
Abstract
Recent studies have suggested an association between Helicobacter pylori infection and migraine. However, various strains of the bacterium are present, some endowed with greater pathogenicity. In particular, H. pylori type I CagA-positive strains induce a higher release of proinflammatory substances by the gastric mucosa that could trigger systemic vasospasms. The aim of the present study was to assess the prevalence of H. pylori CagA-positive strains in subjects with migraine. One hundred and seventy-five patients affected by migraine (49 with aura, 126 without aura) were consecutively enrolled and matched for sex, age, social background and geographical origin with 152 controls. Helicobacter pylori infection was assessed through 13C-urea breath test. Specific serological IgG against CagA were detected through ELISA. The prevalence of H. pylori infection was similar in migraine patients and in controls (40% vs. 39%, respectively). Among migraine patients, prevalence of infection was not related to presence or absence of aura (45% vs. 37%, respectively). However, among infected subjects, a significantly higher prevalence of CagA-positive strains was observed in patients affected by migraine with aura when compared with those affected by migraine without aura (41% vs. 19%, P < 0.01) and with controls (41% vs. 17%, P < 0.01). CagA-positive H. pylori strains were found to be strongly associated with migraine with aura. A higher inflammatory response of the gastric mucosa to more virulent strains could release substances that may act as triggers of vasospasm in peculiar cerebral arterial districts, probably implicated in the ‘aura’ phenomenon.
Keywords
Introduction
Migraine is a common functional neurovascular disorder, characterized by attacks of severe headache and autonomic and neurological symptoms (1). The two main types of migraine are migraine with aura, occurring in about 75% of migraineurs, and migraine without aura, occurring in the remaining 25% of patients (1). Aura symptoms nearly always include visual, together with sensory or aphasic symptoms and, rarely, motor ones (1).
Helicobacter pylori infection, the most common chronic gastrointestinal infection worldwide, is the most important cause of chronic gastritis and peptic ulcer (2); its eradication, in fact, promotes healing of these and significantly reduces ulcer recurrence (3). Moreover, it is associated with an increased occurrence of MALT-lymphoma and gastric cancer (4, 5). Great variation exists in the prevalence of H. pylori infection between different countries and age groups. Once established, the infection can last for decades and spontaneous eradication is rare. Recently H. pylori infection has also been associated with some extra-intestinal pathologies. Among others, H. pylori infection has been shown to play a role in vascular organic disorders, such as ischaemic heart disease and stroke, and in vascular functional disturbances, such as primary Raynaud's phenomenon and migraine (6–10). Recently however, the presence of different strains of H. pylori has been decribed. In particular, a genetic polymorphism of H. pylori has been shown: the strains carrying the Cytotoxin Associated gene A (CagA), type I, appearing to be more virulent. CagA-positive strains, in fact, directly induce an enhanced inflammatory response locally at the site of infection, whereas CagA-negative strains are associated with a significantly lower flogistic infiltrate in the gastric mucosa (11, 12). A persistent and strong inflammatory response related to H. pylori infection may, eventually, influence vascular disorders through an immune-mediated release of substances, which could lead to vasospasm in extra-intestinal areas (13–16).
The aim of the present study was to assess the prevalence of H. pylori type I cytotoxic strains in subjects with migraine with respect to an age- and sex-matched group of controls.
Methods
We studied 175 patients (121 females and 44 males; mean age 40 ± 11 years) affected by migraine (49 with aura, 126 without aura), coming from a series of consecutive patients referred to the Headache Centre of the La Sapienza University. Informed consent was obtained from each patient before the study. Migraine was classified as with or without aura according to the criteria defined by the International Headache Society (IHS) (17). Six (12%) of the 49 patients affected by migraine with aura had experienced migraine without aura in the previous year, whilst 14 (11%) of the 126 patients affected by migraine without aura had attacks preceded by aura symptoms in the same period.
