
Abstract
In a female population of Turkey (1146 adult females), some epidemiological and clinical characteristics of migraine and tension type headache and their subtypes were investigated. The relation of the headache severity to clinical characteristics were inquired.
Migraine prevalence was found to be statistically higher in the 35-44 years age group (P < 0.01) and those who were university graduates (P < 0.001), married (P < 0.01) and living in urban areas (P < 0.01). Tension type headache was found to be higher in the 45-64 years age group (P < 0.05). Chronic tension type headache patients were found to be older than episodic type (P < 0.01) and frequently were in the lowest education level (P < 0.05).
Presence of impact on daily activities because of the severity of headache was found to be related to aggravation by physical activities (P = 0.001) in tension type headache, with no clinical characteristics in migraine headache and on consideration of all headache patients with throbbing nature (P < 0.05), aggravation on physical activities (P = 0.001), nausea (P < 0.01), vomiting (P < 0.05) and phonophobia (P < 0.05).
Introduction
There are many epidemiological studies of headache, but relatively few studies are conducted in Asian countries. It is reported that racial, cultural and environmental risk factors play an important role in epidemiological findings (1). This study was performed in an Asian country, whose population belongs to the Caucasian race. Studies especially concerning females are also relatively few. In an epidemiological study of headache in Turkey printed as an abstract performed on 2007 person, one year prevalence of migraine and tension type headache (TTH) were reported as 16.4% and 31.7%, respectively (2). But the clinical characteristics of headache were not evaluated. This is the first population based and detailed study of headache and its clinical characteristics based on IHS criteria in a female population of Turkey. The one year prevalences, sociodemographic data and the characteristics of migraine, TTH and their subtypes were investigated. The relationship of clinical characteristics with the headache severity was also assessed.
Materials and method
The study was carried out in Kayseri province with a female population, older than 14 years age, of 375 441. Minimum sampling size was calculated as 1100 persons (95% confidence interval, SD:1.6%) estimating migraine prevalence at 8%. Thirteen hundred females aged 15–87 years were selected randomly by cluster and systematic sampling methods in the region, using household cards in primary health centres, which have records of all inhibitants of their regions; 1146 of these females could be reached. Headache symptoms were assessed via a structured face to face interview based on IHS criteria (3). Before each interview, the objective of the study was described and verbal informed consent was obtained. All of the contacted females agreed to be involved in the study. The study was approved by Erciyes University Ethical Committee.
After some introductory questions concerning age, educational and economic level, marital and professional status, subjects were asked if they have any chronic disease diagnosed by physicians and had any important, attention calling (discomforting) headache in the last year period. If headache was reported, they were asked questions about the characteristics of their headaches and some related topics, such as frequency, duration, trigger factors, concomitant symptoms, sleep disturbances, family history, treatments undergone so far, etc. The interviews were performed by medical students, who were trained on the subject by working in the headache polyclinic. After the interview, headache types were determined according to IHS criteria in interviews between neurologists and the students. The diagnosis of other diseases were based on the decisions of primary health centre physicians. The other causes of headache like sinusitis, hypertension were considered and evaluated for probability of being the cause of the headache. In 15 of the cases (1.31%), the headache was thought to be caused by these diseases.
The prevalence ratios of migraine with aura (MWA) and migraine without aura (MWOA), episodic and chronic type TTH were found. The evaluation of the relationship between the prevalences of headache types and the properties of headache patients, such as age, educational and economic level, marital and professional status, residential area and the comparison of clinical characteristics between headache subtypes were achieved by χ2 test. The relationship between clinical characteristics and headache severity were assessed by using Spearman rank correlation analysis.
Results
The sociodemographic properties of migraine and TTH patients: Age, educational and economic level, marital and professional status, residential area of the patients are shown in Table 1.
