
Abstract
Raeder first described Horner's syndrome with ipsilateral head pain due to paratrigeminal organic disease, but most subsequent reports of this syndrome were idiopathic. Our recent case prompted a review of past reports of idiopathic Raeder's syndrome. Because in recent years the features of Raeder's syndrome have been recognized as common manifestations of carotid artery dissection, we divided the cases into those with and those without carotid imaging studies. The classifications and differential diagnoses are discussed. Sixteen cases with carotid imaging studies were not very different from the 28 cases without such studies. Most studies were performed several weeks after onset of symptoms and carotid dissection could not be definitely excluded in any case. In most cases of idiopathic Raeder's syndrome, carotid artery dissection was not considered and in no case was that condition definitively excluded. People with Raeder's syndrome not associated with a paratrigeminal organic lesion probably have a disease of the carotid artery. Because of the different criteria and classifications of Raeder's syndrome it is best to relegate this eponym to history.
Introduction
In 1918 and 1924 Raeder described five patients presenting the clinical picture of Horner's syndrome and ipsilateral head pain (1, 2). Because four of Raeder's five cases were due to organic disease affecting cranial nerves adjacent to the trigeminal nerve, he and others localized this syndrome to the paratrigeminal region. Thereafter the clinical features of Horner's syndrome and ipsilateral head pain were termed Raeder's syndrome and often carried the additional rubric of paratrigeminal syndrome.
Raeder's syndrome has been a confusing term. Some believe the term ‘Raeder’s syndrome' should be reserved for those rare diseases of the paratrigeminal area in the middle cranial fossa. Others use the term to include all cases with features of a painful Horner's syndrome and several subclassifications have been suggested.
Most reports of Raeder's syndrome were idiopathic and the courses were benign. Many older reports of Raeder's syndrome meet the International Headache Society (IHS) criteria for cluster headache (3). A recent case of Raeder's syndrome appeared to be free of organic disease and prompted a review of the benign/idiopathic form of this syndrome. We believe that Raeder's syndrome may well be benign but that idiopathic cases are probably due to unrecognized carotid artery disease, especially dissection. The features of our case are listed in Table 1. Because there is no general agreement about the definitions and subclassifications of Raeder's syndrome it would be advisable to relegate the eponym to history and analyse these syndromes by studying both the head and the neck.
