly vulnerable to placebo effects. Theodore et al. (79) studied 24 patients with localization-related epilepsy, randomized to blinded active or sham stimulation. Weekly seizure frequency was compared for 8 weeks before and after 1 week of 1-Hz rTMS for 15 minutes twice daily at 120% of motor threshold. When the 8-week baseline and poststimulation periods were compared, active patients had a mean seizure frequency reduction of 0.045 ± 0.13, and sham-stimulated controls had a reduction of −0.004 ± 0.20. Over 2 weeks, actively treated patients had a mean reduction in weekly seizure frequency of 0.16 ± 0.18, and sham-stimulated controls, of 0.01 ± 0.24. There was a tendency for patients with neocortical, as opposed to mesial temporal foci, to have a greater mean reduction in seizure frequency. However, none of the effects was significant.
The Theodore et al. study (79) used a figure-of-eight copper coil, which generated a 1.5- to 2-Tesla magnetic field at the surface of the scalp, with a spatial resolution of approximately 0.5 cm. With a similar coil, field strength 4 cm below the surface of the scalp is 1.5 V/cm, probably the minimum needed to evoke motor effects (80). The center of the hippocampus is approximately 5.5 cm below the surface, however. The peak field in studies producing finger movements appeared to occur at 0.3 to 0.6 cm below cortical surface, in the gray–white junction/layer VI (81). The Theodore et al. (79) controlled trial results are consistent with the anatomy of stimulation, suggesting that stimulation may be suboptimal in the mesial temporal region and that rTMS, if it works at all, may likely be more effective for patients with neocortical than with mesial temporal foci. Moreover, the difference between the 2- and 8-week reduction in seizure frequency suggests that the therapeutic effect of TMS, if any, is likely to be short-lived.
Several new rTMS therapeutic studies are in progress. Theodore et al. are conducting a study similar to the initial one but involving a larger group of patients with neocortical foci. The study uses the same blinded, placebo-stimulation design as well as coil and stimulus rate. However, the duration of stimulation is increased to 30 minutes twice a day. Tergau et al. (82) are performing a study on patients with drug-resistant epilepsy syndromes, using a round coil placed over the vertex. Each patient receives three different types of stimulation on 5 consecutive days, with 1,000 pulses daily, in randomized order: 0.3-Hz, 1.0-Hz, and 0.6-Hz sham stimulation using a coil with “ineffective” output. These two studies use different approaches to assessing the efficacy of rTMS, and the results will be interesting to compare.
Conclusions
The clinical role of TMS in epilepsy remains uncertain. Some valuable results have been reported from studies of cortical excitability in generalized and focal epilepsy. TMS can provide interesting but limited data on the effects of AEDs. However, it has not been useful for preoperative localization of epileptic foci, nor is it a reliable tool for functional mapping. The most exciting potential use for TMS is in the treatment of seizures. So far, however, controlled trials have not confirmed the results of anecdotal studies.