The control group consisted of 152 healthy subjects (102 females and 50 males; mean age 46 ± 14 years). Controls were occasional blood donors of the Gemelli Hospital. They were checked for migraine presence using same criteria as for cases (17). Still they did not show a familial history of migraine or other recurrent headaches. Moreover, controls were matched for sex and age, social background and geographical provenance with patients.
Helicobacter pylori infection was diagnosed by 13C-urea breath test, a non-invasive highly sensitive and specific method (18). Specific serological IgG against CagA were detected through ELISA (Radim, Pomezia, Italy) in infected subjects. Titres were defined as positive or negative according to a cut-off value of 10 U/ml (sensitivity and specificity > 95%).
In order to assess clinical level of migraine, self-evaluation test was used. Patients were asked to indicate in a daily diary intensity (with a score range from 0 to 4; 0 being the minimum, 4 being the maximum level), frequency (days of the month) and duration (hours) of attacks of migraine in the month preceding admission (7). Moreover, in patients and in controls, the prevalence of gastrointestinal (GI) symptoms (pyrosis, epigastric pain, halitosis, belching, bloating) was also evaluated using a validated dyspepsia score questionnaire (19).
Results are expressed as mean ±
Results
Helicobacter pylori infection
Prevalence of H. pylori infection was similar in migraine patients (70/175, 40%) and in controls (59/152, 39%). Mean age was significantly higher in infected patients (41 ± 10 vs. 34 ± 11 years; P < 0.001). In all the groups studied, no significant difference was found between females and males regarding positivity to H. pylori.
Type of migraine was not significantly related to infection status. In particular, 47 (37%) out of 126 subjects affected by migraine without aura and 22 (45%) out of 49 subjects affected by migraine with aura were infected by H. pylori. In both groups, infected patients did not show a significant pattern of intensity, frequency or duration of migraine attacks per month (Table 1), nor in the prevalence of all the GI symptoms evaluated (data not shown), when compared with non-infected subjects.