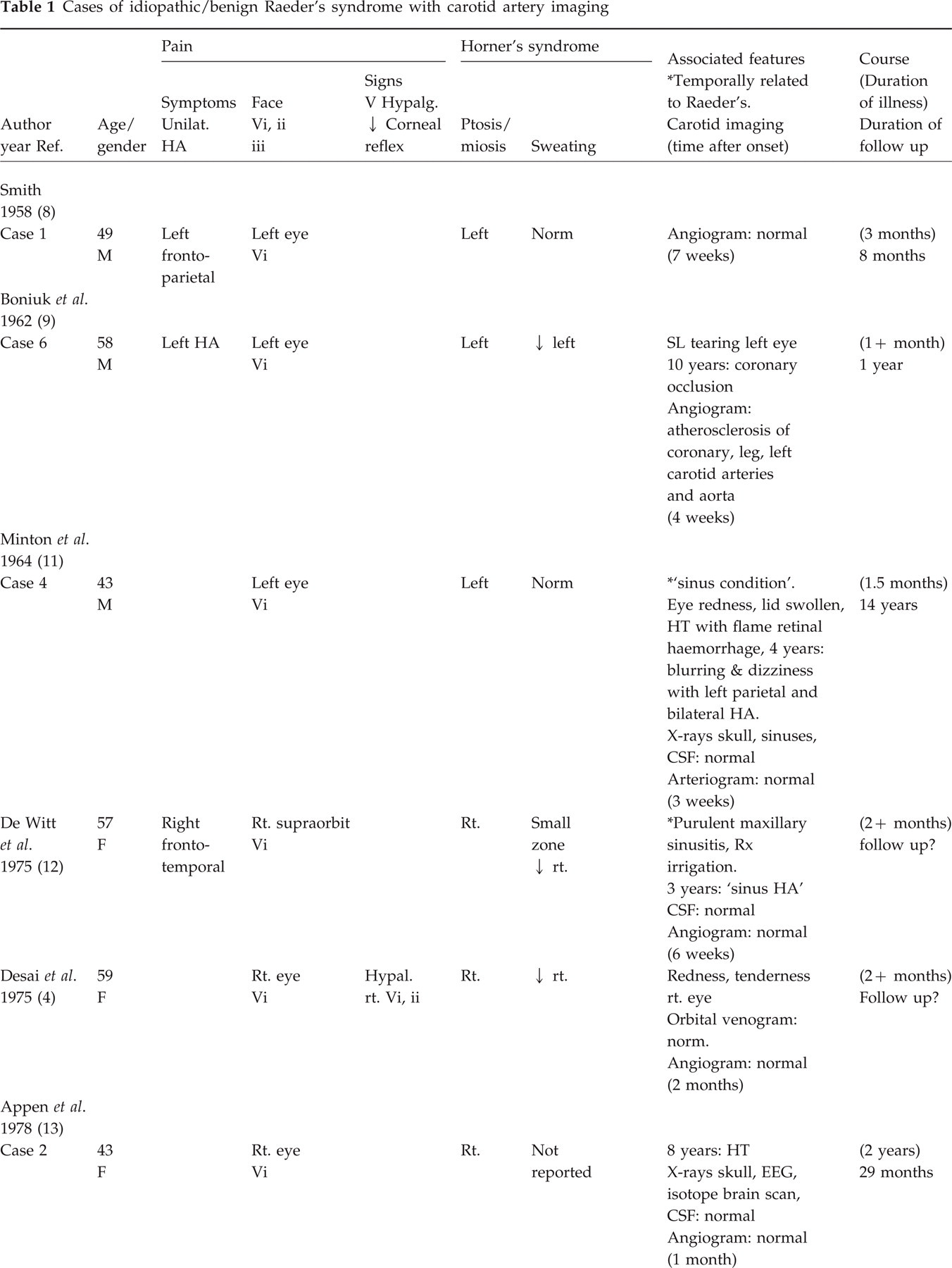
Cases of idiopathic/benign Raeder's syndrome with carotid artery imaging

Methods
We added our case to a review the literature of the benign/idiopathic form of Raeder's syndrome presenting with Horner's syndrome and ipsilateral head pain (Tables 1 and 2). The pain was within or included the ophthalmic division of the trigeminal nerve (orbit or frontotemporal area or both) and there was associated ipsilateral ptosis and miosis, with or without associated anhydrosis. Past reports of idiopathic/benign forms of Raeder's syndrome included signs of ophthalmic division trigeminal nerve dysfunction as manifested by decreased corneal reflex and altered response to pain and touch. In four or five cases maxillary division hypalgesia was also reported (4, 5). In our review we included cases with these signs. (The associated features of these patients were not different from the majority.) Because carotid disease had not been an important consideration until recent years, we divided the cases into those with and those without carotid artery imaging. Since false-negative carotid studies may be due to healing of an arterial dissection we tabulated the time of the carotid imaging since the onset of symptoms. We documented the major features of the syndrome, the gender and age of onset. In addition, features temporally related to the syndrome, other important findings and the duration of the illness at follow up were noted.
To rule out organic paratrigeminal disease cases were excluded if there was evidence of cranial nerve involvement other than trigeminal. Cases of carotid artery disease proven by imaging studies were also excluded. One case of internal carotid artery stenosis was excluded because the stenosis might have been due to dissection (Grimson case 12) (6). At least one case was excluded because the clinical features suggested the diagnosis of carotid artery dissection (7). Some cases reported as examples of Raeder's syndrome were excluded because they appeared to be better classified as cluster headache. A few cases were omitted from our tabulation when the diagnosis of cluster headache appeared to be as probable as Raeder's syndrome (e.g. Smith case 4) (8) or when clinical features or laboratory data suggested underlying organic disease (e.g. Bonuik & Schlezinger case 3 and Hubert) (9, 10).
