
Abstract
A total of 26 episodes of V-1 trigeminal neuralgia attacks have been recorded in two female patients. Autonomic phenomena were assessed according to a semiquantitative scale. Attacks lasted 17 ± 5 s. Mild lacrimation without conjunctival hyperaemia, rhinorrhea or ptosis was observed, even in relatively long lasting episodes. This is in clear contradiction with SUNCT (shortlasting, unilateral, neuralgiform headache with conjunctival injection, tearing and rhinorrhea) attacks that are always dramatically accompanied by both lacrimation and conjunctival injection of the symptomatic side from the very onset of symptoms. Carbamazepine provided complete and sustained relief of symptoms in both patients. Herein we will show differential autonomic features of V-1 trigeminal neuralgia vs. SUNCT that will both aid the clinician to distinguish both syndromes and stress that both entities are nosologicaly different.
Introduction
The controversy regarding the nosological independence of SUNCT (shortlasting, unilateral, neuralgiform headache with conjunctival injection, tearing and rhinorrhea) from V-1 trigeminal neuralgia is still a subject of debate. SUNCT syndrome resembles V-1 trigeminal neuralgia in several features (unilaterality of pain, triggering mechanisms, brevity and frequency of attacks) (1, 2). This similitude may be further supported by cases of SUNCT secondary to structural lesions in the posterior phosa (3, 4) where compression of the trigeminal nerve has been taken as pathogenically crucial. Even conventional treatment of V-1 trigeminal neuralgia successfully used in SUNCT, such as Gasser's ganglion compression (5), has been claimed as evidence of the similitude between both disorders. Indeed, reports claiming that SUNCT may be a ‘transformed’ trigeminal neuralgia (6), or that SUNCT could be a trigeminal neuralgia with lacrimation (7), have also been the subject of discussion.
On the other hand, there are numerous clinical differences between SUNCT and trigeminal neuralgia (sex distribution, temporal profile of attacks, refractory periods, autonomic signs and response to treatment) that make us consider them distinct nosological entities (8). V-1 trigeminal neuralgia patients may report mild autonomic signs (usually lacrimation) that tend to appear during severe attacks and after suffering for years from headache (8), whereas SUNCT attacks are characterized by both conjunctival injection and lacrimation appearing in a dramatic and rather ‘explosive’ way from the onset of symptoms.
The principal aim of the present study was to document the autonomic signs in V-1 trigeminal neuralgia in order to obtain objective information to further dissect and clarify the differences with other pain syndromes.
Methods
Patients
Two patients suffering from pure V-1 trigeminal neuralgia (i.e. not extended to V-2 or V-3 territories) were studied during numerous acute episodes. Neurological and ophthalmologic examinations did not reveal underlying abnormalities. Routine blood analysis including ESR and brain/orbital MRI were also within normal limits. Treatment with standard oral doses of carbamazepine completely controlled symptoms. Diagnosis of idiopathic trigeminal neuralgia fulfilled IHS diagnostic criteria (9). Patients gave written consent for withdrawal of treatment, the induction of the attacks and the recording.
Patient 1
A 79-year-old right-handed female with a 8-year history of right primary V-1 trigeminal neuralgia was successfully treated with carbamazepine (600 mg daily). The patient reported having suffered from brief episodes of several seconds of lancinating pain, some of which were accompanied by ipsilateral lacrimation. She denied reddening of the eye, nasal stuffiness, rhinorrhea, changes in pupil size or palpebral width. Attacks could be induced by light tapping of the temple and by blowing the nose.
The patient agreed to stop medication in order to record typical provoked attacks. Three days after discontinuing medication a severe symptomatic period developed. On the day of the recording the patient triggered a total of seven attacks, of which three could be studied in detail. After one day of study carbamazepine was resumed providing complete relief of symptoms.
Patient 2
A 58-year-old right-handed female diagnosed de novo (5 months after the onset of symptoms) with right V-1 trigeminal neuralgia, agreed to allow us to witness several attacks before starting treatment with carbamazepine. Attacks were provoked by light touch of the forehead and temporal area. On the day of the recording and after several hours of observation the patient did not present spontaneous attacks, therefore she proceeded to trigger 23 attacks within a period of 2 h, after which carbamazepine was started and complete response was achieved and sustained for the past 5 years.
