
Abstract
The aims of this study were: (i) to compare health-related quality of life (HRQoL) as measured by the Medical Outcomes Study Short Form 36-Item Health Survey (SF-36) in a population sample of migraine headache sufferers and controls without migraine; (ii) to assess the relationship of HRQoL and work-related disability attributed to headache in a population sample. The study was conducted in two phases. First, a population-based, telephone interview survey of 5769 residents of greater London, England was conducted to identify individuals with migraine headache (cases) and controls without migraine. In the second stage, in-person interviews were conducted in a matched sample of 200 migraine cases and 200 controls selected from survey respondents. At the beginning of the in-person interview, participants were asked to complete the SF-36. In addition, a work-related disability score based on the telephone interview was defined as the number of lost work days or days when usual activity was reduced by 50% or more over the previous year. The disability score was trichotomized as mild (n = 98), moderate (n = 49), and severe disability (n = 49). Compared with controls, individuals with migraine headache scored significantly lower in eight of the nine domains of the SF-36 as well as in the overall Physical Component Summary (PCS) score and Mental Component Summary (MCS) score. Further, among migraine sufferers, each of the disability groups scored significantly lower in seven of the nine domains and in the summary scales. Scores showed greater reductions in HRQoL for the moderate and severe disability groups vs. the mild disability group in five of nine scales and in the Total Physical Summary score. We conclude that, in a population-based sample of migraine headache sufferers, individuals with migraine headache have lower HRQoL scores compared with controls. Moreover, among individuals with migraine headache, work-related disability is associated with lower HRQoL scores. Specifically, individuals classified with moderate to severe work-related disability had lower HRQoL scores than those classified with low disability.
Introduction
Migraine headaches vary in severity from moderate pain with no activity limitations to severe pain and prolonged incapacitation (1, 2). Depending on the frequency of attacks and level of disability, migraine headaches may also influence health status and behaviour between attacks (1, 2). The burden of migraine has been assessed using many kinds of measures. Common strategies include assessment of health-related quality of life (HRQoL) and measurement of headache-related disability (2).
Quality of life refers to an individual's assessment of their general well-being and position in life as perceived within the context of their culture, value systems, goals, and concerns (2). HRQoL is a subset of overall quality of life that encompasses an individual's health state, functional status (both physically and mentally), as well as the individual's overall well-being (3).
Measures of HRQoL provide a quantitative assessment of an individual's health status including the aggregate burden imposed by specific health conditions such as migraine headache. HRQoL has been assessed in headache sufferers using two categories of questionnaires: generic and disease specific (4). Generic HRQoL instruments are designed to measure the influence of a broad range of health conditions using a single yardstick. They are useful for making comparisons across individuals and disease categories. The most widely used generic HRQoL instrument is the Short Form 36 (SF-36). This brief questionnaire, developed as part of the Medical Outcome Studies, has been extensively used in patients with chronic diseases, including headaches (3–6). Other generic HRQoL scales include the SF-20 (7), the SF-12 (8) and the Sickness Impact Profile (9). Disease-specific HRQoL instruments are designed to provide more precise measurement of the burden imposed by specific conditions. They should have greater sensitivity to the specific burdens imposed by a condition and better discriminate a change over time than generic measurements (10). However, disease-specific HRQoL measures cannot be used to compare HRQoL across disease categories (2).
HRQoL in migraine sufferers has been assessed in a number of studies conducted in subspecialty clinics (4, 6–10). However, patients who seek care from specialists represent < 5% of migraine sufferers (11, 12). In addition, these patients tend to have more severe disease, more frequent attacks, and more co-morbid illnesses (13). As a consequence, studies in specialty care centres may not accurately estimate the impact of migraine in the general population (1, 4, 14, 15). Two studies have assessed HRQoL in a population-based sample of migraine sufferers and a contemporaneous population-based control; one study from the USA (16) and another from the Netherlands (17) showed that those with migraine have significantly lower HRQoL as measured by the SF-12 (16), and SF-36 (17).
