
Abstract

Introduction
Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing (SUNCT) is a syndrome predominant in males. In the majority of the cases, aetiology and pathogenesis are unknown. Only a few descriptions of SUNCT-like picture linked with either intra-axial or extra-axial posterior fossa lesions are reported in the literature (1–5). To our knowledge, SUNCT syndrome linked with sinus cavernous lesion has not previously been described.
We report a case of SUNCT syndrome, which increased progressively and revealed a tumour of the ipsilateral cavernous sinus.
Case report
A 45-years-old patient, with nephroangiosclerosis due to severe arterial hypertension, received renal transplantation in July 2000. Immunosuppressive therapy by ciclosporine, azathioprine and steroids was then introduced. He had an history of ischaemic cerebral strokes: the first one occurred in 1995 (right hemiparesia), the second in 1997 (paresia of the right leg) and the third in January 2001 (right abducens palsy). Symptoms disappeared in a few days at each time.
About six months after transplantation, the patient started to complain of severe periorbital headache attacks, of a wrenching character. The attacks were always left-sided. As soon as the headaches started, in March 2001, the patient noted that, during the attacks, the left eye was tearing with conjunctival injection, associated with nasal congestion. Tearing, with conspicuous conjunctival injection and nasal congestion, started, for each attack, immediately after the onset of the pain and persisted throughout the duration of the pain. The duration of each attack was 1–2 minutes and they could be induced by orthostatism. There was no trigger zone. Attacks occurred during the day and night and awakened the patient. The headache attacks became progressively more frequent and more intense: the patient reported they occurred once a week in March 2001 which increased to 10–15 attacks per day by September 2001. Intensity was then described as dreadful. The patient did not report nausea and there was no interictal pain.
In September 2001, a neurological examination showed corneal hypoesthesia. A diplopia appeared in October 2001. Lancaster's test revealed a left abducens palsy.
Several treatments were given (paracetamol, beta-blocker (propranolol: 80 mg/day), tricyclic antidepressant (amitriptyline: 25 mg/day), benzodiazepine (clonazepam: 1.5 mg/day), oxcarbazepine (low daily dose of 300 mg/day because of renal insufficiency), lamotrigine (300 mg/day), indomethacin (125 mg a day)) without any improvement. Morphine (90 mg/day) improved the headaches a little.
Blood tests showed a high sedimentation rate (100/130 mm) with lymphopenia (850/mm3). There was a kidney insufficiency (creatininaemia: 250 µmol/l). Serology of Human Immunodeficiency Virus was negative. Serology of Ebstein-Barr Virus was compatible with old immunization. Spinal fluid was normal (albuminorrhachia, glycorrhachia, cytology). A Magnetic Resonance Imagery (MRI) scan showed a lesion of the left cavernous sinus, enhanced by gadolinium injection (Fig. 1). Flair sequences of the MRI scan also showed small cerebral lacunae in the basal ganglia and a significant leuco-araiosis. Surgical biopsy revealed an Epstein-Barr virus-associated leiomyosarcoma, involving the cavernous sinus, due to immunodeficiency. Immunosuppression was reduced. The patient received chemotherapy (adriamycine) and a protontherapy was realized. Nevertheless, the headache attacks did not improve and the patient died in July 2002 because of local tumour progression and kidney failure.
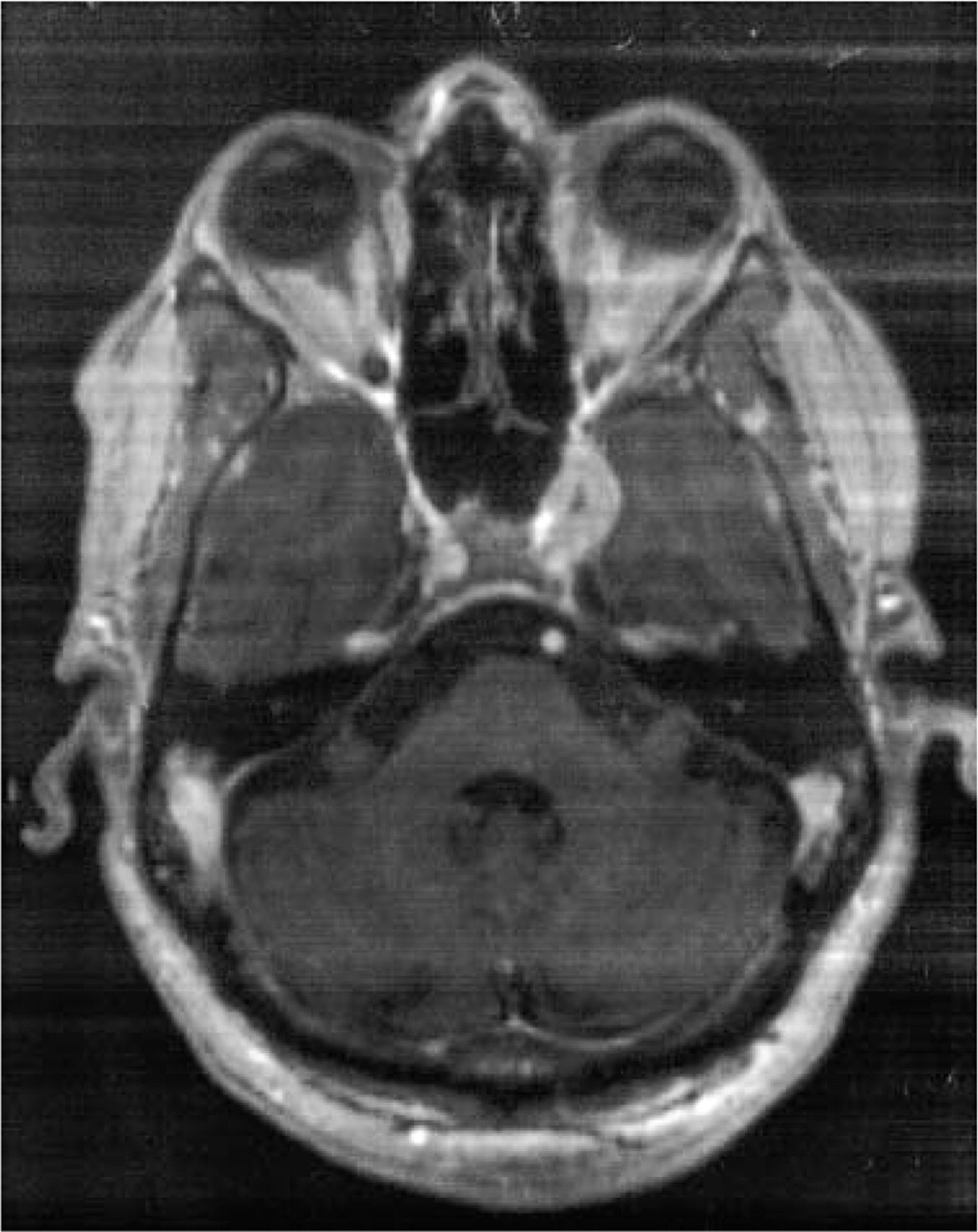
