
Abstract

Introduction
Various diseases can present with a periorbital pain syndrome with or without cranial nerve palsies. The differential diagnoses include, besides primary ophthalmologic diseases (e.g. glaucoma, orbital pseudotumour), painful diabetic neuropathy, Graves’ orbitopathy, any space-occupying lesions of the orbit and the region of the cavernous sinus, thrombosis of the cavernous sinus, giant cell arteritis (GCA), and as a diagnosis of exclusion Tolosa–Hunt syndrome (THS) (1). The presentation of systemic vasculitis as a tumour is rather unusual, but has been reported in declining frequency in cases of Wegener's granulomatosis, GCA, polyarteritis nodosa, Behçet's disease and other various vasculitides (for review see (2)).
We report on a patient who developed a submandibular mass without other clinical or paraclinical findings indicating systemic disease activity during low-dose steroid therapy for suspected THS.
Case report
In December 1999 a 72-year-old female farmer developed an intense, gnawing, constant pain behind and around her left eye which was accompanied by mild lacrimation. She was treated with various eyedrops, which gave intermittent slight relief. In July 2000 the patient fell ill with fever up to 39°C and fatigue, decreased appetite, and weight loss (3–4 kg). The periorbital pain intensified, and she developed a sixth nerve palsy on the left side. At that time ESR was 64 mm/h, CSF, a magnetic resonance imaging (MRI) and a computed tomography of the cranium were normal. The diagnosis of THS was made, and the patient was treated with 20 mg prednisolone once a day. After the first dose of prednisolone the pain lessened. Four days later the patient fully recovered and the ESR normalized. Steroids were tapered after 4 weeks and mild left orbital pain recurred. When steroid treatment was stopped in December 2000 the periorbital pain intensified, and the patient developed a swelling and reddening of the left eye. The symptoms again resolved with 5 mg prednisolone. Steroids could not be tapered without recurrence of pain.
The patient was first seen in our department in February 2001. While on treatment with 5 mg prednisolone, she complained of a constant aching periorbital pain of moderate intensity with intermittent lacrimation and reddening of the eye. Other migraine- or cluster-like symptoms and any symptoms indicating systemic disease were lacking. The detailed neurological, ophthalmological, and internal clinical investigation was normal, except for the complaint of intensified pain during eye movements on the left side, a mild enlargement of the thyroid gland, and a tender, painless submandibular mass approximately 3.5 × 1.5 cm in size, which had developed in the last few months.
Routine blood tests and vasculitis parameters (ESR, C-reactive protein, ANA, ANCA, AMA, C3-, C4-complement factors, cardiolipin antibodies, rheumatoid factor) were negative, except for a reduction of the creatinine clearance (33.5 ml/min). Another cranial MRI (slide thickness 5 mm) showed swelling and oedema of the left Musculus rectus lateralis and the soft tissue in the orbital apex with mild contrast enhancement (Fig. 1). Intracranially, there was a discrete asymmetry of the cavernous sinus. There were no serological markers indicating a reactive vasculitis (HIV, EBV, CMV, herpes simpex, lues). Lyme serology was positive in serum (indirect immunofluorescence test for IgG1 : 256; Lyme Recomb-Blot IgG: p100+, Osp17++), while the CSF again was normal with a negative Lyme serology including a negative CSF-serum quotient. There was no history indicating Lyme disease. A probatory antibiotic therapy with ceftriaxone 2 g/day for 2 weeks did not improve either pain or the swelling. Borreliosis was considered unlikely. Scintigraphy, a needle biopsy of a cold nodule, and normal laboratory findings did not indicate any relevant thyroid dysfunction. Therefore, unilateral Graves’ ophthalmopathy was also considered unlikely.