Experimental setting
Patients were placed in front of a video camera and asked to provoke attacks based on their previous experience, such as by touching the forehead, temporal area or blowing the nose. Both patients were videotaped and in patient 1 photographs were also taken (Fig. 1). All images were obtained under the same conditions of light, magnification and exposure parameters using a high-resolution camera (ZEISS FF 450 IR Fundus camera) and digital image archiving system (Visupac/System 450 Digital). In order to get a better image of the bulbar and tarsal conjunctiva the lower and upper eyelids were lifted and patients were told to look up. Images were obtained both during and in between attacks. The contralateral eye during the attack and both eyes during the interictal period were used as control. The following autonomic parameters were evaluated: lacrimation, presence of hyperaemia and oedema in bulbar and tarsal conjunctiva, rhinorrhea, ptosis, eyelid swelling and changes in pupil diameter. If a tear was observed during an attack, it was removed with the aid of a tissue before induction of the next episode. Relevant autonomic phenomena were quantified according to a previously described scale (Table 1(10)).
Grading of ocular signs of lacrimation and conjunctival injection (10)

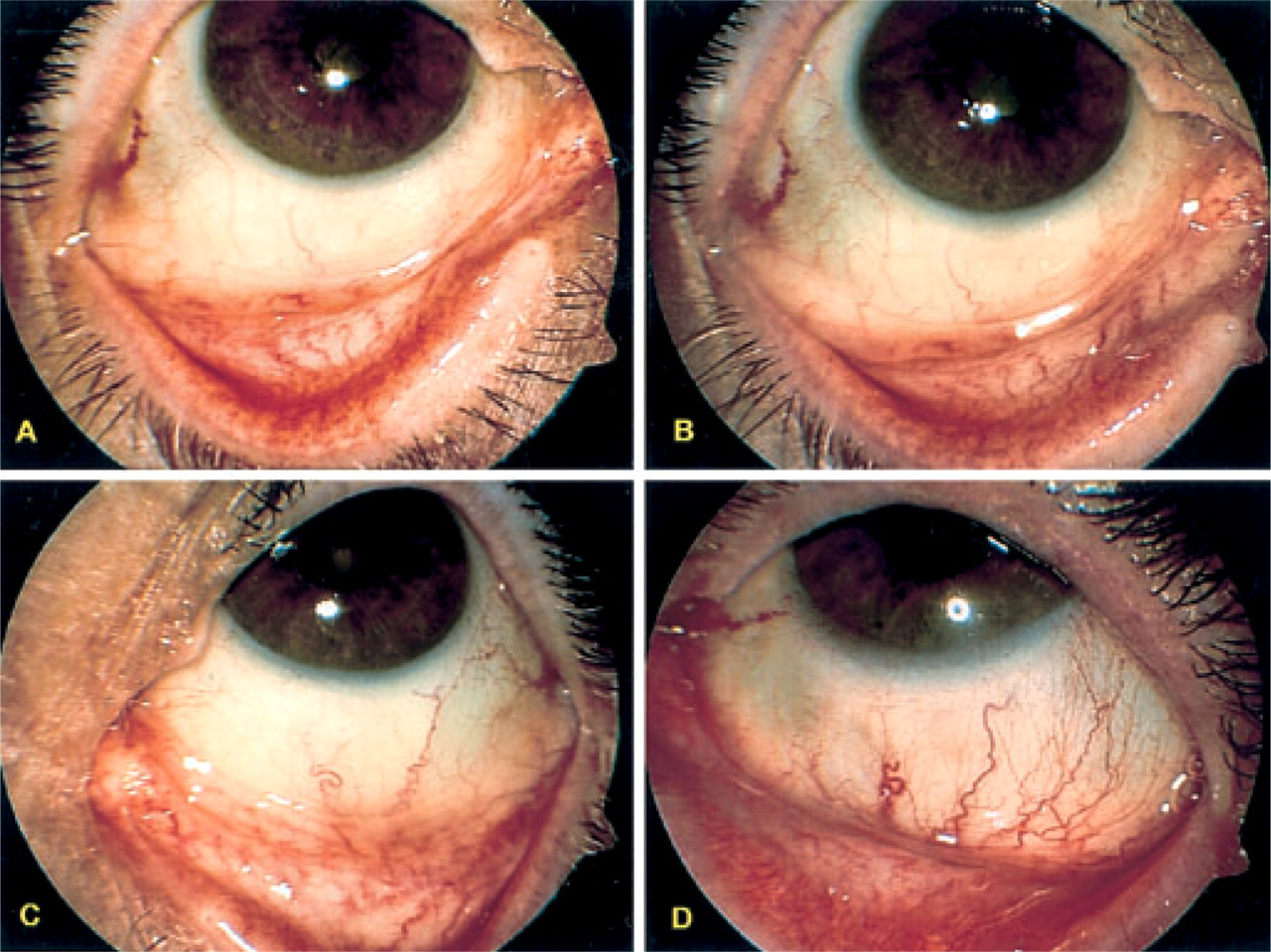
Differential conjunctival signs in V-1 trigeminal neuralgia vs. SUNCT syndrome. Panel A shows the eye ipsilateral to the symptomatic side during a V-1 trigeminal neuralgia attack (patient 1). Note the absence of lacrimation and conjunctival injection. Panel B represents the same eye as in panel A in between two attacks. Panel C is the contralateral eye during the same attack to demonstrate absence of lacrimation or conjunctival injection. Note: the eye shown in panels A–C is from the same patient. Panel D shows the symptomatic eye of a different patient during a SUNCT attack, to demonstrate a clear conjunctival hyperaemia and lacrimation (outer corner of the eye) as opposed to V-1 trigeminal neuralgia. Pictures were taken with a ZEISS FF 450 IR Fundus camera, Panasonic 3 ccd camera (768 × 576 pixels).
