
Abstract

Introduction
Migraine is generally considered to be an inherited brain disorder of the aminergic pathways related to sensory control. It involves activation of the trigeminovascular system which results in headache. Investigations that have been carried out in several laboratories have demonstrated that peripheral and central serotonin (5-HT) receptors play a crucial role in the pathophysiology of the disease. The development of a new class of effective antimigraine compounds, the triptans, 5-HT1B/1D receptor agonists (1), has confirmed the involvement of these receptors and posed new questions concerning the relevance of their central effects to symptom resolution.
While researchers are interested to find out the nature of the mechanisms by which these medications work, patients expect complete and fast relief of pain (2). The results of this population-based study also indicate that patients expect the medication to eliminate the possibility of recurrences, have few side-effects, relieve associated symptoms and be convenient to use (2). This is consistent with the current recommendations of the Clinical Trials Committee of the International Headache Society (IHS) (3), and pain free will be the recommended endpoint in the new revision of its guidelines. This paper reviews data from the development programme for rizatriptan, a 5-HT1B/1D agonist (4), in relationship to these outcomes.
Efficacy of rizatriptan in placebo-controlled studies
The endpoints that will be considered in the analysis of clinical trials presented here are: headache response, i.e. moderate or severe pain becoming nil or mild pain and pain free, severe or moderate pain completely disappearing, in both cases 2 h after giving the medication.
In these studies, rizatriptan was administered using conventional tablets or a wafer formulation. The wafer was developed as an oral alternative to the tablet. It dissolves within seconds when placed on the tongue, maybe swallowed without liquids and is absorbed from the gastrointestinal tract. The results obtained with the rizatriptan tablets were reported by Teall and colleagues (5) and those of the wafer by Ahrens and colleagues (6).
In the tablet study, both 5 and 10 mg rizatriptan were superior to placebo in terms of headache response at 1 and 2 h and, at 2 h, the 10 mg dose was significantly better than the 5 mg dose, producing headache relief in 71% (n = 455) of patients. Similar results were obtained when the wafer was used (Fig. 1). When the pain free endpoint, which is becoming the preferred endpoint in the evaluation of the efficacy of antimigraine therapy, was considered for both studies, the percentage of patients who were pain free 2 h after treatment with rizatriptan 10 mg was lower (tablet study: 42%, n = 455 and wafer study: 42%, n = 186).

Comparison between rizatriptan and other triptans
Due to the availability of many compounds of the triptan class in the market, it becomes important to gather evidence from trials in which they are compared head-to-head in order to provide the basis for making clinically sensible decisions. The arguments for head-to-head over meta-analytic comparisons have been made elsewhere (7), but briefly centre around ensuring homogeneous populations for comparison and the problems of combining data from results not all clearly on the same measurement scale. For these reasons it is important to compare the effects of rizatriptan to those of other triptans, and particularly with sumatriptan which is the clinical gold standard. Both compounds have different pharmacokinetic characteristics: rizatriptan reaches the maximal plasma concentration faster than sumatriptan, 1.0 (8) vs. 2.5 h (9), and has a better bioavailability, 40 vs. 14% (8, 9). Whether these properties of rizatriptan could translate into a faster onset of action and a better therapeutic consistency was a key question in the development programme.
Methodological considerations: ‘time to’ analysis
One way to study the results of clinical trials in headache is the ‘time to’ analysis which is an application of survival methodologies. Application of such methods represents a step in the sensible direction in which the endpoints in antimigraine therapy trials should be evolving to include more data from early time points, although clearly further steps are needed. With the methodology currently used, the appearance of a positive response to treatment after 30 min does not mean more than if it appears at 1 h when, for example, the endpoint is the response at 2 h. However, for the patient, a response at 30 min is very important because the migraineur wants the headache to disappear as soon as possible. Patients do not discard early endpoints, particularly those prior to 2 h, and nor should clinicians.
The availability of extra data points gives some small increment in power to the analysis and allows their inclusion with one test for the primary outcome, avoiding the problems of multiple t-tests. Moreover, it makes it possible to incorporate data from earlier time points when there are none from later ones, thus accommodating censoring. The technical and mathematical aspects of this methodology specific to headache have been analysed recently (10). This approach is not new, having been applied particularly in oncology from where the term survival arises (11).
Thus, the ‘time to headache relief analysis’ uses a survival method to ask questions about the proportion of patients who reach a particular endpoint at a particular time, for example, the endpoint of headache response or headache free. This can be done for continuous, stopwatch data, as well as for noncontinuous information, such as in the studies to be discussed for 30, 60, 90 and 120 min. It relies on the use of a discrete regression model that is a variation of the Cox model (11) and asks a very simple question: how long does the headache survive after treatment? In other words, how long does the patient have to put up with the headache?