In addition to HRQoL, an alternative way of measuring the burden of migraine focuses on activity limitations or temporary disability. For example, a Canadian population survey of migraine found that half of migraine sufferers discontinued normal activities during their attacks and almost one-third required bed rest (18). In more than 70% of the headache sufferers in this survey, interpersonal relationships were impaired (18). Other studies have measured disability by estimating lost time due to migraine, including both inability to do things as well as reduced effectiveness (19–22). Extending this approach, the Migraine Disability Assessment (MIDAS) questionnaire measures lost time due to migraine in three domains: work, household work and chores, as well as family, social and leisure activities (23–26). Measures of lost time are more readily translated into economic terms because absenteeism and reduced productivity at work are the principal determinants of the cost of illness (27). In general, improvements in health status translate into increases in HRQoL and reductions of disability. Disability scores and HRQoL run in the opposite direction (1, 3, 6).
In this study, we measure the HRQoL in a population-based sample of individuals with and without migraine headache as measured by the SF-36. In addition, we evaluate work-related disability and examine the relationship of work-related disability and HRQoL.
Methods
This study was completed in two phases. In the first phase, a population-based survey was conducted using a validated computer-assisted telephone interview (CATI). The survey was used, in part, to identify cases with migraine headache, according to the criteria proposed by the International Headache Society (IHS) (28), and controls without migraine. In the second phase, in-person assessments were completed in a sample of migraine cases and matched controls selected from survey respondents. During the in-person assessments, participants completed the SF-36 questionnaire and answered questions about headache-related disability.
Population sample and survey
The population-based survey was conducted in the boroughs of Croydon, Kingston, Sutton, and Merton, within greater London, England. In brief, a sample of households was selected using random digit dialling methods. Ten attempts were made to contact each household. At the time of initial telephone contact, a census of the household was obtained from the person who answered the phone. To obtain a census, the gender and age of each eligible household member were ascertained.
An age-eligible individual (18–55 years) was selected at random for interview. Verbal informed consent was obtained and the purpose of the survey was described to the respondent. Subjects were told that the interview would require 5–15 min to complete. Respondents who agreed to participate were interviewed about their headaches using a clinically validated CATI. A total of 5769 interviews were completed in the UK boroughs. The participation rate was 70.9%.
The CATI interview has been described in detail elsewhere (23, 29). Participants were first asked if they had at least one headache not due to a head injury, hangover, pregnancy, or an illness such as a cold or flu. Detailed questions were asked about the most severe headache type that the respondent had in the last 12 months. The most severe headache type was initially self-defined. If respondents had a second and different self-defined headache, the same questions were also asked about this headache. Questions covered all the diagnostic features of migraine with and without aura, as specified by the IHS (28). Each headache feature reported in the affirmative (ever vs. never) was followed by a question about how often the feature occurred with the specific headache type. The response options included: never, rarely, less than half the time, and half the time or more. When nausea, photophobia, or phonophobia were reported in the affirmative, a follow-up question was also asked about the severity (mild, moderate, or severe) of the symptom.
The diagnostic validity of the CATI was assessed by comparing the telephone-based diagnosis for migraine with an independent diagnosis assigned by a trained physician (23). In the UK, the sensitivity of the telephone interview diagnosis was 91%, specificity was 97% (23), and the positive predictive value was 94%, results similar to that obtained in a US validation study (29).
Definition and selection of migraine cases and controls
Eligible migraine cases met IHS criteria for migraine headache (with or without aura) (28), and had at least six migraine headaches in the past year. This criterion of including subjects with at least six migraine attacks in the last year was intended to ensure that subjects had recent migraine in hopes of optimizing recall. In addition, we wanted subjects whose migraine was an issue in their lives; we reasoned that if attacks occurred less than every other month on average, migraine might not have chronic effects. Those with 15 or more headaches (of any type) per month were excluded.
Eligible controls did not meet criteria for migraine (IHS 1.1 or 1.2) or migrainous headaches (IHS 1.7) (28), and reported fewer that 15 headaches per month. Individuals reporting any migraine-defining associated symptom (i.e. nausea, vomiting, photophobia, or phonophobia) more than rarely with their headaches, or reporting two or more migraine-defining quality of pain features (i.e. exacerbation, unilateral head pain, moderate to severe intensity, or throbbing pain) more than rarely with their headaches were also excluded. Other headaches were not excluded. Controls were matched to individual cases on gender, year of birth (within 3 years), date of interview (within 2 weeks), and race. In four cases, race could not be matched. An effort was made to enrol one control for each case. Where more than one matched control was available, we selected one control at random.