Results
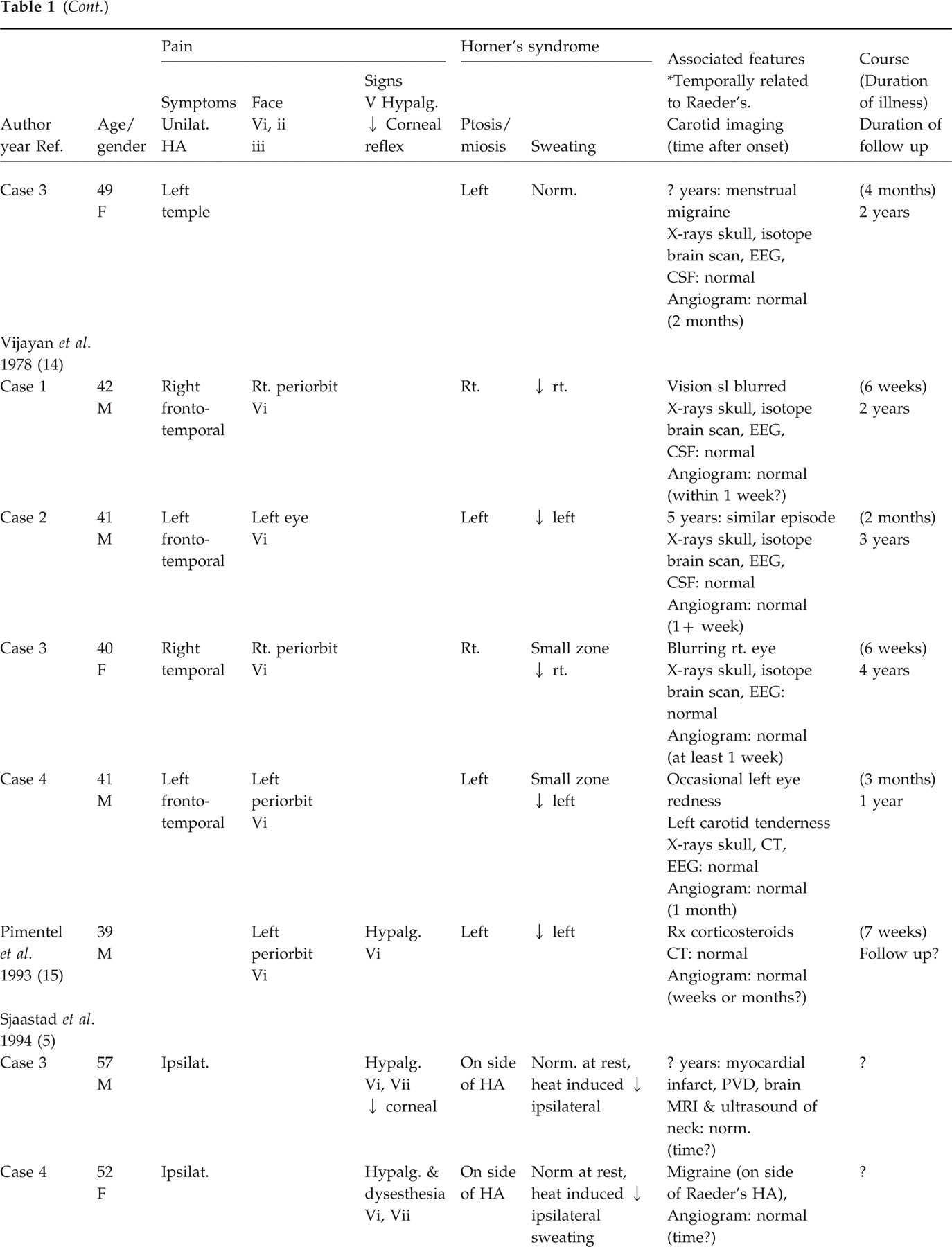
Of the 16 cases with carotid imaging all but two occurred in the fifth and sixth decades of life (4, 5, 8, 9, 11–15) (Table 1). The youngest patient was 33, the oldest 59. Although Raeder's syndrome was once thought to occur almost exclusively in males, the male-to-female ratio was 9:7. The site of pain by definition included the ophthalmic division of the trigeminal nerve but sometimes pain extended to the temple or parietal areas or the description was not specific. Signs of ophthalmic division trigeminal nerve dysfunction occurred in four of 16 patients and included diminished corneal reflex (n = 1) and hypalgesia (n = 4). Hypalgesia in the maxillary division was noted in three patients.
All patients had ptosis and miosis; a complete Horner's syndrome with diminished sweating was noted in 12 of 16 cases. In three cases the decreased sweating was noted only in a small zone above the eyebrow. In four cases including ours, anhydrosis was not evident in a normal setting but it was evident after heat or exercise. Because sweating is not routinely tested it was specifically noted to be normal in three patients.