The sociodemographic properties of all interviewed person and headache patients
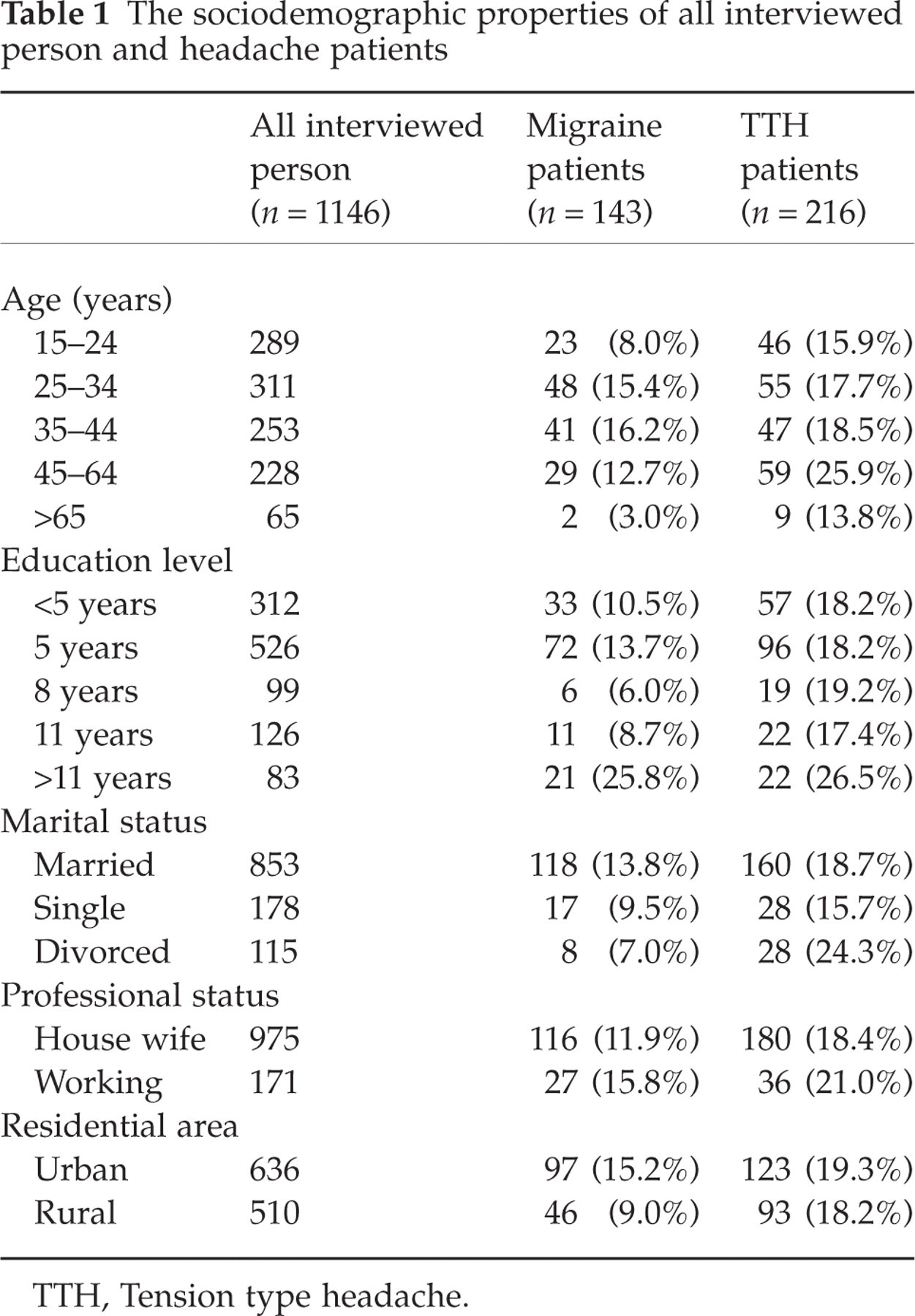
TTH, Tension type headache.
Migraine type headache and sociodemographic properties
One thousand, one hundred and forty-six women were interviewed. Three hundred and fifty-nine (31.3%) of them experienced migraine or tension type headache in the last year period. The 1-year prevalance of migraine was 12.5% (143 patients), comprising 7.3% (84) MWA and 5.2% (59) MWOA.
Migraine prevalence was found to be statistically higher in 35–44 years age group and lower in above 65 years age group compared to the other groups (χ2: 16.38, P < 0.01). Migrainous headache was detected at a higher prevalance in the most educated, university graduates (χ2 : 19.59, P < 0.001), married women (χ2 : 6.04, P < 0.05) and those who were living in urban areas (χ2 : 9.5, P < 0.01). However, professional status and economical level were not significantly related to the presence of migraine type headache.
Tension type headache and sociodemographic properties
The 1-year prevalance of TTH was found to be 18.8% (216 persons), including 144 (12.5%) episodic and 72 (6.3%) chronic type headache.