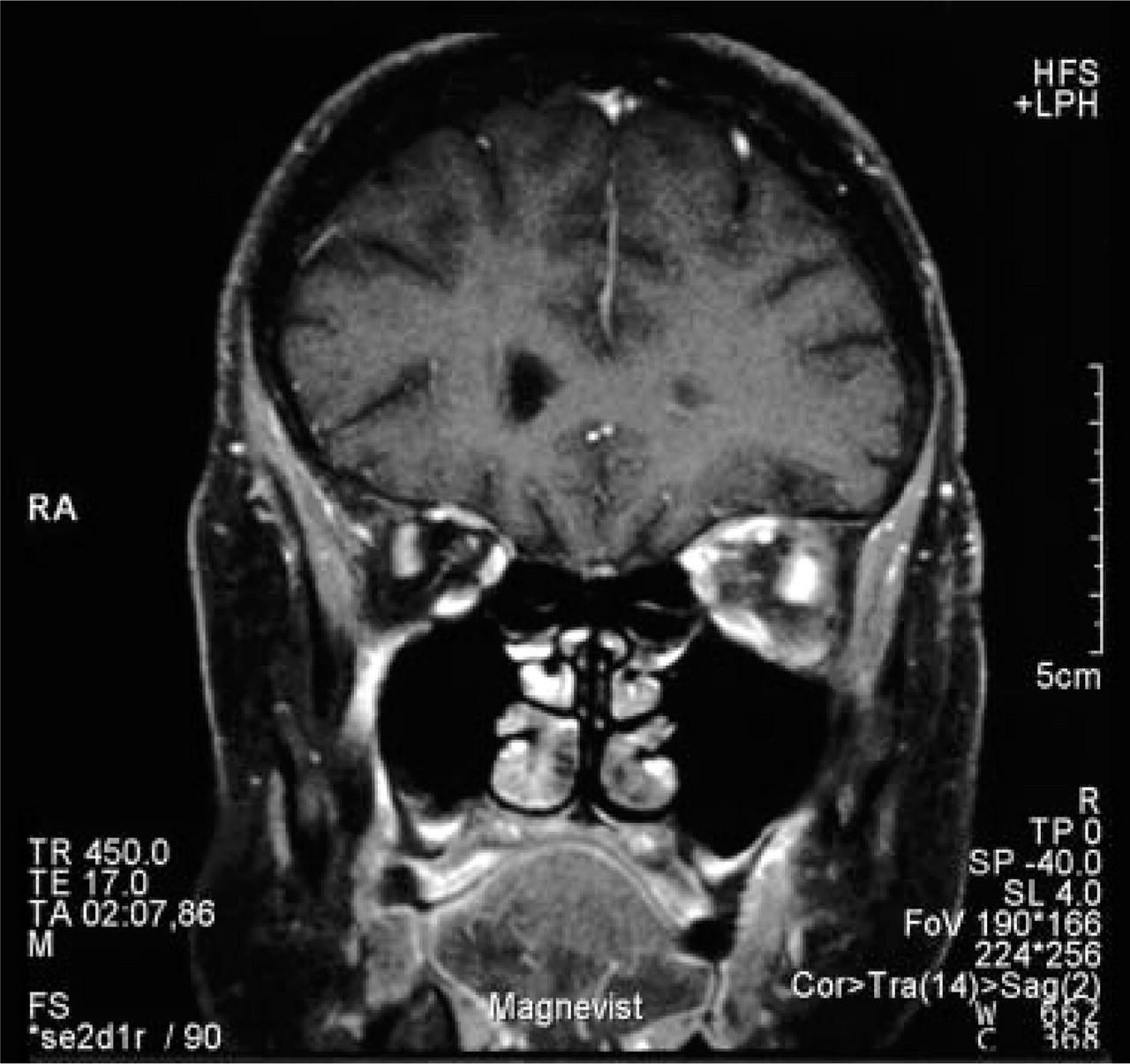
T1-weighted magnetic resonance imaging (coronar plane) showing swelling and oedema of the left Musculus rectus lateralis and the soft tissue in the orbital apex with mild contrast enhancement.
Scintigraphy of the submandibular gland and glucose-PET of the region from the base of the skull to the upper two-thirds of the thorax were normal, but sonography showed a mass adjacent to the submandibular gland.
To arrive at diagnosis and determine the appropriate therapy the submandibular mass was resected. The histomorphological analysis showed a fully developed GCA with transmural inflammation, frequent fragmentation of elastic fibres and subtotal lumen stenosis. The chronic sclerosing inflammation extended widely to the surrounding soft tissues with partial involvement of adjacent lymph nodes, provoking a large tumour-like mass (Fig. 2).