There was no pattern to the different features that were often associated with the syndrome. Conjunctival injection or tearing were reported in four cases but the pattern did not conform to the criteria of cluster headache. Blurring of vision was noted in two, but there were no associated signs. A history of inflammatory disease, i.e. purulent sinusitis, was temporally associated with the onset of Raeder's syndrome in one patient. Another patient experienced tenderness over the carotid artery but there was no other evidence of carotid dissection. Hypertension or cardiovascular disease was found in five patients, not unexpected at this age group. A history of migraine in four patients did not exceed the expected prevalence of this common condition. Minor head trauma was rarely reported and not temporally related.
The duration of illness was noted in 13 of the 16 cases. Symptoms persisted from 1 to 3 months in most instances; pain persisted for as long as 4 months and 2 years in two cases. Clinical details regarding long-term follow up were usually absent, but follow-up periods from 8 months to 14 years supported the benign non-recurrent nature of this condition. Occasionally residuals of the Horner's syndrome persisted. A carotid angiogram was abnormal, showing atherosclerosis, in only one of the 16 cases, but the timing of the studies was usually several weeks after onset of symptoms.
There were 28 cases that appeared to be benign manifestations of Raeder's syndrome, but they were not included in the primary group because carotid disease was not excluded by imaging studies (5, 6, 8, 9, 11, 13, 14, 16–19). Analysis of this group (Table 2) revealed features similar to the primary group (Table 1). All but four patients were in the third, fourth and fifth decades of life, the youngest 27, the oldest 70, but nine of 28 were in the third decade while only two of 16 in the primary group were in that age group. The male-to-female ratio was 23:5. Ipsilateral headache sites were usually not well described; they were rarely beyond the ophthalmic division of the trigeminal nerve. Signs of trigeminal nerve dysfunction (ophthalmic division) were present in 10. Diminished sweating as part of the Horner's syndrome was noted on examination in five patients; in three of the five decreased sweating was noted after heat exposure. In eight sweating was noted to be normal.
Cases of idiopathic/benign Raeder's syndrome without carotid artery imaging



?, Unknown; ↓, decreased; ↑, increased;
temporally related to Raeder's syndrome; #, symptoms of pain consistent with Raeder's syndrome, details not stated—dysesthesia, if noted, is subjective; &, and; BP, blood pressure; CSF, cerebrospinal fluid; CT, computed tomogram; HA, headache; HT, hypertension; hypal., hypalgesia; hypesth., hypesthesia; MVA, motor vehicle accident; PVD, peripheral vascular disease; ref., reference; rt., right; Rx, treatment; sl, slightly; unilat., unilateral; URI, upper respiratory infection; Vi, ii, iii, trigeminal nerve dermatomes.
Of the features temporally associated with Raeder's syndrome an inflammatory illness was most common: abscessed tooth (n = 1), diseased tooth (n = 1), pneumonia (n = 1), purulent sinusitis (n = 1), upper respiratory infection (n = 4). Hypertension was noted in eight patients, slight head trauma in two. The duration of the illness, when noted, ranged from 3 weeks to 6 months.
Discussion
Summary of clinical features
Because carotid artery disease may present with or be manifested by the features of Raeder's syndrome we divided this compilation of the benign apparently idiopathic form into those with and without imaging of the carotid artery (Tables 1 and 2). The two groups were similar in age; their clinical features and associated conditions, with rare exceptions, were similar. Patients were in the fourth, fifth and sixth decades of life and the male-to-female ratio was approximately 2.7:1. All had symptoms (pain) within the ophthalmic division of the trigeminal nerve and one third had associated trigeminal nerve signs. All patients had ptosis and miosis but diminished sweating was noted in less than one-third of the patients. The headache usually cleared after 1–3 months but residual features of Horner's syndrome might persist. There were no instances of recurrence of the syndrome. In a few cases the onset appeared to be temporally related to an inflammatory illness.
Classification and diagnosis
The essence of Raeder's syndrome is Horner's syndrome and ipsilateral head pain. Raeder's first patient had paratrigeminal cranial nerve signs due to a middle cranial fossa neoplasm and some believe that the syndrome should be limited to paratrigeminal lesions. But paratrigeminal disease is rare and the term has been used when oculosympathetic paresis and ipsilateral head pain were not associated with paratrigeminal disease. Some of these cases were due to disease of the carotid artery but the majority did not have an obvious cause and the course was benign. As a result, Raeder's syndrome was divided into two groups: those associated with organic disease and those without. Idiopathic/benign Raeder's syndrome was termed Group II by Bonuik & Schlezinger, and Group IB and II by Sjaastad et al. (5, 9). The condition was characterized as pain in the distribution of the ophthalmic division of the trigeminal nerve (Vi) with partial or complete Horner's syndrome with or without signs affecting Vi. Dysesthesia might accompany the pain. The signs might be hypalgesia or hypesthesia within the distribution of the ophthalmic division of the trigeminal nerve with or without impairment of the corneal reflex. On rare occasions sensory defects within Vii were also reported.