Rizatriptan and sumatriptan study
Time to event analysis has been applied to the data for headache response obtained in a direct comparison between rizatriptan 10 mg vs. sumatriptan 100 mg (12). When expressed conventionally using the fixed time point of 2 h, the results of the comparison between rizatriptan 10 mg (67%, n = 385) and sumatriptan 100 mg (62%, n = 387) indicate that both compounds were more effective in relieving pain than placebo (40%, n = 159) and that, at 2 h, the effect of rizatriptan 10 mg was equal to that of sumatriptan 100 mg.
However, using the same data, the calculated hazard ratio captures the cumulative benefit over 2 h of one drug over the other (Fig. 2). In this case, a hazard ratio of 1.21 (95% CI = 1.02–1.44, P<0.032) indicates that there is a 21% greater likelihood that, at any point in the period of 2 h, the headache will go away sooner with rizatriptan than with sumatriptan. In this particular study, the hazard ratio was adjusted for an age imbalance because the sumatriptan group included older patients who tend to do better on the medication in that study. In the same way, it is possible to analyse ‘time to pain free’ outcome, and in this case the hazard ratio of 1.29 (95% CI = 1.02–1.63) indicates that, in the period of 2 h, there is a 29% possibility of doing better with rizatriptan. The comparable 2 h pain free outcomes were 9% (n = 159) for placebo, 40% (n = 385) for rizatriptan 10 mg and 33% (n = 387) for sumatriptan 100 mg.

Time-to-headache relief in patients receiving rizatriptan 10 mg or sumatriptan 100 mg (12). The hazard ratio was 1.21 (95% CI: 1.02–1.44, P < 0.032) after adjustment for age imbalance in the populations.
Apart from relieving the pain, it is important for the drug to reduce the functional disability of the patient. In the same comparative study it was found that both active compounds were significantly better (P<0.01) than placebo in returning patients to normality within 2 h. At this particular endpoint, rizatriptan 10 mg did significantly better (42%, n = 385, P = 0.015) than sumatriptan 100 mg (33%, n = 387). All groups had a comparable incidence of functional disability at baseline (12).
The elimination of nausea may be related to the effects of the triptans on the CNS (13). In a post hoc analysis of this particular study, looking at the effects of placebo, sumatriptan and rizatriptan in the group of patients that had nausea, at 2 h rizatriptan 10 mg produced a significantly greater reduction of nausea, starting at 30 min, (66%, n = 385), in comparison with placebo (38%, n = 159) and sumatriptan (58% n = 287), a peculiar difference that deserves further consideration (P<0.05). This study set out to compare the recommended dose of rizatriptan (10 mg) with that of naratriptan (2.5 mg) using the survival analysis methods described above, in terms of headache relief and time to headache relief within 2 h after drug administration, pain free and time to pain free (14). The return to normal function within 2 h and the effect on associated symptoms were also analysed. This was a randomized, double-blind, placebo-controlled out-patient study. The compounds were used for treating a single migraine attack in patients whose ages ranged between 18 and 65 years and who were 84% female.
