
Abstract

Introduction
Allodynia is present when non-pain stimuli evoke pain (1). Touch-evoked extracranial allodynia may occur during migraine attacks (2, 3), and suggest a sensitization process (4–6). Allodynia occurs in 79% of migraine attacks and spreads beyond the distribution territory of any nerve, suggesting that migraine produces central sensitization. We describe a patient with a long history of migraine with aura, who developed attacks of extracranial stabbing and burning pain associated with allodynia (ESBA) independent of her migraine attacks. These attacks had the same duration as her migraine attacks and resolved completely after she was treated with a β-blocker. On two occasions, discontinuing the β-blocker led to recurrence of the migraine and ESBA. We review the mechanisms involved in producing allodynia and the possible relationship of this syndrome to migraine.
Case report
A 44-year-old woman had a 22-year history of visual aura (fortification spectra and negative visual phenomena). These symptoms lasted 20 min and were followed by bilateral frontal headache. Once a month the headache was severe and throbbing, and associated with nausea, vomiting, photophobia and phonophobia, and lasted 72 h. The patient had been treated with amitriptyline for 2 years. Headache duration, intensity and frequency were reduced, and fewer analgesics were required per attack. Ten months prior to presentation, she began to experience stabbing pain over her head, limbs, and abdomen. This lasted for fractions of a second, and occurred several times a day. When the stabbing sensation occurred repetitively in the same area for 15 min, a prolonged burning attack followed that lasted 48 h. They were burning in character, ‘like a burn with hot water’, and there was increased cutaneous touch sensitivity during the first 24 h. The patient did not have headache, or other associated symptoms, such as photophobia, phonophobia, nausea, or vomiting. During the last 24 h after the attack, the patient did not have allodynia, and the burning sensation decreased until it disappeared in the last 24 h (Fig. 1). The attacks recurred two or three times per month and were unilateral, although they would occur on different sides of the body (Fig. 2).
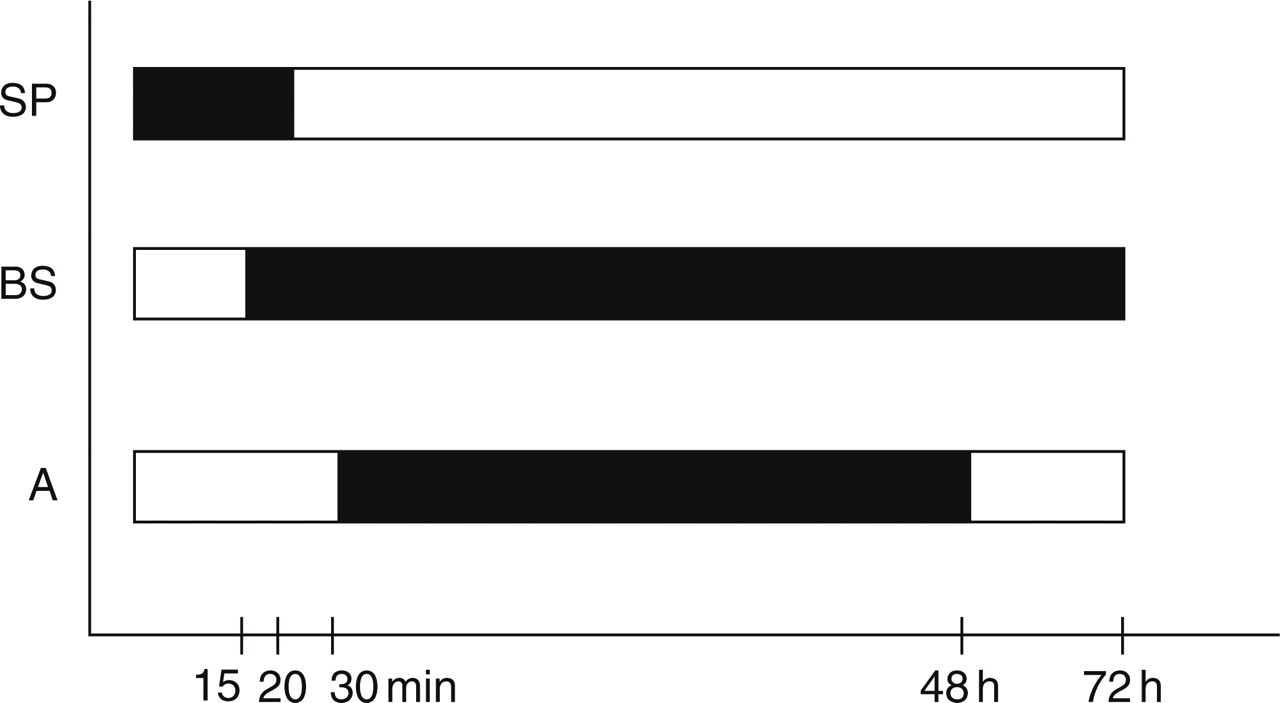
Biological standard of the pain symptoms. SP, Stabbing pain; BS, burning sensation; A, allodynia. ▪, Present; □, absent.

