
Abstract
Case report
A 46-year-old woman with a past medical history of episodic migraine and benign sexual headache was in good health until she experienced an explosive, sudden and severe occipital headache while having a bowel movement. There was no associated loss of consciousness or awareness. The headache, however, was associated with nausea and neck pain/stiffness. The headache intensity diminished over several hours. Two days later, she experienced a recurrent more prolonged thunderclap headache, whereupon she was taken immediately to hospital. In the emergency department (ED), she was hypertensive (190–200/110–120) and mildly drowsy. Examination revealed no meningeal, long tract, focal, or lateralizing neurological signs. Furthermore, there was no evidence of hypertensive retinopathy or papilloedema.
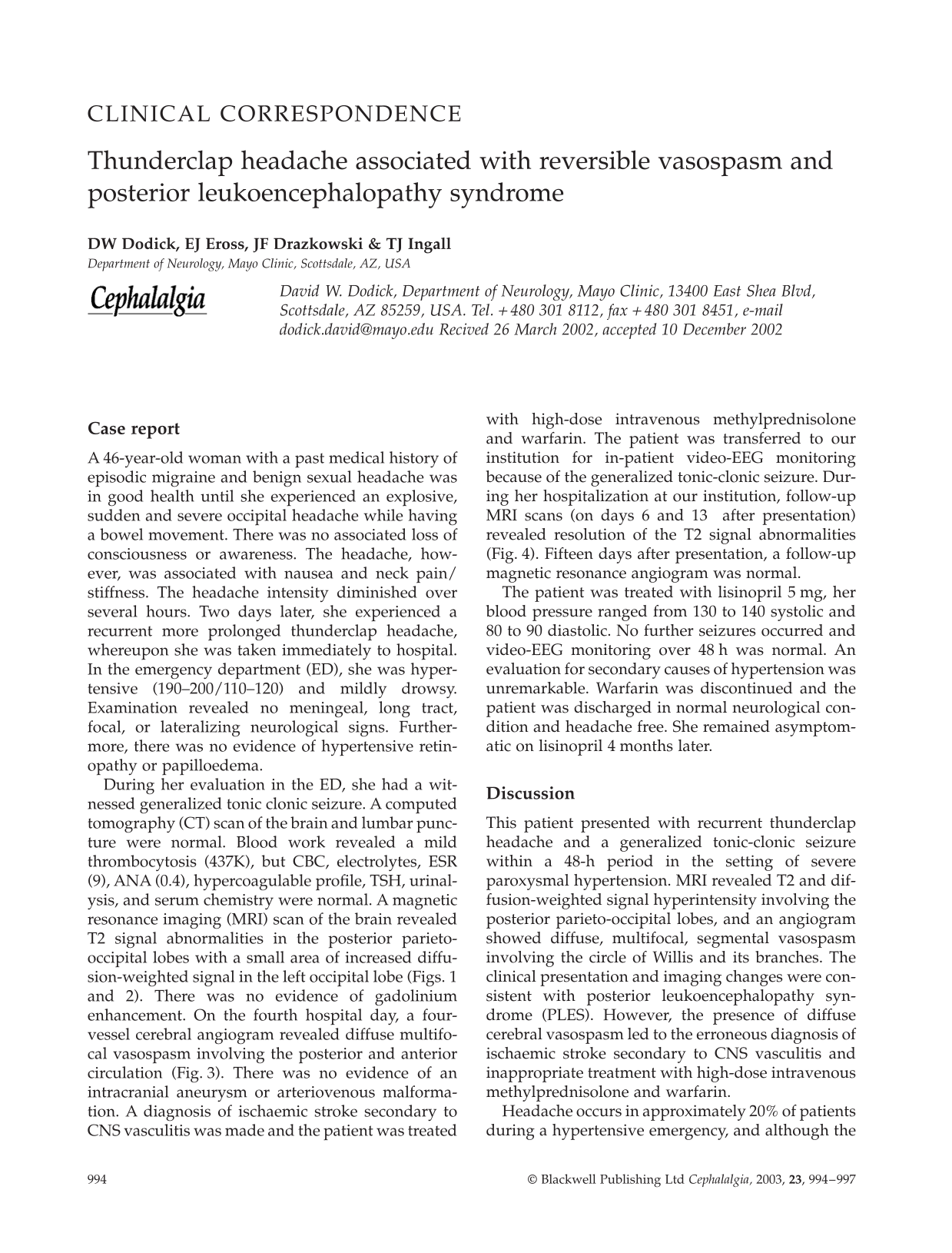
During her evaluation in the ED, she had a witnessed generalized tonic clonic seizure. A computed tomography (CT) scan of the brain and lumbar puncture were normal. Blood work revealed a mild thrombocytosis (437K), but CBC, electrolytes, ESR (9), ANA (0.4), hypercoagulable profile, TSH, urinalysis, and serum chemistry were normal. A magnetic resonance imaging (MRI) scan of the brain revealed T2 signal abnormalities in the posterior parieto-occipital lobes with a small area of increased diffusion-weighted signal in the left occipital lobe (Figs. 1 and 2). There was no evidence of gadolinium enhancement. On the fourth hospital day, a four-vessel cerebral angiogram revealed diffuse multifocal vasospasm involving the posterior and anterior circulation (Fig. 3). There was no evidence of an intracranial aneurysm or arteriovenous malformation. A diagnosis of ischaemic stroke secondary to CNS vasculitis was made and the patient was treated with high-dose intravenous methylprednisolone and warfarin. The patient was transferred to our institution for in-patient video-EEG monitoring because of the generalized tonic-clonic seizure. During her hospitalization at our institution, follow-up MRI scans (on days 6 and 13 after presentation) revealed resolution of the T2 signal abnormalities (Fig. 4). Fifteen days after presentation, a follow-up magnetic resonance angiogram was normal.
(a, b) The initial FLAIR MRI sequences reveals signal abnormalities located in the posterior parieto-occipital lobes.

