
Abstract

Introduction
Hot bath-related headache (HBRH), a new disorder recently described by Negoro et al., is provoked by pouring hot water over the patient or by soaking in a hot bath (1). In this study, we present four cases of HBRH. In most respects our patients have similar characteristics to the previously reported cases of this type of headache, but also present some differences, such as beginning at an earlier age, always occurring after taking a hot bath, and not disappearing spontaneously.
Case reports
Case 1
A 29-year-old woman had from the age of 15 years always developed a headache after taking a hot bath. The headaches occurred within 5–10 min of getting out of the hot bath. They occurred by gradual onset, reached their maximum intensity in 10–15 min, were bifrontal, severe or moderate, and not throbbing headaches, and lasted for 1–1.5 h without photophobia, phonophobia, nausea, vomiting, etc. They could be relieved by taking an analgesic tablet and/or bed rest. After 3 years from the beginning of the headaches, the patient became aware that the headaches would not occur if she dried her hair with a hair dryer immediately after getting out of the bath. Thereafter she dried her hair after taking every hot bath. She reported that, if she did not dry her hair after a hot bath, she had the same headaches. Other types of exposure to heat, such as heat exposure during hairdressing which lasts 15–20 min with approximately the same degree of heat, and long periods of sun bathing on the beach in summer, did not bringing on the HBRH. The patient did not ingest any particular foodstuffs or beverages, and did not use any particular perfumes during the hot baths. In addition, the patient developed migraine headaches with aura for 4 years. The headaches localized to the left side of the head, and were throbbing and lasted 3–6 h with photophobia, nausea, and vomiting.
Case 2
An 18-year-old girl had suffered for 10 years from migraine headaches without aura, which were severe and throbbing and affected the whole head, with nausea and vomiting. The patient's migraine headaches became frequent in the last year and than she was given prophylactic flunarizine for 6 months. During this period her migraine headaches became significantly less frequent. She had developed further headaches after taking every hot bath in the last 3–4 years apart from the disorders outlined above. These headaches gradually developed and reached a maximum level of intensity in 10–15 min, were severe or moderate and not throbbing headaches localized to the occipital region without nausea and vomiting, and lasted for 1–1.5 h. They began immediately after leaving the bathroom. They could be relieved usually by resting in the bed for an hour. There was no history of triggering of headaches by heat stimulus other than hot bath. The patient did not ingest any particular foodstuffs or beverages, and did not use any particular perfumes during the hot baths. She needed an analgesic drug when the pain was severe. In this patient use of flunarizine for prophylaxy of migraine was not effective against the HBRH.
Case 3
A 34-year-old man was admitted to our unit with tension headache and depression which had existed for 4–5 months. On his medical history, he reported that he had been having headaches and feeling that his hair was bristling when exposed to very cold weather from the age of 15 years. He described severe or moderate and not throbbing headaches on the whole head without nausea and vomiting, lasting 30–60 min. He took an analgesic to lessen the pain. He developed further headaches, similar to the headaches described above, and always felt his hair to bristle after taking a hot bath for the last 4 years. The headaches began within 4–5 min after leaving the bathroom, with gradual onset, lasted 45–60 min, did not occur with exposure to different types of heat, and diminished with bed rest and/or an analgesic drug, 500 mg paracetamol. There was no history of ingesting any particular foodstuffs or beverages, or using any particular perfumes during hot baths.
Case 4
A 38-year-old woman had from the age of 23 years always developed headaches after taking a hot bath. The headaches had occurred within 10 min of getting out of the hot bath. They were of gradual onset, reached their maximum intensity in 10–15 min, were bifrontotemporal, severe or moderate, and not throbbing headaches, and lasted for 3–6 h with no accompanying photophobia, phonophobia, nausea and vomiting. She reported that the headaches would not occur if she took an analgesic tablet (500 mg paracetamol or metamizol) immediately after leaving the bathroom. She then started to take an analgesic tablet after every hot bath. If a headache occurred when no analgesic was taken immediately after the hot bath, an analgesic tablet could still relieve it. Drying her hair after a hot bath did not prevent the headache. There was no headache history with exposure to other types of heat, or association of these headaches with ingesting any particular foodstuff or beverages, or use of any particular perfumes during the hot baths. In addition, the patient had suffered migraine headaches with aura for 10 years. The headaches localized to the left or right side of the head, and were severe and throbbing, and lasted 3–8 h with photophobia, nausea and vomiting.