TTH prevalence was found to be higher in 45–64 years age group (χ2: 10.34, P < 0.05). Chronic tension type headache patients were found to be significantly older than episodic type (Mean age ± SD for chronic and episodic type tension headache: 41.11 ± 15.57, 35.85 ± 12.91, P < 0.01). With respect to the education, chronic type headache was found to be most prevalent (χ2: 6.83, P < 0.05) in the lowest education level.
Frequency of headache attacks
Approximately 73.4% of patients with migraine had 1–4 attacks monthly, while the remaining experienced>4 attacks per month. Fifty-five migrainous patient (38.5% of all migraineurs; 21 MWA, 14 MWOA) had at least 180 attacks per year. Considering TTH, 31.9% of patients had 1–3 headaches per month and 68.1% of patients suffered from headache at least once a week; 33.3% of patients had at least 180 attacks per year i.e. chronic tension type headache.
Duration of headaches
According to the IHS criteria, the accepted duration of a migraine attack in untreated patient is 4–72 h. Twenty-two patients (15.4%) with migraine had duration <4 h. But all of these patients were using drug treatment for their headache attacks. This study showed that the most common duration of migraine attacks (71.3%) was between 4 and 24 h. In TTH, attacks finished within several hours (51.9%), continued throughout the day (22.2%), lasted 1–3 days (14.8%) and 3–7 days in (11.1%) of patients. Episodic tension type headache differed from chronic type in that the attacks usually had the shortest duration, 15 min – several hours (χ2: 10.52, P < 0.05).
Characteristics of headache
Throbbing was observed in 88.8% of migraineurs and 62.0% of TTH patients, while the remaining patients had pressing/tightening sensations. Fifty-three point one percent of migraine patients had unilateral headache. Bilateral headache was reported in 72.7% of TTH patients. In 82.5% of patients with migraine and 43.5% of patients with TTH, the headache was aggravated by routine physical activities.
The characteristics of migraine type headache with aura and without aura are shown in Table 2. Comparison of these characteristics by χ2 test showed throbbing character was found to be more frequent in migraine with aura (χ2 : 4.88, P < 0.05).
The characteristics of migraine with aura and without aura

MWA, Migraine with aura; MWOA, Migraine without aura.
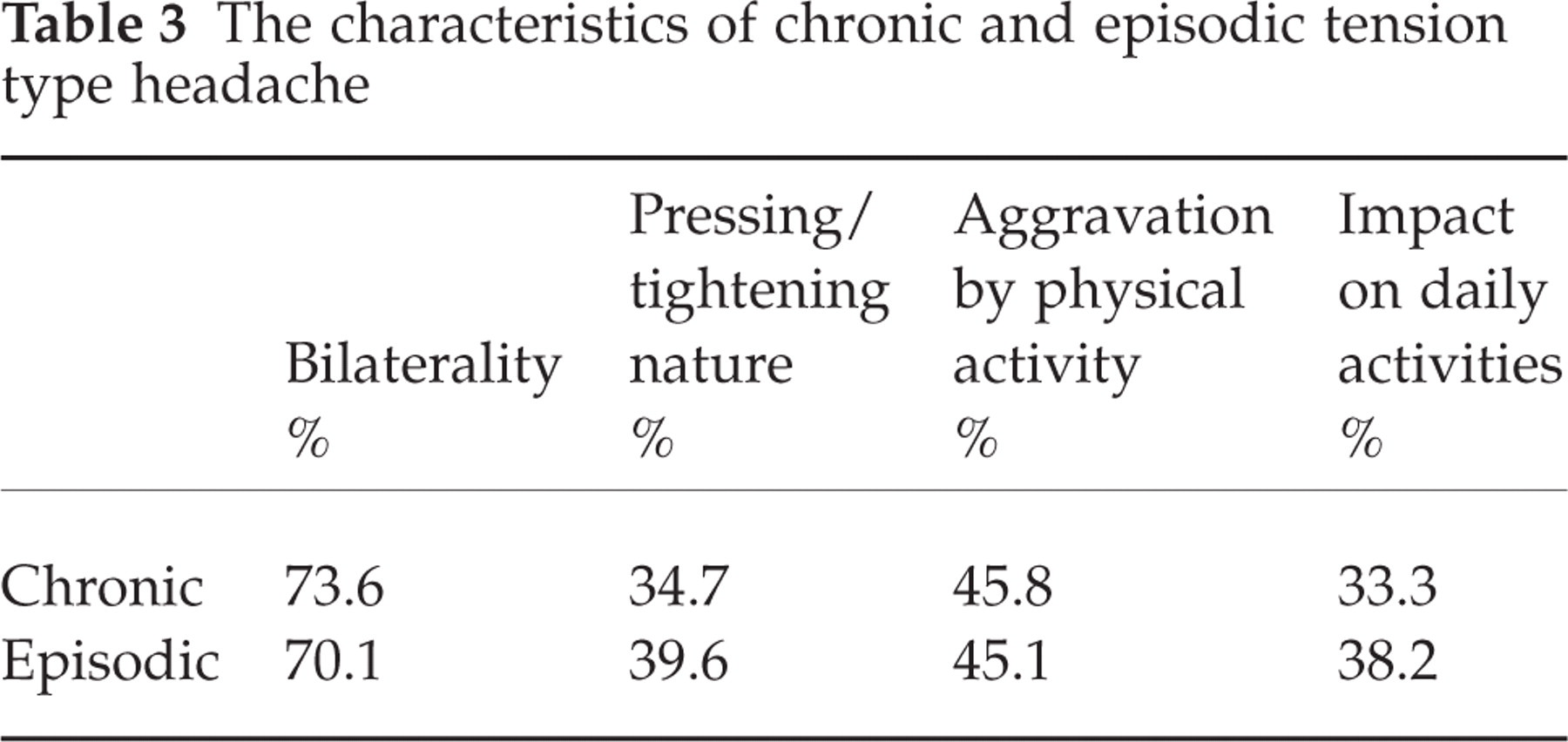
The characteristics of chronic and episodic tension type headache are shown in Table 3. There was no statistical difference (χ2 test) between the two types of tension headache.
The characteristics of chronic and episodic tension type headache
Concomitant symptoms