Axial cerebral MRI (T1W sequence with gadolinium injection), showing a lesion in the left cavernous sinus, enhanced by gadolinium injection.
Discussion
Sjaastad et al. reported the full description of SUNCT syndrome in 1989 (6, 7): attacks are strictly unilateral, with pain usually confined to the ocular or peri-ocular area. Intensity is moderate to severe, with pain of a burning, stabbing or electrical nature. Mean duration of the paroxysms is one minute. Ipsilateral conjunctival injection, lachrymation and rhinorrhea are regularly associated with the attacks. Treatment of such a pain is usually very difficult, especially because of the lack of persistent effect of drugs used in other type of headaches. According to diagnosis criteria of SUNCT syndrome reviewed by Goadsby & Lipton in 1997 (8), our patient had a SUNCT syndrome. The clinical picture had however, atypical features of SUNCT such as absence of trigger zone and frequent nocturnal attacks.
Trigeminal neuralgia of first division involvement differs usually from SUNCT syndrome in a few clinical features (9, 10): mean duration of the attacks is shorter; autonomic features appear after years of attacks; attacks are more intense; pain could extend progressively to other territories (V2 and V3); and effects of carbamazepine is usually good. According to this, clinical features of the pain of our patient are clearly different from those of trigeminal neuralgia.
Nevertheless, the localization of the tumour of our patient in the cavernous sinus and the corneal hypoesthesia suggest that pain is linked with a blow of the trigeminal nerve in the cavernous sinus. Few data support the hypothesis of a link between SUNCT syndrome and the trigeminal nerve. A reduction of corneal sensitivity has been already noted in some patients with idiopathic SUNCT syndrome (11). Others have showed abnormalities of orbital phlebography in the cavernous sinus in two patients with idiopathic SUNCT syndrome (12).
Such a link between trigeminal nerve and SUNCT syndrome has also already been suggested by the cases of symptomatic SUNCT syndrome (1–5). Table 1 summarizes the different locations of lesions responsible of SUNCT syndrome in the literature. Two of them were secondary to cerebellopontine angle lesions, close to the trigeminal root and, in a lesser extend, to the facial root (1, 2). In a third one, the SUNCT syndrome was due to a cavernous haemangioma in the anterolateral part of the pons in close proximity to the trigeminal nerve root entry zone (3). The fourth case of symptomatic SUNCT syndrome described in the literature was due to brainstem compression, complicating a basilar impression, without accurate location (4). In the last case (5), the SUNCT syndrome started and resolved in parallel with a Horner's syndrome, suggesting that the autonomic features of SUNCT syndrome were due to a sympathetic deficit, which contribute to a relative autonomic imbalance with functional parasympathetic excess.

M, Male; CPA, Cerebellopontine angle.
Our case is the first one of SUNCT syndrome with a lesion of the cavernous sinus. The tumour was clearly responsible of a lesion of the abducens nerve (diplopia) and of the first division of the trigeminal nerve (corneal hypoesthesia) in the cavernous sinus. The facial nerve was not involved in the lesion. Despite the few descriptions of symptomatic SUNCT syndrome in the literature, this case supports the absolute need for MRI investigation in any suspected case of SUNCT syndrome, searching lesion in the posterior fossa or in the cavernous sinus, especially if some clinical features suggest trigeminal involvement.