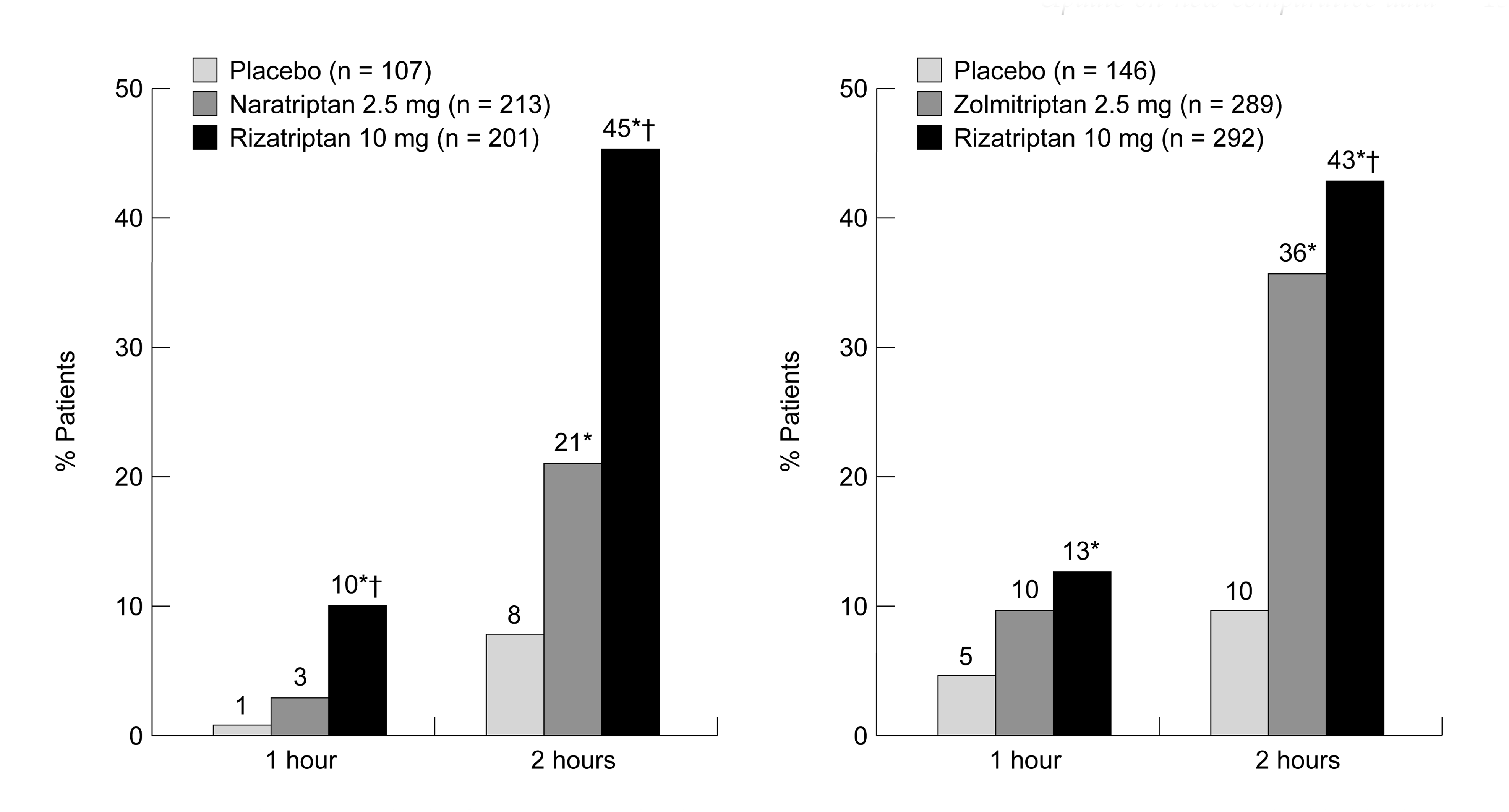
A significantly greater proportion of the patients was pain free both at 1 h with rizatriptan than with naratriptan or placebo. At 2 h, 8% (n = 107) of patients were pain free with placebo, 21% (n = 213) with naratriptan and 45% (n = 201) with rizatriptan, the differences between naratriptan and placebo, and between rizatriptan and naratriptan being statistically significant (P<0.05) (Fig. 3). This is not a particularly surprising result from what is previously known about these compounds (15), and constitutes a reassurance that it is possible to predict the results on the basis of the pharmacokinetic properties, such as the delayed time to reach maximal plasma concentration (T max) of naratriptan (16), of a compound before it reaches the clinic.
In the rizatriptan/naratriptan comparison, the time to headache response analysis showed a hazard ratio of 1.62 (95% CI = 1.26–2.09, P < 0.001) indicating that 62% of patients on rizatriptan were likely to do better than those receiving naratriptan during the first 2 h. On the other hand, the time to pain free analysis gave a remarkable hazard ratio of 2.68 (95% CI = 1.87–3.82, P < 0.001) in favour of rizatriptan.
Rizatriptan and zolmitriptan study
This study compared the recommended dose of rizatriptan (10 mg) with zolmitriptan (2.5 mg) in similar terms to those described above for the naratriptan comparator study. The other characteristics of the trial were similar to those of the naratriptan study with the exception that, in this case, the age of the study population was between 17 and 66 years (17).
In the zolmitriptan study, the response to rizatriptan was significantly better than that produced by placebo at 1 h. At 2 h, the pain free response was significantly better (P < 0.001) for zolmitriptan (36%, n = 289) and for rizatriptan (43%, n = 292) than for placebo (10%, n = 146). Rizatriptan was superior to zolmitriptan (P < 0.05) on the pain free endpoint at 2 h.
In the case of the rizatriptan/zolmitriptan comparison, the time to pain free analysis gives a hazard ratio of 1.31 (95% CI = 1.01–1.71, P<0.05) favouring rizatriptan over zolmitriptan. This indicates that in the 2-h period the patients who took rizatriptan were 31% more likely to have a better response. This result was adjusted in the analysis by removing patients whose freedom from pain was not sustained (rizatriptan n = 2, zolmitriptan n = 6) because it is an assumption of the model that relief is sustained up to 2 h (10).