Duration of attacks was measured by a stopwatch. Start-time was defined as the time when the patient felt the onset of pain, and stop-time as the time the patient considered pain completely abated. Estimation of the degree of autonomic phenomena observed in real time was independently assessed by two of the authors (JAP, MB). In order to rule out any subjective bias two ophthalmologists (JY and PG) also evaluated the autonomic phenomena by watching the videotapes and photographs. Only close-up images were analysed. Inter-rater reliability was of 100%.
Results
Duration of attacks
A total of 26 attacks were recorded (three in patient 1 and 23 in patient 2). Duration of attacks was 17 ± 5 s (patient 1, 12 ± 4 s; patient 2, 17 ± 5 s). According to the patient's own estimation previous attacks usually lasted less than 10–15 s. However, in patient 2, 61% of the 23 attacks recorded lasted more than 15 s (Table 2). This same patient considered that the triggered attacks were more severe and lasted longer than the apparently spontaneous generated ones.
Semiquantitative estimation of some ocular signs during V-1 trigeminal neuralgia attacks

∗The first digit corresponds to the patient number and the second digit to the number of the attack.
Lacrimation
Assessment of lacrimation revealed production of moderate amounts of ipsilateral lachrymal fluid, enough to be detected by the naked eye of the investigators but insufficient to overflow the lower eyelid and form a tear. During six attacks (23%) a single well-formed tear hardly leaving the eyelid was documented.
Conjunctival hyperaemia
In none of the observed attacks in patient 2 was there any appreciable conjunctival injection. However, in patient 1 we observed a selective mild injection of the tarsal conjunctiva on the symptomatic side (Fig. 1A) without obvious hyperaemia of the bulbar conjunctiva. In this case this selective hyperaemia could either be explained by retraction of the symptomatic inferior eyelid in order to take the photographs or secondary to an antialgic contraction of the eyelids.
Other autonomic signs
There was no ptosis, engorgement of the vessels of the eyelids, swelling of eyelids, changes in pupil size, rhinorrhea or reported nasal stuffiness in any of the attacks recorded.
Contralateral eye and interictal period
The contralateral eye did not show changes in any of the parameters evaluated during pain, and did not differ from its appearance during the interictal period (Fig. 1C). The affected eye during the interictal period revealed no asymmetries with the contralateral eye (Fig. 1B).