Differential diagnoses
There are several considerations in the differential diagnosis of benign/idiopathic Raeder's syndrome. Most important are diseases of the carotid artery (occlusion (14), aneurysm (20), inflammation (21), fibromuscular dysplasia (22), and especially dissection). It is common for Raeder's syndrome, unilateral head pain and Horner's syndrome to be the presenting features of carotid dissection and they may be the only features of this condition (23–25). In large series of carotid dissection symptoms of Raeder's syndrome were prominent. Hart & Easton analysed 140 cases of extracranial carotid dissections published between 1975 and 1983 (23). An ipsilateral Horner's syndrome occurred in 46% of patients and head or neck pain in 83%. In Mokri's series of 70 patients 53% had oculosympathetic palsy, 84% had headache and 17% presented with both features (24). In the largest review of carotid dissection to date, Biousse and associates reported Horner's syndrome with ipsilateral head pain in 44% (65 of 146 cases) and it was the only feature in half of the patients, the other half having ischaemic signs (25). A Horner's syndrome with ipsilateral head pain was noted in as high as 58% of other large series (25). Although carotid dissection must be ruled out by imaging techniques when considering the diagnosis of Raeder's syndrome, false-negative carotid studies are not rare (14). False-negative studies may be due to delay between the onset of the dissection and the tests with healing of the dissection, the type of dissection (e.g. subadventitial with little or no narrowing of the lumen) and other factors. Doppler studies evaluate the proximal carotid rather than the more distal portions where dissection usually occurs (25).
In our review at least one case (Grimson case 12) was excluded because the report of moderate stenosis of the internal carotid artery may have been due to dissection (6). There were rare suggestions of carotid disease in our compilation (Tables 1 and 2). Tenderness of the carotid artery was noted in one patient. Blurring of vision was reported in two patients. Although carotid imagings were normal in 15 of 16 patients (one showed atherosclerosis, Table 1), the timing of the studies (when reported) was usually late (1–2 months) after the onset of symptoms. Carotid imaging in our case was completed within a week of onset of symptoms but the imaging was by ultrasound. In two other cases radiographic angiography was probably performed relatively early (exact times uncertain) and the studies were negative.
In earlier decades there were many cases labelled as Raeder's syndrome that would now be diagnosed as cluster headache. Several features are common to both conditions but there are distinguishing characteristics. Anhydrosis of Horner's syndrome may or may not be present in Raeder's syndrome but, paradoxically, forehead and facial sweating is more likely to occur during cluster headache. Redness and tearing of the ipsilateral eye, typical during cluster headache, were rarely reported in Raeder's syndrome but the temporal relationship to the syndrome was problematic (4, 9, 11, 14). Ipsilateral nasal congestion and rhinorrhoea, also typical of cluster headache, were not reported in cases of Raeder's syndrome. In contrast to the brief (15 min to 3 h) periodic excruciating pain of cluster headache, the pain of Raeder's syndrome is continuous or almost so and the pain is less intense. While the periodicity of cluster headache was first noted by Harris in 1926 it was not until 1952 that Kunkle emphasized the clustering pattern (26, 27). The cluster pattern and the brief duration of the cluster headache attack distinguishes it from Raeder's syndrome. Other variants of cluster headache, chronic and episodic paroxysmal hemicrania, are also differentiated from Raeder's syndrome by the features noted above; the headache duration of these conditions is even shorter than that of cluster headache.
Hemicrania continua is a rare primary headache that, as the name implies, is locked to one side. There may be mild ipsilateral autonomic features associated with this headache and very rarely an associated partial Horner's syndrome has been reported (28). In contrast to hemicrania continua, the course of Raeder's syndrome is finite (weeks or months). Hemicrania continua is fully responsive to indomethacin therapy. (Admittedly none of the patients tabulated as having Raeder's syndrome received such therapy. Conversely the cases of hemicrania continua are not usually evaluated for carotid disease.)