From the 5769 survey respondents, a total of 767 eligible migraine cases were identified. Of the 767 eligible migraine cases, subjects were randomly selected to be interviewed in person. In order to yield 200 migraine cases for in-person interview, 235 persons with migraine were approached. To yield 200 control subjects, 242 individuals were approached. Subjects received £25 for their time and travel costs.
In-person assessment
The in-person assessments were conducted by trained medical interviewers in a research clinic. Before initiating the interview, signed informed consent was obtained. The interviews gathered information on the following: demographics, work and educational history, leisure and recreational activities, headache symptom history and history of co-morbid conditions (e.g. depression and anxiety), medical history, and perceived impact of headaches on family life. Study participants also completed self-administered versions of the SF-36 (30), the RAND Symptom Checklist-90 (31) and the Eysenck-10 questionnaire (32).
The SF-36 measures HRQoL in nine subscales including a one-item measure of change in health status (labelled health transition) and eight domain-specific measures: physical functioning, role–physical, bodily pain, general health, vitality, social functioning, role–emotional, and mental health. The physical functioning subscale measures the impact of health on limitations to any physical activity including dressing, bathing, running or lifting heavy objects. The role–physical subscale assesses the impact of health on work and related activities. The bodily pain subscale evaluates the severity of bodily pain in the past month and its impact on work or chores. The general health subscale summarizes current health status overall. The vitality subscale captures general energy levels by assessing feelings of ‘pep and energy’ and of being ‘worn out and tired’. The social functioning subscale reflects the impact of health on participation in social activities. The role–emotional subscale assesses the impact of emotional health on work and other activities. and finally, the mental health subscale evaluates the frequency of feelings of nervousness, depression, happiness, and calm.
The SF-36 was scored in accordance with the published standards (31), where 100 represents the best possible score (e.g. excellent health, no limitations at all) and 0 represents the worst possible score (e.g. feeling tired and worn out all of the time, very severe limitations). The eight domains of measurement are summarized into two scales that measure the physical component of HRQoL, the Physical Component Summary, and the mental component of HRQoL, the Mental Component Summary (30, 31).
Work-related disability was defined by responses to two questions asked during the in-person interview. These questions were: ‘Thinking about the time when your headaches most interfered with your job or career, on average, how many days per month or per year did you miss?’, and ‘Thinking about the time when your headaches most interfered with your work or career, when you were still able to go to work, on average, how many days per month or per year was your productivity reduced by half or more?’. Responses were recorded as the total number of days of work missed in the past year and as the total number of days when productivity at work was reduced by half or more in the past year, respectively. Responses to these two questions were summed as a measure of total number of affected days. Among migraineurs, disability scores ranged from 0 to 336; each migraine case was classified into one of three categories of disability: low disability (0–15 days), moderate disability (16–38 days), and high disability (39–336 days).
Statistical analysis
Analysis of variance was used to compare controls to all migraine cases and to migraine case subgroups defined by disability scores (low, moderate, high) on domain-specific HRQoL scores. To compare each disability group with each other and with the control group, a multiple comparisons procedure was used only when the overall F-test was significant at 0.01.
Results
Study participants
Individuals with migraine who completed a clinical visit (n = 200) were similar to the 235 migraine cases who were approached to be interviewed in person (data not shown) and to 767 population-based migraine cases identified in the telephone survey (Table 1) with regard to gender (79.5% vs. 78.4% female), age (49.5% vs. 48.4% were ≥ 40 years of age), and race (92.5% vs. 89.9% Caucasian). Moreover, migraine headache cases were representative of all migraine sufferers with regard to headache features (Table 2), including average unmedicated headache duration (41.0% vs. 41.2% 5–24 h), nausea associated with headache (83.5% vs. 83.0%), photophobia associated with headache (81.0% vs. 84.3%), and phonophobia associated with headache (72.0% vs. 67.3%), but differed on headache frequency (40.5% vs. 30.1% reported ≥ 25 per year) and headache pain intensity (42.5% vs. 34.7% reported 9 or 10 on a 10-point pain intensity scale). A total of 59.3% of the migraine case sample (118 of 199) had a self-reported physician diagnosis of migraine on the screening interview. One subject was missing on this item. For the 118 previously diagnosed migraine cases and the 81 previously non-diagnosed migraine cases, there were no significant differences in any of the HRQoL measures.
