
Abstract

Dear Sir In their recent and very interesting article, Förderreuther et al. (1) discussed the effects and side-effects of the treatment of refractory cluster headache with topiramate (TPM), based on their experience with five patients. They found that TPM caused intolerable side-effects in two patients, leading to the conclusion that its clinical value is limited due to these central nervous system side-effects. After reading their paper carefully, we think the results could be summarized as presented in Table 1.
Efficacy and side-effects of five patients receiving topiramate, as presented in (1)
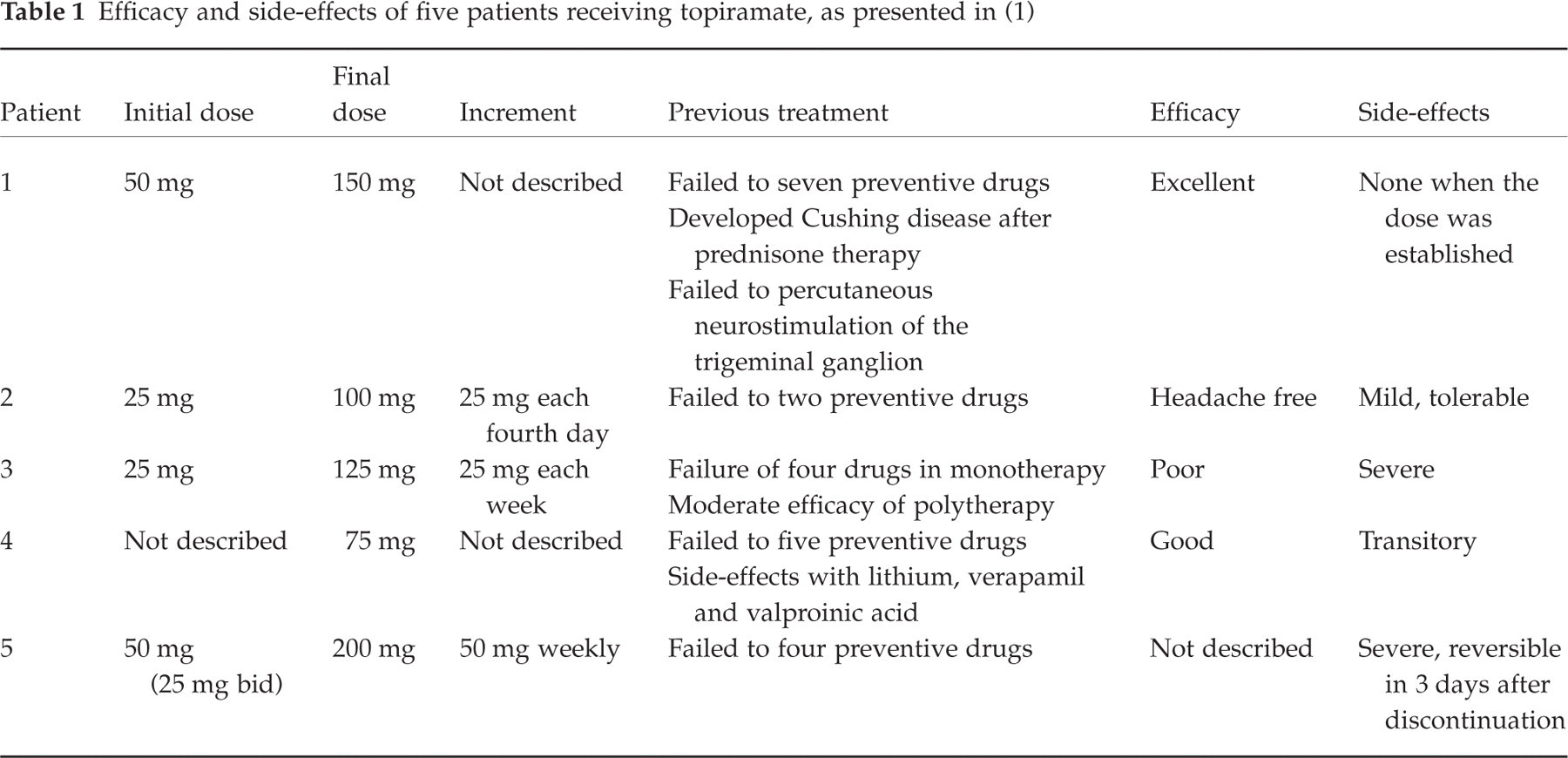
The authors selected otherwise refractory cluster headache patients, some episodic and some chronic, obtaining good results in 3/5 (60%) patients. Although the number is small, this can be considered a good result considering the refractoriness of the sample. Two patients developed severe side-effects (Table 1): patient number 3, who was started with 25 mg and increased by 25 mg per week, and patient 5, who was started with 50 mg and increased by 50 mg per week. Another patient (patient 1), who could tolerate TPM, was also started with 50 mg per day and was increased until 150 mg daily was reached. Patient 4 tolerated TPM and had presented side-effects to three other standard preventive drugs previously. The main question raised by the authors regards the tolerability of TPM.
It is our clinical experience that TPM can be extremely well tolerated when started in doses ranging from 15 mg to 25 mg, and gradually and slowly increased (by a maximum of 25 mg every week or every other week). Our clinical experience is supported by scientific data. TPM was initially suggested to treat refractory migraine in an open study of 37 patients that had failed treatment on a number of preventive drugs (6). The patients used 25–100 mg/day and over a 3- to 9-month follow-up. Just three (8.1%) patients discontinued therapy due to side-effects (light-headedness, ringing in ears and numbness in hands). Edwards et al. (7) studied 30 patients with migraine with or without aura that were randomized to TPM (n = 15) or placebo (n = 15) after completing a 4-week baseline phase. Patients were titrated over 6 weeks by 25-mg increments to a maximum dose of 100 mg bid followed by a 12-week maintenance period. Just three (20%) on TPM discontinued from the study, due to adverse events. The most common side-effects on TPM were paresthesia, diarrhoea, altered taste and somnolence. On the other hand, Krusz and Scott (8) performed an open trial of 28 patients with episodic and chronic migraine refractory to other preventive medications, increasing the dose more aggressively and reaching higher doses, and found a higher rate of adverse events.
We can conclude, analysing the literature, and motivated by this very interesting report of Förderreuther et al., that TPM can be an important option for the treatment of refractory CH, and that it can be better tolerated when doses are started very low and increased slowly.