Discussion
We had the opportunity of witnessing and recording multiple stereotypical V-1 trigeminal neuralgia attacks, providing an objective assessment of the attacks and avoiding the patient's recall bias. In a total of 26 episodes of V-1 trigeminal neuralgia attacks, recorded paucity of autonomic signs has objectively been demonstrated, even in relatively long lasting episodes. Although caution is required as only two patients were studied, it seems that in V-1 trigeminal neuralgia, lacrimation, when present, is meagre and hardly ever accompanied by conjunctival injection (8). This is in clear contradiction with SUNCT attacks that are always dramatically accompanied by both lacrimation and conjunctival congestion of the symptomatic side from the very onset of symptoms, Table 3 (1, 2).
Summary of differential autonomic features between V-1 trigeminal neuralgia and SUNCT estimated by the same semiquatitative method (10)

∗Twenty-two attacks in three patients (10).
†Twenty-six attacks in two patients, present series.
Generally, SUNCT attacks last three times as long as V-1 trigeminal neuralgia attacks (11). We had the exceptional opportunity of witnessing 23 V-1 trigeminal neuralgia attacks lasting more than 10 s (range 12–28). These unusual relatively long-lasting attacks have given us the chance to compare the pain and accompanying features of V-1 trigeminal neuralgia attacks vs. equivalent shorter episodes of SUNCT. This is important because attacks of V-1 trigeminal neuralgia of long duration may overlap the shortest SUNCT attacks (10–20 s) (11). By doing so we ruled out any uncertainty regarding the paucity of local autonomic signs in V-1 trigeminal neuralgia due to the short duration of the attacks (less than 10 s) (8). It should be noted that it is widely acknowledged that SUNCT attacks lasting 10–20 s already present full-blown autonomic accompaniments 1 to 2 s after onset of pain (1). Our data show the almost complete absence of autonomic signs in even relatively long attacks of V-1 trigeminal neuralgia, clarifying that duration of the episode is independent of the accompaniments, and nosologically separating V-1 trigeminal neuralgia attacks from other similar cephalgias.
It has been proposed that in some patients SUNCT might have evolved from trigeminal neuralgia (6, 7). The question is whether it is possible that both disorders consecutively appear in some patients, as has been reported in cluster–tic (12, 13) and CPH–tic (14, 15), or rather a unique polymorphous condition may exhibit two clinical variants (V-1 trigeminal neuralgia and SUNCT). In V-1 trigeminal neuralgia attacks, as opposed to SUNCT attacks, autonomic signs appear either occasionally or are present to a minor extent (8). Although in theory incomplete attacks of SUNCT with less overt autonomic accompaniments might well occur with what we know so far, V-1 trigeminal neuralgia and SUNCT attacks seem to represent two different disorders (8).
The clinical differences described above between SUNCT and V-1 trigeminal neuralgia could well follow a difference in the threshold for activation of only the trigeminal system, as in V-1 trigeminal neuralgia or the additional recruitment of other systems such as the parasympathetic, that would lead to the appearance of more or less profuse conjunctival injection, lacrimation and rhinorrhea as observed in SUNCT. The cessation of the attack and following refractory period in V-1 trigeminal neuralgia suggests the presence of a strong central inhibitory system that is lacking or malfunctioning in SUNCT. Recently, the reported activation in the hypothalamus during a SUNCT attack has been claimed as pathogenically relevant as the hypothalamus has connections to the superior salivary nucleus, responsible for the autonomic signs observed (16). Nevertheless, we still face the problem of a difficult diagnosis in these patients unless future biological markers are available.
In conclusion, there seem to be quantitative and qualitative differences regarding local autonomic accompaniments between SUNCT and V-1 trigeminal neuralgia. According to our data, absence of conjunctival injection and mild lacrimation characterize V-1 trigeminal neuralgia, while marked lacrimation and conjunctival injection appear in tandem during SUNCT attacks, and both signs should, in the future, be incorporated together as one solid diagnostic criterion of SUNCT as it strengthens the differences with V-1 trigeminal neuralgia. However, further research is necessary as inter- and intraindividual differences in autonomic signs accompanying V-1 trigeminal neuralgia may occur.
Footnotes
Acknowledgements
The work described here was supported in part by the PPA Humphrey-IHS-GlaxoSmithkline 2000 Research Fellowship (MSDR).