None of the patients had a history of any other disease, and neurological examination, routine blood and urine examinations, EEG and cranial computed tomography and magnetic resonance imaging findings of all the patients were normal (Table 1).
Some characteristics of the patients
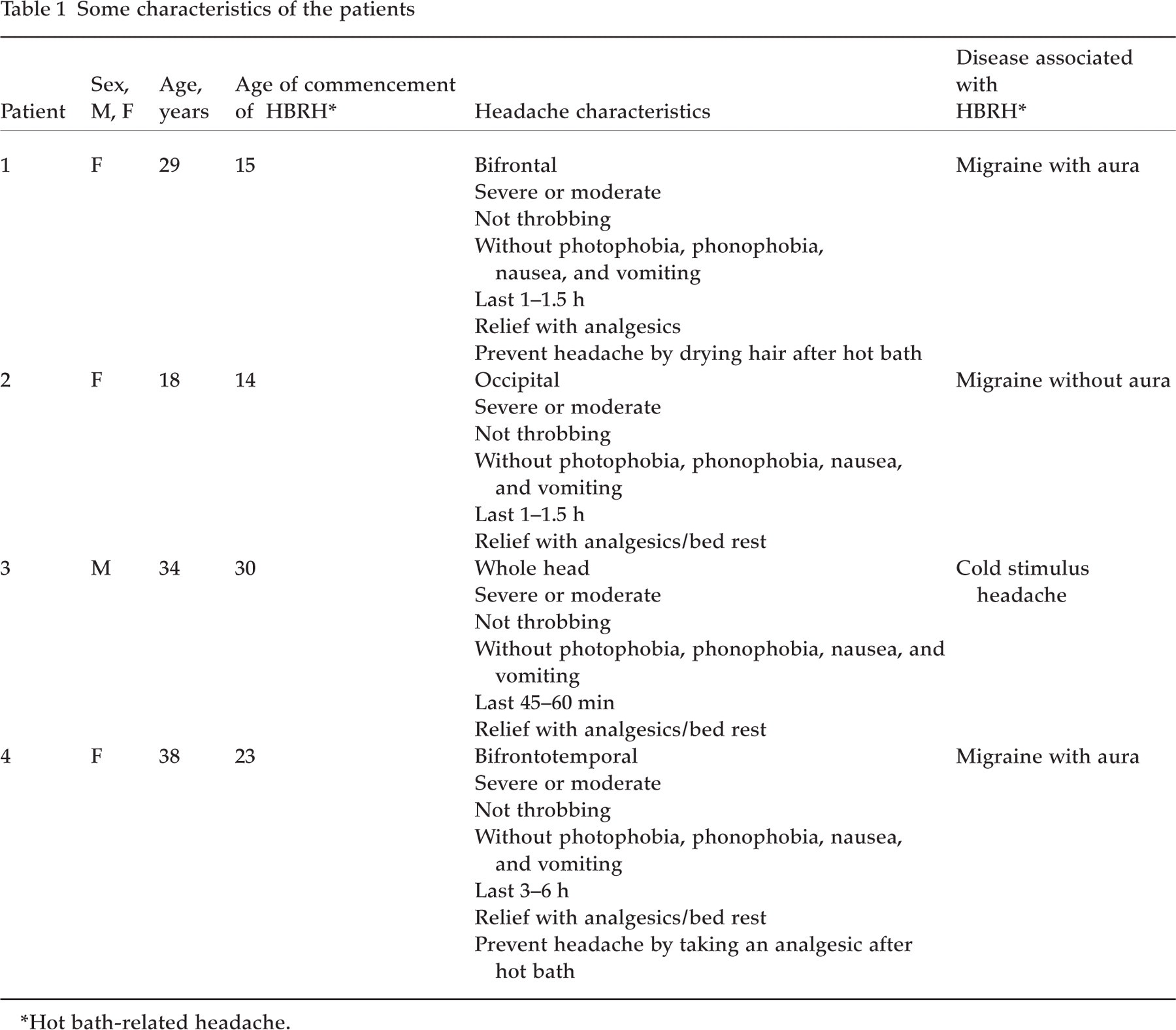
∗Hot bath-related headache.
Discussion
Our patients consisted of three females and one male, whereas in the report of Negoro et al. (1) all the patients were female. The female preponderance is seen in HBRH. The age for the beginning of the headaches was 15, 14, 30, and 23 years for our patients. However, the beginning ages of headaches for Negoro et al.'s patients were 48, 42, and 41 years (1). The beginning ages of our patients’ headaches were clearly earlier than those of the others.