Phonophobia (85.3%) was the most common concomitant symptom of migraine followed by nausea (80.4%) and photophobia (77.6%). Vomiting was observed in 44.8% of patients with migraine. In MWA, the most common aura was visual disturbance, including scintillation and distortion of image, hemianopia and blurred vision (81.8%), followed by tinnitus/vertigo (67.1%), sensorial symptoms (34.3%) and aphasia (15.4%).
In TTH cases, phonophobia was also the most common concomitant symptom (50.9%). Nausea was observed in 40.7% and photophobia in 14.4% of the patients.
The concomitant symptoms of migraine with and without aura are shown in Table 4 and those of chronic and episodic tension type headache in Table 5. With respect to these findings, there was no difference statistically between migraine with and without aura. However, when similar comparison was made between subtypes of tension type headache, the symptoms of nausea (χ2 : 6.48, P= 0.01), vomiting (χ2 : 5.12, P < 0.05) and phonophobia (χ2 : 4.48, P < 0.05) were found to be more frequent in chronic type tension headache.
The concomitant symptoms of migraine with and without aura

MWA, Migraine with aura; MWOA, Migraine without aura.
The concomitant symptoms of chronic and episodic tension type headache

Trigger factors
The most frequent factors triggering headache attacks were stress (migraine 81.8%; TTH 83.3%), sleep deprivation (migraine 52.4%; TTH 53.2%), fasting or starving (migraine 37.1%; TTH 39.4%), hormonal factors such as menstruation (migraine 35.6%; TTH 24.5%), pregnancy (migraine 16.1%; TTH 6.0%). Various foods did not play any significant role as a trigger factor in migraine patients (cheese 0%, chocolate 1.4%).
32.2% of migraine with aura and 42.4% of migraine without aura reported that their headache was triggered by menstruation. When compared, these frequencies were found not to be statistically different. Five patients (3.5% of migraineurs; 3 MWA, 2 MWOA) reported migrainous type headaches only related to menstruation, so they were menstrual migraine patients.
Impact on daily activities
Routine daily activities were affected in 77.6% of migraine and 37.5% of TTH patients because of the severity of headache. With respect to this factor, no significant difference was found between migraine with and without aura or between episodic and chronic tension type headache.
In tension type headache patients, comparing the presence of impact on daily activities with headache characteristics and concomitant symptoms, a relationship was found between the impact on daily activities and aggravation by physical activities (Spearman ρ: 0.27, P= 0.001). When same comparisons was made in migraine type headache patients, no relationship was found.