In the Tolosa–Hunt syndrome ophthalmoplegia accompanies ocular pain. There may be involvement of the trigeminal nerve in Tolosa–Hunt syndrome and rarely Horner's syndrome or impaired sympathetic innervation of pupil causing miosis (29), but the ophthalmoplegia distinguishes it from Raeder's syndrome.
Site of disease
The location of the lesion in the benign/idiopathic form of Raeder's syndrome has been speculative. The common carotid artery is implicated in those cases with complete Horner's syndrome. The internal carotid artery is implicated in those without impaired facial sweating since sympathetic pathways to the sweat glands ascending the common carotid artery from the cervical sympathetic ganglia follow the external carotid artery and would not be affected by disease of the internal carotid artery or its branches. In some cases, however, sympathetic nerves to sweat glands travel with the supratrochlear and supraorbital branches of the ophthalmic branch of the internal carotid artery. Interruption of these fibres explains the small supraorbital zone of anhydrosis found in some cases (9). Others postulate denervation of sweat glands in the medial aspect of the forehead innervated by the sympathetic plexus on the internal carotid artery (5). As Sjaastad et al. emphasized, decreased forehead sweating is often not evident on standard examinations but found with heat-provoked sweating or other sweating tests (5).
Vigayan & Watson were so convinced that the site of disease was pericarotid, that they used the term ‘pericarotid syndrome’ (14). If all idiopathic forms of Raeder's syndrome are due to unrecognized carotid artery disease then one must consider not only false-negative carotid artery studies, but also differences in the clinical features of carotid dissection vs. that of the benign Raeder's syndrome. Although carotid dissection and Raeder's syndrome may present the same clinical features, half or more patients with carotid dissection experience retinal or brain ischaemic signs and the duration of pain is relatively short (median of 5 days) (22).
Evaluation
Because carotid artery dissection often evokes symptoms of Raeder's syndrome, the integrity of this vessel must be established. The carotid artery may be studied by radiographic angiography, Doppler, magnetic resonance imaging (MRI) or magnetic resonance angiography (MRA) (30, 31). None of these studies is infallible, for dissection may be evident in one study but not another, or dissection may quickly resolve before the study is accomplished. Nevertheless MRI/MRA are the diagnostic studies of choice at this time (31). Indeed, because subintimal or subadventitial dissection may not narrow the lumen, the diagnosis may be made only by MRA of the neck. Cranial nerve involvement beyond the trigeminal warrants an MRI or angiography or both to establish paratrigeminal disease. (But note that the trigeminal and other cranial nerves may be affected by carotid dissection (32).)
Conclusion
The syndrome first described by Raeder consisted of partial or complete Horner's syndrome, ipsilateral head pain within the trigeminal nerve distribution and signs of adjacent cranial nerve disease, hence the term paratrigeminal syndrome. Only the first of his five cases were due to a neoplasm in the middle fossa. Most subsequent reports of Raeder's syndrome did not have paratrigeminal cranial nerve involvement, had a benign course and were labelled as ‘Group II’ (Bonuik & Schlezinger) or Group IB and II (Sjaastad et al.). We believe the cases in this benign group are usually due to carotid disease. Headache alone or an isolated Horner's syndrome may be the only manifestations of carotid dissection (33–35). The majority of cases that were classified as benign idiopathic Raeder's syndrome did not have evidence of paratrigeminal disease and were not studied for the possibility of carotid disease (Table 2). In most of those who were studied (Table 1) the tests were late in the course of their illness, permitting resolution of carotid dissection; none were studied by MRI of the neck. In summary, there have been no cases classified as benign Raeder's syndrome in which carotid dissection was definitively excluded.
The classification of headache and face pain by the IHS does not recognize Raeder's syndrome because ‘… Raeder’s paratrigeminal neuralgia (is) not (a) specific diagnosis, but a syndrome indicating a particular location of intracranial pathology' (3). The classification of chronic pain by the International Association for the Study of Pain recognizes two groups of Raeder's syndrome with and without parasellar cranial nerve involvement, as proposed by Bodiuk & Schlezinger (9, 33, 36). On the basis of this review it would appear that the IHS statement is closer to the mark, though the search for pathology should include the neck as well as the head. Carotid artery disease is the most probable cause of Raeder's syndrome when paratrigeminal signs are absent.
The confusion about this syndrome is due to subclassifications and divisions of diseases that have a kernel of similarity but disparate sites and aetiologies. The best way to eliminate the confusion is to relegate the term ‘Raeder’s syndrome' to the history of the twentieth century.