Distribution of selected demographic characteristics reported in the initial telephone interview among the 200 migraine headache sufferers and the 200 control subjects
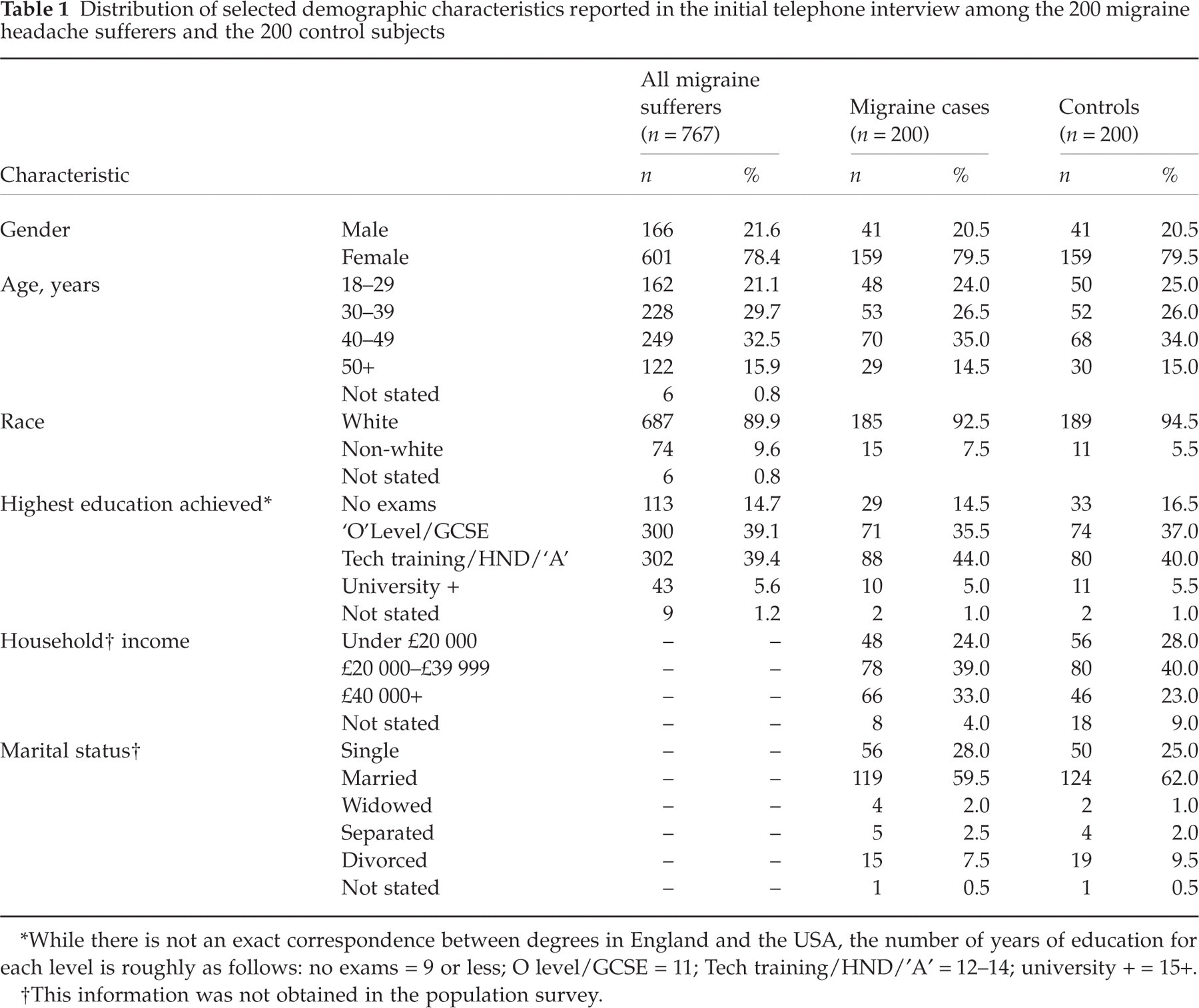
∗While there is not an exact correspondence between degrees in England and the USA, the number of years of education for each level is roughly as follows: no exams = 9 or less; O level/GCSE = 11; Tech training/HND/′A′= 12–14; university += 15+.
†This information was not obtained in the population survey.