In the case of all headache patients, throbbing nature (P < 0.05), aggravation on physical activities (P < 0.001), the concomitant symptoms of nausea (P < 0.01), vomiting (P < 0.05) and phonophobia (P < 0.05) were found to be related with the headache impact on daily activities on Spearman rank correlation analysis.
Sleep and headache
In our study, lack of sleep was reported in 23% of migrainous and 20.8% of TTH patients.
Patient-physician relationship
Seventy-five point five percent of migraine and 56.7% of TTH patients had consulted a physician about their headaches. Fifty-one percent of migrainous patients had known about their migraine.
Treatment measures
The ratio of using drugs in migraine patients during their attacks was found to be 90.9%, while in TTH patients 63.4%. Other important measures were staying alone in a room and sleeping (migraine 86.0%; TTH 66.7%), massage (migraine 38.5%; TTH 31.0%), cold or hot compress (migraine 10.5%; TTH 6.0%).
Family history
Forty-three point four percent of migraineurs had a family history of similar headaches (48.8% MWA; 35.6% MWOA) while a positive family history was reported in 32.9% of TTH patients. In this respect, no significant difference was found between types of headache.
Discussion
This is a population based epidemiological study of female headache patients in Turkey. We tried to evaluate sociodemographic and clinical characteristics of tension and migraine type headache. We further classified the tension and migraine headaches into episodic and chronic tension type and migraine with aura and without aura. The clinical characteristics, concomitant symptoms were evaluated in all subtypes of headache and compared to each other. The attidudes of the patients to headache were investigated.
The rates of fullfilling the criteria of IHS in all types and subtypes were considered and compared. Any significant difference between subtypes were evaluated. The relationships of headache characteristics and concomitant symptoms to the impact on daily activities were especially investigated in the types of headache and in all headache patients. As a result, on the consideration of all headache patient, we found statistically significant relations of some characteristics and concomitant symptoms with the severity of headache. These characteristics and concomitant symptoms were the ones typically related to migraine type headache; throbbing, aggravation on physical activities, nausea, vomiting, phonophobia. In tension type headache, the severity was found to be related with the aggravation on physical activities. This finding was in concordance with the report of Lavados & Tenhamm (4) indicating aggravation of headache pain with headache movements were not specific discriminators of headache syndromes, they were probably more related to pain severity. Any similar relation was not found in migraine type headache.
Migraine is commonly unilateral, pulsating, moderate to severe in intensity, and is associated with nausea, photophobia and phonophobia. In a previous study performed in migraine patients without aura appling to an university hospital in Turkey (5), 58% had pain of pulsating quality, 74% had unilateral pain. Aggravation by routine physical activity was reported to be in the ratio of 96% in the mentioned study. Our results (throbbing 96.6%, unilaterality 49.2% in patients with MWOA) are very different to this study (5), probably because of the difference between the study populations.
The clinical characteristics of migraine was found to be rather similar to those in western countries (6, 7). The lower ratio of vomiting found in Korea and Hungary was not found in our study (8, 9).
We found a significantly higher ratio of throbbing in MWOA when compared to MWA. Such a finding was not reported any where else. Russell et al. (10) stated that they refrained from statistical analysis of comparison between MWOA and MWA because of the difference in inclusion criteria. But we think that the lower occurrence of throbbing in MWA is related to pathophysiology. Cortical spreading depression and cerebral blood flow changes are held responsible for migraine aura. These processes may trigger pain on either side of the head through central connections (11). Rostral brain stem areas play a pivotal or defining role in migraine (12). It seems plausible to consider whether the projections from these brain stem areas to the cortex play a part in initiating the aura and the vascular changes of migraine (11) and whether they cause such a difference of pain between the migraine subtypes.
Tension type headache is characterized as bilateral, pressing/tightening in quality, mild or moderate in intensity, and is not usually aggravated by routine physical activities (13). Our pressing/tightening headache ratio (38%) was lower than those found in previous reports (52%−73.8%) (4, 8). Unilaterality was reported in a high ratio (28.7%) for this type of headache. Exacerbation on physical activities was found in a high ratio (45.4%), a situation stressed in some recent studies (7, 14–16). In our study, photophobia was reported in 14.8% of TTH patients. This finding is in aggreement with those in some other studies (17, 18). We did not find a high ratio of photophobia (82%) as reported by Vanagait & Stovner (19).