Effects on functional disability for rizatriptan, naratriptan and zolmitriptan
When the effects of placebo, rizatriptan, naratriptan and zolmitriptan on functional disability at 2 h were compared, rizatriptan was found to eliminate functional disability significantly more than placebo, naratriptan and zolmitriptan. Zolmitriptan, but not naratriptan, eliminated functional disability significantly more than placebo (Fig. 4).

Consistency of the antimigraine effect of rizatriptan in the treatment of multiple attacks
A double-blind, placebo-controlled multiple attack study was carried out to examine the efficacy of rizatriptan 10 mg in the treatment of multiple attacks. Patients were randomized to one of five sequence groups in which each patient was instructed to treat four consecutive migraine attacks (18). In four of the groups, patients received rizatriptan 10 mg for three of the four attacks and placebo for the remaining attack in a sequential order, while in the fifth group, patients received the active compound for all four attacks. Ideally the results of this type of study allow the physician to explain to the patient what the chances are of obtaining a consistent response when treating several migraine attacks.
The results of this study indicate that 96% of the 252 patients receiving rizatriptan 10 mg experienced headache pain relief after 2 h in one out of three attacks (n = 243), 86% (n = 216) responded in two out of three attacks and 60% (n = 150) responded in three out of three attacks (Fig. 5). Seventy percent of the patients who did not respond to rizatriptan in the first attack, did so during the second attack, indicating that non-response during the first episode did not predict the lack of response during a subsequent attack. This constitutes the best published consistency data achieved so far, and it is interesting to speculate about the relationship of these results in the context of the good bioavailability data.
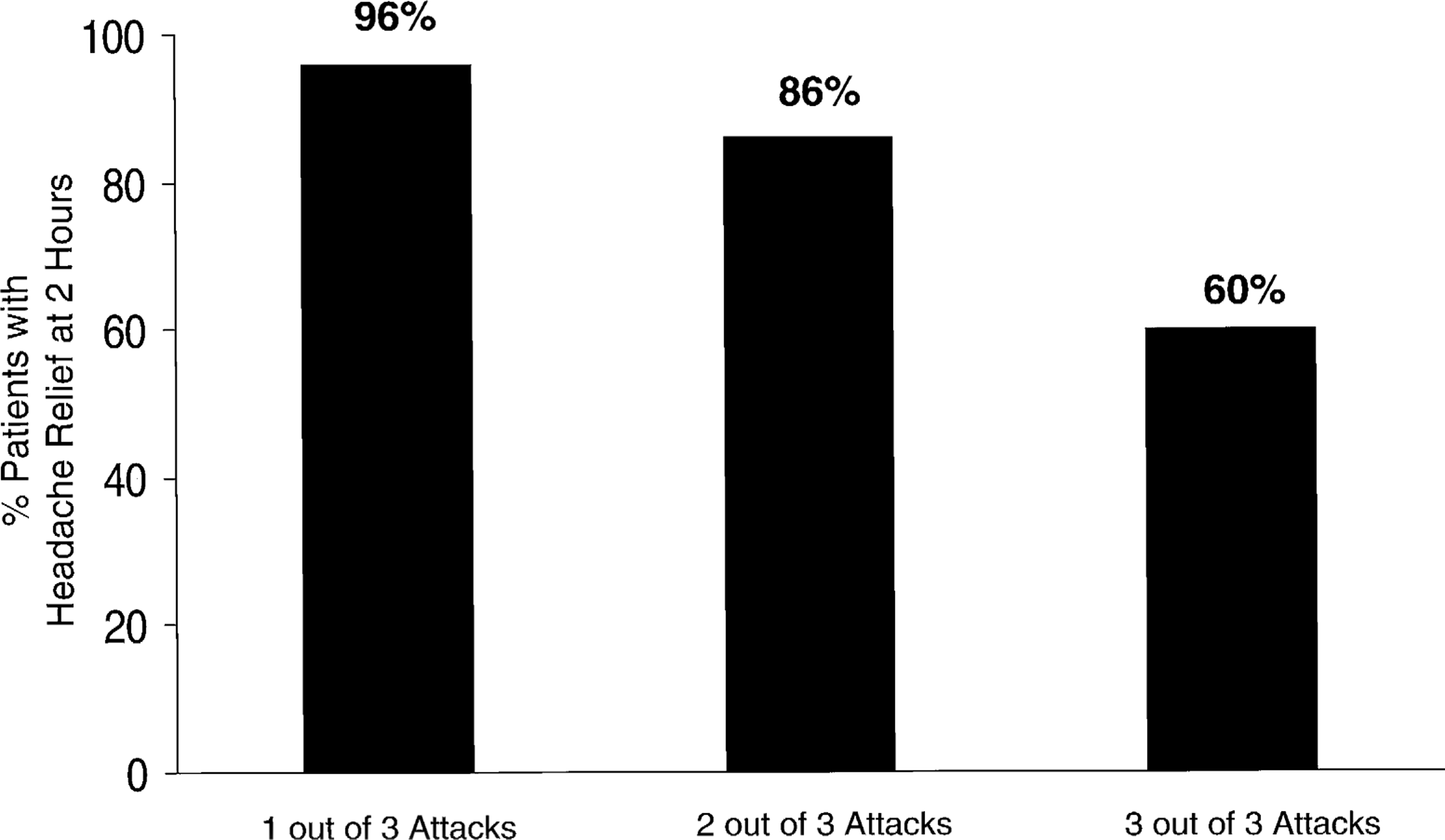
Consistency of the response obtained treating multiple migraine attacks with rizatriptan 10 mg (18).