Distribution of selected headache characteristics among population-based migraine headache sufferers, participating migraine cases, and control subjects

∗These 27 subjects reported having at least one headache in the last year and at least five in their lifetime, but did not provide a frequency of headaches for the last year.
Group matching ensured that migraine cases and controls participating in the clinical study were similar in distribution by gender, age and race (Table 1). Cases and controls were also similar in education, i.e. comparable with regard to the highest education achieved and marital status, but, on average, migraine cases had a higher annual household income than control (Table 1, 33.0% vs. 23.0%£40 000 or higher). As expected, there were substantial differences between migraine cases and controls with regard to headache characteristics (Table 2).
HRQoL and migraine headache
Migraineurs had reduced quality of life relative to healthy controls, as indicated by significantly lower scores in eight of the nine scales and in the summary measures (Fig. 1). The greatest differences were measured on role–physical (55.4 for the combined case groups vs. 79.2 for controls; P < 0.005), bodily pain (55.4 vs. 79.2; P < 0.005), social functioning (73.6 vs. 88.9; P < 0.005), and role–emotional (70.4 vs. 90.9; P < 0.005) scales. No differences were identified for the health transition scale. In addition, there were statistically significant differences on the two summary scores—the total Physical Component Summary and the total Mental Component Summary. On each of these summary scales the migraine cases had reductions of more than 5 points, compared with the control population.

Comparison of the SF-36 domain-specific quality of life scores among control (▪) and migraine (□) cases. ∗P < 0.05.
HRQoL and headache-related disability
Within the migraine case group we examined HRQoL in each of the disability groups (Table 3). Using a multiple comparisons procedure, all disability groups were individually different from the control group in all SF-36 scales except the health transition subscale. In six of the comparisons, the low disability group was significantly better off (as reflected by the high scores) than the moderate and high disability groups. Though trends were similar for the vitality and mental health scales, the low disability group was different from the high disability group but not from the moderate group. The HRQoL scores were substantially lower (>10 point difference) among individuals in the high disability group compared with the low disability group for role–physical (70.2 vs. 45.3), bodily pain (64.3 vs. 48.2), vitality (53.3 vs. 43.8), and social functioning (80.2 vs. 66.8). In no comparison was the high disability group different from the moderate disability group. There were no differences among the disability groups for the role–emotional and health transition scales.
Mean, median, and standard deviation of the SF-36 domain-specific quality-of-life scores among controls and migraine cases by disability status

∗Using a planned comparison of the control group vs. all case groups, P < 0.005 by analysis of variance.
†Using a multiple comparison's procedure, the control group is significantly different from each case group at P < 0.05.
‡Using a multiple comparison's procedure, the control group is significantly different from the moderate and the high groups at P < 0.05.
§Using a multiple comparison's procedure, the low disability group is significantly different from the moderate and the high groups at P < 0.05.
¶Using a multiple comparison's procedure, the low disability group is significantly different from the high group at P < 0.05.
Due to missing data for the disability score, four subjects were not classified according to level of disability.
Discussion
Measurement of HRQoL and disability have emerged as important complementary approaches to the evaluation of the burden of headache (1, 4, 15, 25). The present study shows that a population sample of migraine sufferers has substantial, statistically significant reductions in most domains of HRQoL as measured by the SF-36 in comparison with a contemporaneous control group drawn from the same population.
Most previous studies of HRQoL among those with migraine identify subjects from referral or specialty care clinics or from among clinical trials participants. For example, Osterhaus et al. (1) reported the HRQoL in a convenience sample of clinical trial participants. In this study, scores in the migraine group were substantially lower in several HRQoL domains when compared with published norms for the US population. However, clinical trials participants are unlikely to be representative of migraine sufferers in the community. In addition, the study did not have a contemporaneous control group. For these reasons, patient selection limits the generalizability of the findings.
A number of other clinic-based studies demonstrate the impact of migraine on the HRQoL. In a subspecialty clinic-based sample, Solomon et al. (5) found that HRQoL was significantly reduced relative to published population norms and relative to patients with other chronic conditions, such as arthritis, diabetes and back problems. This group also demonstrate that HRQoL scores improve with treatment (33). Breslau et al. compared the well-being of migraine sufferers with an age- and sex-matched control group, and found that, even between attacks, migraine sufferers reported more symptoms and greater emotional distress as well as disturbed contentment, vitality, and sleep relative to the control population (34). Clinic-based studies of HRQoL in migraine have been reviewed elsewhere (2, 14, 15).