Histological findings. (a) Low power magnification (×35; Elastica van Gieson) of the tumour-like inflammatory process exhibits a lumen-stenosing giant cell arteritis with unusual wide extension of sclerosing inflammation to the surrounding soft tissue. (b) Higher magnification (×300; haematoxylin–eosin) illustrates the active, transmural arteritis with numerous giant cells (arrow), associated with fragmented elastic fibres (arrowhead). The intima is intensely proliferated, provoking subtotal lumen stenosis.
Under treatment with 80 mg prednisone pain completely resolved within 3 days. The dose was tapered over 3 weeks to 30 mg and to overcome the complications of long-term steroid treatment methotrexate (MTX) 10 mg/week was added.
During a check-up in May 2001, the patient was free of complaints (prednisone 7.5 mg/day, MTX 10 mg/week); however, two attempts to reduce the prednisone dose resulted in recurrence of orbital pain. In November 2001 the patient was asymptomatic and the neurological test was normal, but the orbital MRI (slide thickness 2 mm) showed soft tissue in the left region of the cavernous sinus and the superior orbital fissure with mild contrast enhancement. All anatomical structures in the left orbital apex could be differentiated less distinctly than on the right side.
Discussion
Two aspects of our patient with biopsy-proven GCA are of special interest: (i) the difficulty of diagnosing periorbital pain syndromes, and most importantly (ii) the atypical presentation of GCA with an inflammatory orbital process and an inflammatory submandibular tumour.
The patient was first diagnosed to have THS on the basis of the painful sixth nerve palsy with normal neuroradiological and CSF findings as well as on the initially good response to steroid therapy (3). In THS findings consistent with an inflammation can sometimes be visualized in the region of the cavernous sinus, but not primarily in the orbita (4). The cranial MRI findings of our patient were consistent with an orbital inflammation during the first follow-up and showed a mass in the region of the cavernous sinus only during the second follow-up. However, we cannot exclude the possibility that this intracranial mass was missed during the first investigation due to the investigative technique using 5 mm thick slides. However, since MRI findings in THS are regressive during therapy (4), we finally excluded THS not only due to the months long course with incomplete response to steroid therapy, but also due to the MRI findings.
The serological findings raised the question of a Borreliosis-associated syndrome. Ophthalmological and vasculitic manifestations of Lyme disease and even Borreliosis associated with GCA have been reported (5–7), but in our patient the normal CSF findings and the lack of response to antibiotic treatment made GCA associated with Borreliosis highly unlikely.
When the patient was first seen in our department she had no symptoms or signs suggesting systemic disease. The only typical symptoms indicating GCA were the patient's age and the initially good response to steroid treatment. Although ESR and C-reactive protein are the most reliable and well-established variables for monitoring disease activity in GCA (8), these markers can be normal in approximately 20% at the beginning and in approximately 50% of patients during relapses of GCA (8, 9). In our patient an elevation of the ESR was documented only once. Eye pain, diplopia, the submandibular mass and finally the MRI findings consistent with an orbital inflammation were the main findings. All these findings are consistent with GCA, although they are not typical: prospective studies of biopsy-proven GCA reported eye pain in 5.6–8.2% and diplopia in 5.9–11.1% of patients (10, 11). The occurrence of an orbital pseudotumour has been reported in single cases of GCA (12, 13) and the presentation of GCA as a tumour is extremely rare, too. Amongst the few patients with GCA presenting either a breast or an ovarian mass (2), there are only two case reports of a ‘swelling’ of the submandibular gland in GCA in the literature. As in our patient, the swelling was obviously caused by an affected artery that crossed the gland (14, 15), but in this particular case the vasculitic mass even developed during steroid treatment and in absence of other signs or symptoms suggesting a systemic disease.
Therefore we believe, based on the histological pathology, that all findings, the orbital symptoms, the MRI findings and the submandibular mass had one common aetiology: active GCA. Although the course was very unusual for GCA, it finally was not compatible with THS or any other disease causing periorbital pain.