The initial diffusion-weighted image show an abnormality existing in the left occipital lobe.

The cerebral angiogram (hospital day 4) reveals diffuse, multifocal, segmental vasospasm in the posterior circulation. Similar findings were present in the anterior circulation.

Follow-up FLAIR MRI (14 days after initial MRI) is essentially normal.
The patient was treated with lisinopril 5 mg, her blood pressure ranged from 130 to 140 systolic and 80 to 90 diastolic. No further seizures occurred and video-EEG monitoring over 48 h was normal. An evaluation for secondary causes of hypertension was unremarkable. Warfarin was discontinued and the patient was discharged in normal neurological condition and headache free. She remained asymptomatic on lisinopril 4 months later.
Discussion
This patient presented with recurrent thunderclap headache and a generalized tonic-clonic seizure within a 48-h period in the setting of severe paroxysmal hypertension. MRI revealed T2 and diffusion-weighted signal hyperintensity involving the posterior parieto-occipital lobes, and an angiogram showed diffuse, multifocal, segmental vasospasm involving the circle of Willis and its branches. The clinical presentation and imaging changes were consistent with posterior leukoencephalopathy syndrome (PLES). However, the presence of diffuse cerebral vasospasm led to the erroneous diagnosis of ischaemic stroke secondary to CNS vasculitis and inappropriate treatment with high-dose intravenous methylprednisolone and warfarin.
Headache occurs in approximately 20% of patients during a hypertensive emergency, and although the headache is usually throbbing and non-distinct (1), thunderclap headache has been reported in a recent report of a patient with hypertensive encephalopathy with PLES (2). The clinical presentation and MRI changes in the patient described here are very similar to those described in this recent report and are suggestive of PLES secondary to severe hypertension.
PLES is a rapidly evolving neurological condition characterized by headache, nausea and vomiting, visual disturbances, altered mental status, decreased alertness, seizures, and, occasionally, focal neurological signs (3, 4). PLES is associated with an abrupt and severe increase in blood pressure in most cases, including patients with eclampsia or renal disease with hypertension. Although hypertensive encephalopathy is the most common cause of PLES, there have been a number of cases described which occurred in the absence of severe hypertension. The syndrome is also seen in patients treated with immunosuppressive drugs such as intravenous immunoglobulin, cyclosporin A, tacrolimus, and interferon-alpha (3). The main finding in neuroimaging and autopsy studies is posterior white matter oedema, particularly involving the parietal and occipital lobes, which may spread to the basal ganglia, brainstem, and cerebellum (5, 6). Complete clinical and radiological recovery often occurs with prompt anti-hypertensive treatment or withdrawal of the immunosuppressive drug. Occasionally, the clinical features and CT or standard MRI findings may be indistinguishable from a bilateral posterior cerebral artery stroke syndrome. Thus, early recognition of PLES is essential.
To the best of our knowledge, diffuse cerebral vasospasm, as seen in this case, has not been previously reported in patients with PLES. The mechanism of the reversible vasospasm in this patient is unclear. Reversible vasospasm of the cerebral vasculature is recognized to occur in patients with idiopathic thunderclap headache, following subarachnoid haemorrhage (SAH) due to a ruptured saccular aneurysm, and in association with pheochromocytoma, eclampsia sympathomimetic (amphetamine and cocaine) and ergotamine drug intoxication, angiographic contrast material, surgical manipulation, and closed head injury (7–15). It has also been described in patients with ‘vascular’ headache, migraine, and ‘isolated benign cerebral vasculitis’(16–18). The mechanism of vasospasm in this patient and in patients with PLES is unclear, but may be related to a loss of autoregulation, resulting in dilatation of cerebral arterioles and disruption of the blood–brain barrier (BBB). In animals, arteriolar resistance increases proportionately as blood pressure rises until a threshold is reached at which autoregulation fails segmentally, and the mechanical effect of elevated pressure causes passive segmental vasodilation (19–21).
The recognition that reversible segmental vasospasm can occur in patients with PLES has important clinical implications. As seen in this case, an acute neurological illness which is associated with cerebral vasospasm and acute parenchymal changes on MRI can easily be mistakenly diagnosed as CNS vasculitis and result in the inappropriate use of immunosuppressive and anticoagulant therapy. Indeed, recognizing the clinical and MRI features of this disorder would obviate the need for a cerebral angiogram. Failure to recognize this syndrome could also lead to failure to lower blood pressure acutely and aggressively, the definitive treatment of PLES, especially when the diagnosis of ischaemic stroke is erroneously made. It should also be recognized that isolated CNS vasculitis is not known to present with thunderclap headache in the absence of SAH, and these patients often have abnormal spinal fluid examinations (22). Furthermore, isolated CNS vasculitis is invariably restricted to blood vessels which are < 0.5 mm in diameter and not, as in this case, large blood vessels that constitute the circle of Willis and its second-order branches.