The headaches in our patients began within 10 min after leaving the bathroom, i.e. after taking a hot bath. However, the patients in the other study reported developing headaches immediately after pouring the hot water over themselves or soaking in the hot bath. The headaches in our patients began somewhat later than the other reported cases. Although the headaches in our cases were still continued except for cases 1 and 4, Negoro et al. reported the headaches in their cases lasted for a certain period (a few weeks or months), and had disappeared spontaneously (1). Our first patient had been aware that the headaches did not occur if she dried her hair with a hair dryer immediately after taking a hot bath, and had prevented her headaches in this way since then. The mechanism by which the hair dryer prevented the headaches in this patient is not clear. One of the possible mechanisms could be the placebo effect. Our fourth patient had prevented her headaches by taking an analgesic drug immediately after every hot bath. The only explanation for an oral analgesic drug taken immediately after a hot bath preventing a headache which will begin in 10 min is a placebo effect.
The general characteristics of the headaches in our cases were severe or moderate, not throbbing pains, of gradual onset and reaching their maximum intensity in 10–15 min, confined to frontal, frontotemporal or occipital regions bilaterally, or on the whole head, not associated with aura, nausea, or vomiting, beginning within 10 min after taking a hot bath, lasting for 30 min to 6 h, relieved by taking an analgesic drug, and not occurring with exposure to other types of heat. The headache properties are, in general, similar to the headaches in the cases reported by Negoro et al. (1).
A hot water bath (approx. 37–40 °C) usually takes approximately 15–20 min in our country. Odourless soap or shampoo is generally used during the hot bath in Turkey.
Our first, second and fourth patients also suffered from migraine headaches. The characteristics of migraine headaches in these patients showed clear differences from those of the HBRHs. Although use of flunarizine for migraine prophylaxy in case 2 decreased the frequency, duration, and intensity of migraine headaches, it showed no effect on the HBRHs.
None of our patients referred to our clinic due to HBRH. The reasons for referring to our clinic were: cases 1, 2, and 4 for migraine, and case 3 for tension headache and depression. People in our country do not refer primarily to a physician because of HBRH and cold stimulus headache (CSH), as these phenomena are considered a personal characteristic rather than a disease. We can define HBRH with detailed medical history when the cases refer to us for other reasons such as migraine. We think, for this reason, that HBRH is not rare in the community.
The pathogenesis of HBRH is not known. In the light of available knowledge, the possible mechanisms are as follows: (i) it is possible that hot stimulus (hot water used for a hot bath) may trigger headaches in these patients by bringing on vasodilatation at the cerebral arteries; (ii) two of the patients reported by Negoro et al. and also our third patient were associated with CSH. CSH is thought to be caused presumably by excessive stimulation of temperature-sensitive receptors in the face and scalp (2, 3). Negoro et al. speculated that, ‘this conjunction of CSHs and HBRHs suggests that HBRH might be connected with excessive stimulation of temperature-sensitive receptors in the face and scalp’ (1) with exposure to heat. If this is true, HBRH which is provoked by taking a hot bath could be named ‘hot stimulus headache’, as the CSHs provoked by the exposure to the cold (external application of a cold stimulus and/or ingestion of a cold stimulus) were classified as CSH (2); (iii) the hot water poured over the head may affect the head and scalp as a cold stimulus by cooling them while evaporating. Thus, the headache occurring due to hot water, HBRH, may be a kind of CSH. Hot air is usually used for drying hair quickly using a hair dryer. Drying of the hair by a hair dryer might prevent headaches by preventing the process mentioned above in case 1; (iv) there was a conjunction of migraine and CSH in most cases when those of Negoro et al. and ours are considered. The reason for this conjunction is not clear. It was previously reported that CSH was more frequent in migraineurs then in the general population (4, 5). The underlying pathogenic mechanism in the cases of HBRH may predispose these patients to the other disorders (migraine and CSH), i.e. there may be identical or similar points in the pathogenesis of these three disorders.
The international classification of headaches has not yet include HBRH (2). From the point of view outlined above and also from our present knowledge, it may be proper to include this kind of headache in Group 4 (miscellaneous headaches unassociated with structural lesion).
HBRH will in time be better known with reporting of new cases, and elucidation of possible underlying pathogenic mechanisms.