HRQoL in migraine has on occasion been examined in special populations. The SF-36 was administered to a sample of employees of the French national gas and electricity company (21). The study reported a reduced HRQoL when comparing migraineurs with non-headache control subjects. No differences were observed between migraineurs and other headache sufferers. In this predominantly male, employed population, there may be selection against the most severe headache sufferers.
Few published reports have examined HRQoL in population-based samples of subjects with migraine and in contemporaneous population control. One previous study from the Netherlands (17) showed that subjects with migraine in the community had significantly lower scores on eight SF-36 scales relative to population controls. A study from the USA showed that using the SF-12, HRQoL was reduced in a population sample of migraine sufferers (16). This study demonstrated that migraine and depression exert a significant and independent influence on HRQoL.
The present study shows that migraine in the community exerts a similar HRQoL burden in the UK in comparison with the two previous population studies (16, 17). This study also confirms that many migraine sufferers experience high levels of disability. Half of migraine sufferers experience substantial disability on 16 or more days per year. This is compatible with the prior distribution of lost time reports, which estimate lost time due to migraine (20, 22).
In this study, we explored the relationship between HRQoL and disability. We compared HRQoL in migraine sufferers with low, moderate and high disability. The subgroups with moderate to high disability had lower mean HRQoL scores in all domains; these differences reached statistical significance (P < 0.05) for the following scales: physical functioning, role–physical, bodily pain, general health, social functioning, and the Total Physical Component Summary. There were small non-significant differences in HRQoL between the moderate and high disability groups. Scores were within 5 points of each other for the moderate and high disability group for all domains but the Physical Component Summary score. Our results suggest that both moderate and severe disabling migraine have profound impact on HRQoL, highlighting the burden of this disease. HRQoL measures appear not to discriminate migraine sufferers with moderate to severe disability. Therefore, for assessing the burden of the most severely affected migraine sufferers, disability measures may have advantages over HRQoL measures. Nonetheless, as the degree of disability increases from low to moderate or severe, HRQoL decreases.
This study has several limitations. First, migraine diagnosis was based on a CATI, not a clinical assessment. Although misdiagnosis is possible, the CATI has been demonstrated to have very high sensitivity and specificity, both in the USA and in the UK, using a clinical diagnosis as the gold standard (23, 29). In addition, only migraine sufferers with six or more attacks per year were included. HRQoL would probably be higher if individuals with less frequent headaches had been included, as prior studies show an inverse relationship between HRQoL and disability (16, 17). Our results apply to the migraine sufferers with 6–15 migraine days per month. These results may not apply to those with less frequent attacks, and therefore should not be extrapolated according to the full spectrum of migraine prevalence. A third issue concerns the potential influence of co-morbid depression. Migraine and depression are co-morbid (16, 34, 35) and each influence HRQoL (16). Because depression and other co-morbidities were not measured, we cannot investigate their influence on the present results. This issue does not challenge the accuracy of our measurements but rather the causal attribution. Finally, disability was assessed using two questions focused on the time the patients’ headaches were at their worst, not a validated questionnaire, such as the MIDAS. Therefore, the time of the disability assessment and time of the HRQoL assessment may not coincide, potentially alternating the association between these measures. The disability questions focused on lost time and reduced productivity at work and were measured in units of days. The HRQoL questions were scaled together to generate a score in arbitrary units. The correlation we observed suggests that disability accounts for part of the variation in HRQoL, but that the domains are partially independent.
Our study shows that in a population-based sample of migraine headache sufferers, individuals with migraine headache have reduced HRQoL scores compared with population controls. Moreover, among individuals with migraine headache, work-related disability is associated with lower HRQoL scores. Specifically, individuals classified with moderate to severe work-related disability had lower HRQoL scores than those classified with low disability. This study highlights the profound impact of migraine on the quality of life and suggests an inverse correlation between migraine disability level and quality of life, emphasizing that even subjects in the lowest disability group are burdened by migraine. Additional work is required to assess the clinical utility of HRQoL and disability assessment as well as the benefits of treatment on these metrics (25, 36, 37).
Footnotes
Acknowledgements
The authors thank AstraZeneca Pharmaceuticals for supporting this research.