Main sites where the patient felt the sensory symptoms (allodynia).
After the ESBA attacks started the patient also experienced new attacks of migraine without aura. General physical and neurological examinations were unremarkable. Local signs, such as redness or oedema, did not appear during these attacks. EEG, computed tomography and magnetic resonance imaging of the brain and cervical spine were normal. Sixty days after starting propranolol 40 mg/day the migraine attacks and the sensory symptoms disappeared. Ninety days later, the patient discontinued the propranolol. Fifteen days after propranolol withdrawal, the ESBA recurred, about three times a month. Propranolol was reintroduced and the patient was followed for 10 months, during which time she had only three ESBA episodes and one migraine attack.
Discussion
The pain of migraine probably originates from activation of sensory nerves that supply intracranial blood vessels and the meninges and project to the trigeminal nucleus caudalis (7). During migraine attacks, trigeminal activation is accompanied by the release of vasoactive neuropeptides, especially calcitonin gene-related peptide (CGRP) (8). The neuropeptides amplify the trigeminal terminal sensitivity by stimulating the release of bradykinin and other inflammatory mediators from non-neural cells (7, 8). If the initial activation of peripheral nociceptors is not stopped within 30 min, increased excitability of the pain system occurs, which may last for hours and even days (9). The substrate that underlies this sensation is usually an increase in the ongoing firing rate and a decrease in the minimal stimulus intensity required to activate nociceptors (10). The clinical correlation of this sensitization is spontaneous pain and induction of pain by usually non-noxious stimuli (allodynia) (5, 11).
Sensitization of second-order nociceptors in the nucleus caudalis can explain how pain signals that arise from meningeal nociceptors during migraine attacks can induce facial cutaneous allodynia (12). Allodynia that spreads beyond the trigeminal distribution could involve higher order neurones, perhaps at the level of the thalamus. Current understanding of central sensitization suggests that hyperexcitable peripheral nociceptors are spontaneously active, even in the absence of peripheral stimuli, and the impulses they generate induce long-lasting hyperexcitability in second-order neurones (13). Second-order nociceptors also receive direct input from fibres that supply different cutaneous and visceral structures. Sensitization of second-order nociceptors that innervate one organ can change the way they process sensory signals that arise from another organ (11). Sensitization of third-order trigeminovascular neurones that receive convergent input from second-order dorsal horn neurones (from the level of the caudal trigeminal nucleus to at least the C2 segment) (14) may explain how pain signals that arise from meningeal nociceptors during a migraine attack induce cutaneous allodynia outside the referred pain area (11). Positron emission tomography scan studies showed that during heat allodynia, there is a unique activation of the medial thalamus, the contralateral right ventral putamen, the dorsal midbrain, and limbic brain structures of both hemispheres such as the right anterior insula, perigenual cingulate cortex, and the prefrontal and orbitofrontal cortices (6).
Allodynia can occur during migraine (2, 3). Spontaneous pain and allodynia occur only after sensitization of the peripheral or central nociceptive system (11). Our patient had attacks of allodynia without migraine pain or associated symptoms. The association between allodynia and migraine can be justified for several reasons:
Both migraine and allodynia attacks occurred at the same period of the patient's life.
Migraine attacks last 4 and 72 h without treatment (15). In this case the attacks of allodynia lasted about 48 h and the burning sensation lasted 72 h. If extracranial allodynia develops from sensitization of the nociceptive system that has the same biological life span as migraine, they may have similar neuronal mechanisms.
Propranolol reduced the frequency of both the migraine and the allodynia attacks. Both cutaneous mechanical hyperalgesia and sensitized cultured dorsal root ganglion neurones in the absence of nerve injury can be attenuated by propranolol (16, 17). PGE2 may sensitize nociceptors (18), an effect that appears to be mediated by at least two second-messenger systems, both of which can be blocked by propranolol (18). This mechanism of action could explain the clinical relationship between the migraine and allodynia attacks and the efficacy of propranolol for both disorders.
The first symptom of the allodynia attacks was a recurrent pain similar to ‘jabs and jolts’. This was followed by burning sensation and allodynia (Fig. 1). Jabs and jolts are commonly seen in migraine (19). Extratrigeminal jabs and jolts have been noted in migraine (20). This type of pain could be caused by either a peripheral or central disturbance (21).
A number of benign episodic recurrent conditions have been considered to be migraine-related or migraine-like disorders. We believe that ESBA should be included in this category (Table 1) (22–25).

In conclusion, we have described a novel type of recurrent pain attack without a temporal relationship to migraine head pain. The occurrence of the extratrigeminal idiopathic stabbing pain and burning sensation before the allodynia suggests a sensitization process. We speculate that a susceptibly to sensitization is present in both disorders.