Headache recurrence
This constitutes an important issue from the point of view of patients. In this particular group of studies, recurrence was defined as a response in patients within 2 h of the initial dose, going from severe to moderate pain to mild or no pain, and then return between 2 and 24 h to moderate or severe pain. Although the definition of recurrence is arguable, this is the characterization used in these studies, and highlights the value of direct head-to-head comparisons.
In the investigation in which the actions of placebo, sumatriptan 100 mg and rizatriptan 10 mg were compared (12), the incidence of recurrence was also analysed. Considering group sizes, this was similar for placebo (20%, n = 160), sumatriptan (32%, n = 307) and rizatriptan (35%, n = 388), about a third of patients in all groups had a headache recurrence. There was a somewhat longer time to recurrence in patients who received the active drugs rizatriptan (12.4 h) and sumatriptan (12.3 h) than in those receiving placebo (10.1 h).
In the comparisons between rizatriptan with naratriptan and placebo, the characteristics of headache recurrence were also analysed. Thirty-one percent (n = 201) of patients receiving rizatriptan and 21% (n = 213) receiving naratriptan experienced a recurrence. The mean time to recurrence was about the same for the active compounds, 12.6 for rizatriptan and 12.3 for naratriptan, in both cases longer than for placebo (6.9 h).
When rizatriptan was compared with zolmitriptan and placebo, similar results to those in the previous study were observed in terms of the incidence of recurrence: 28% for rizatriptan (n = 292), 29% for zolmitriptan (n = 289) and 26% (n = 146) for placebo. The corresponding values for the time to recurrence were 11.4, 11.9 and 9.7 h, respectively.
The rizatriptan placebo-controlled study (5) has shown that rizatriptan 10 mg is significantly more effective in the treatment of headache recurrence than placebo in the two endpoints: headache response and pain free. Up to 82% (n = 455) of patients experienced headache relief and 49% (n = 455) became pain free within 2 h after treating recurrence. This indicates that the headache is treatable when it recurs.
Rizatriptan in clinical practice
Rizatriptan is not affected by the concomitant use of oral contraceptives, selective serotonin re-uptake inhibitors (SSRIs) or β-adrenoceptor blockers, such as nadolol, metoprolol and atenolol. It is recommended that the dose of rizatriptan should be reduced to 5 mg in patients taking propranolol, due to interference with the processes responsible for drug metabolism in the liver, as well as in patients with mild to moderate renal, or hepatic impairment, or both. The safety of using the triptans during pregnancy has not yet been established and this constitutes a complex issue that should be determined for each patient and a routine rule cannot be established.
Conclusions
Rizatriptan produces consistent and high response rates in the acute treatment of migraine attacks. In a significant percentage of patients the pain disappears rapidly after administration of the compound. In the direct comparisons with sumatriptan 100 mg, naratriptan 2.5 mg and zolmitriptan 2.5 mg, rizatriptan 10 mg was superior on the pain free outcome at 2 h, on the time to pain free outcome within 2 h. Rizatriptan eliminated disability in a substantial percentage of patients at 2 h. The results of direct comparative studies allow evidence-based decisions to be made when selecting appropriate acute antimigraine treatments and, when applied, can translate into optimal outcomes for patients.
Footnotes
∗
Based on a presentation to the Symposium held during the IX Meeting of the International Headache Society, Barcelona, Spain, 24 June 1999.