In the evaluation of the IHS diagnostic criteria, some authors such as Messinger et al. (20) suggested that evaluation of the criteria seperately instead of the traditional treating of all criteria together. They reported that the overlap of diagnosis in migraine and tension type headache could be diminished if the headache symptoms, such as intensity, duration, quality, aggravation by physical activity, were not combined to build up one common criterion, but each symptom were treated as a seperate criterion (21). Some authors proposed that pain intensity was the most important among the four pain characteristics of migraine without aura. Thus it is helpful in differentiation of migraine without aura and TTH (18, 21). In our study, we found a relationship between severe pain intensity and some other migrainous characters, when we consider all headache patients together. But we could not find such a relationship on consideration of migraine and TTH patients seperately. This finding suggested that when a pain became more severe, it gained some migrainous characters such as throbbing, aggravation on physical activity, nausea, vomiting and phonophobia. However, unilaterality and photophobia were not found to be related to pain intensity.
On comparison of chronic and episodic TTH, nausea, vomiting and phonophobia was found to be higher in chronic TTH. This finding can be considered in agreement with IHS criterion allowing these symptoms more in chronic TTH.
Our 1-year period prevalence of migraine was in agreement with the results of other studies (22). But we found more MWA patients than MWAO, which was surprisingly contradictory to the results of other studies (2, 10, 21, 23). The presence of aura makes recognition of MWA easier. There is a differentiation problem mainly existing between episodic tension type headache and migraine without aura (24, 25). Also, sometimes these two types of headache can exist together in the same patient (26, 27). In this case, in our study, patients might have reported only their tension type headache, which was probably more frequent and recalled as more disturbing, upon answering the question of ‘Do you have any important, attention calling headache?’.
One-year period prevalence of TTH was similar to those reported in other studies (8, 28). The prevalence of chronic type tension headache was reported to be 2–3% in previous studies (6, 28). Our chronic TTH prevalance ratio was higher (6.3%) than these, similar to the study conducted in Turkey before (2).
In our study, migraine prevalence was higher in 35–44 years age group and lower in above 65 years age group. This is in agreement with the results of many studies (14, 29–34). The higher rate of migraine in women of reproductive ages compared with women of other ages was related to endogenous oestrogen (35).
It has been suggested before that migraine is associated with high intelligence and social class (9). Later, in some studies, it was found to be more common in patients with the lowest education and economical level (1, 6, 10, 36–39). We found higher migraine prevalence rate in the most educated and the married patients. However, professional status and economical level were not related to the migraine prevalence rate. In our study, the prevalance was found to be higher in urban areas, in contrast with result of Martin et al. (40). In most of the studies, residential area was not indicated to be related to prevalence.
In the literature, many studies reported that the TTH prevalance peaked between the ages of 30 and 39 and then declined with age (7, 28, 41). In our study, TTH prevalance was found to be higher in the 45–64 years age group. This finding may be related to some social stress in family life in this age group.
We did not find any relationship between other sociodemographic properties and TTH prevalance, in agreement with other studies (42). We detected that chronic type TTH occurred in older and less educated person, similar to the findings of Schwartz et al. (28).
In the literature, almost half of the persons with migraine and more than 80% of persons with TTH were reported to have never contacted a physician because of the headache (22). In females and in migrainous patients, consultation rates were declared to be higher (43). Our consultation rates to physicians were higher than those in previous studies, probably because of our study being conducted in female gender.
We had several limitations in our study. Rasmussen et al. (29) indicated that the way the questions about headache are posed, such as ‘Do you suffer from headache?’ or ‘Do you (ever) have headache?’, could influence the results of epidemiological studies. Presumably, the inclusion of the words ‘suffer from’ was indicated to give a lower prevalance than ‘have’. The same consideration applied, in our study, to asking the question ‘Do you have any important, attention calling headache?’. We asked detailed questions about the most annoying headache of the subjects. This expression might be confounding in some patients having more than one type of headache and might affect the prevalances. But this is a general problem in trials to classify patients into groups according to their headache types.
The interviews are the preferred method in population studies (44). In our study, the medical students, trained by neurologists, performed the interviews and final decisions about cases were made together by the neurologists and medical students. However, it would be better if the interviewers had been neurologists specialized in the subject of headache.
The study was performed in women only, because contact with them was easier than with men because they could be found at home more easily. However, females are a special and important population for headache studies.
Conclusion
This is a population based study searching the clinical characteristics and the sociodemographic factors in migraine and TTH and their subtypes. We believe that it is also interesting, because of the discussion of clinical symptoms in relation to the pain severity.