Intensity (score range from 0 to 4; 0 being the minimum, 4 being the maximum), duration (hours) and frequency (days of the month) of attacks of migraine in patients infected (HP pos) and not infected (HP neg) by Helicobacter pylori
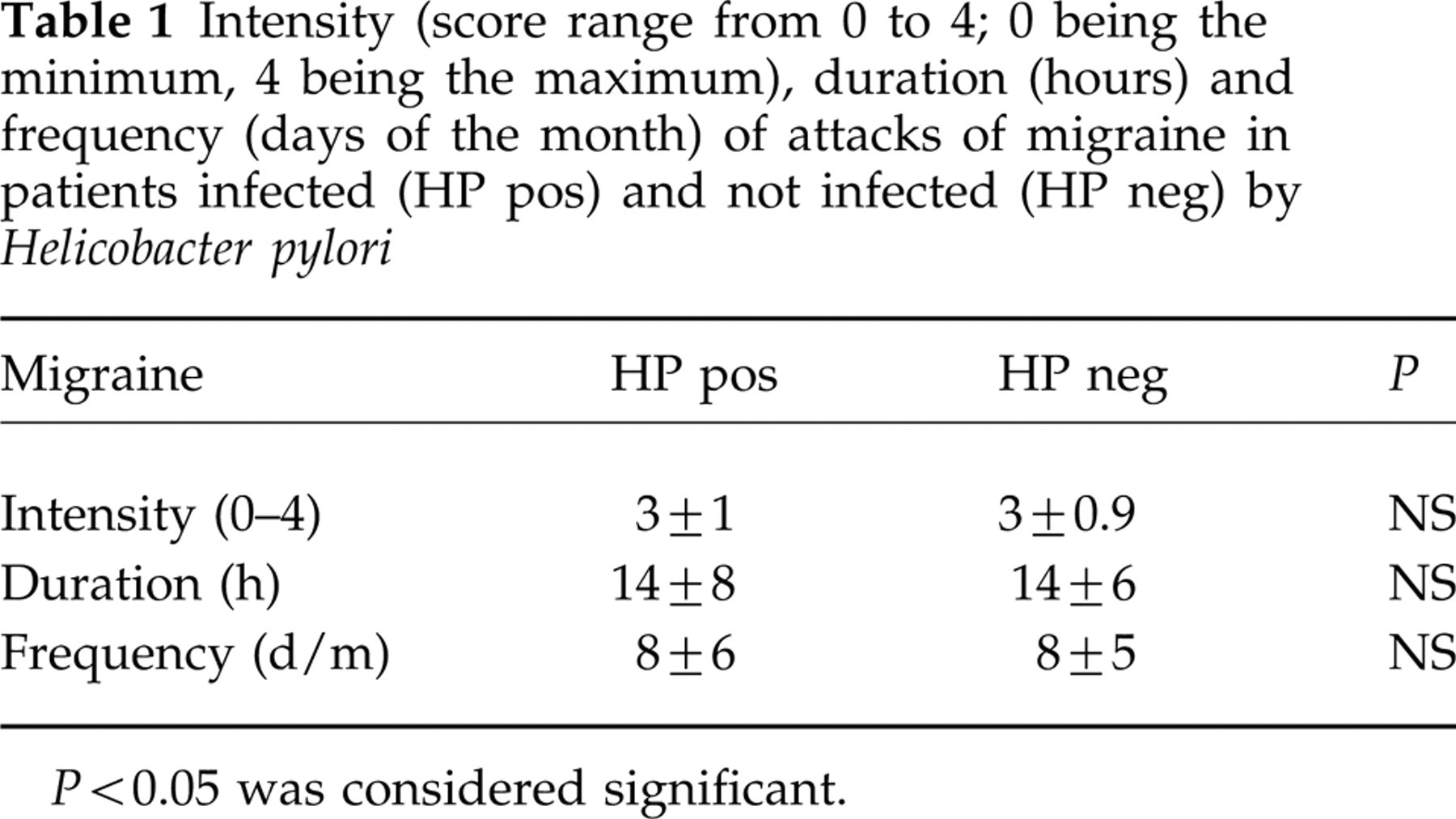
P < 0.05 was considered significant.
Prevalence of CagA-positive H. pylori strains
The prevalence of CagA-positive strains was slightly but not significantly greater in migraine patients. In particular, 44 out of 175 migraine patients and 26 out of 152 controls were bearing CagA-positive H. pylori strains (25% vs. 17%). In both groups, CagA-positive and -negative patients were similar in age, sex, social class and geographical origin. However, a significantly higher prevalence of CagA-positive strains was observed in patients affected by migraine with aura (20/49, 41%) when compared both with those affected by migraine without aura (24/126, 19%) and with controls (26/152, 17%) (Fig. 1). Multiple comparison among groups resulted in significance (P = 0.001). No difference in prevalence of CagA-positive strains between patients affected by migraine without aura and controls was observed.

Schematic representation of prevalence of infection by CagA-positive Helicobacter pylori strains in patients affected by migraine with aura, migraine without aura and in controls. The left column of each group represents the absolute prevalence of CagA status, the right one the relative prevalence, i.e. the prevalence in the subset of H. pylori-positive subjects. P < 0.05 was considered significant (∗).
In summary, considering only infected patients, CagA-positive strains were present in 91% of migraineurs with aura, in 51% of migraineurs without aura and in 44% of controls with significance at multiple comparison (P = 0.03) (Fig. 1). Presence/absence of CagA-positive strains of H. pylori however, was not related to the clinical characteristics of migraine (Table 2) and to the prevalence of the GI symptoms (data not shown) evaluated.
Intensity (score range from 0 to 4; 0 being the minimum, 4 being the maximum), duration (hours) and frequency (days of the month) of attacks of migraine in patients infected by CagA-positive (Cag pos) and CagA-negative (CagA neg) strains of Helicobacter pylori.
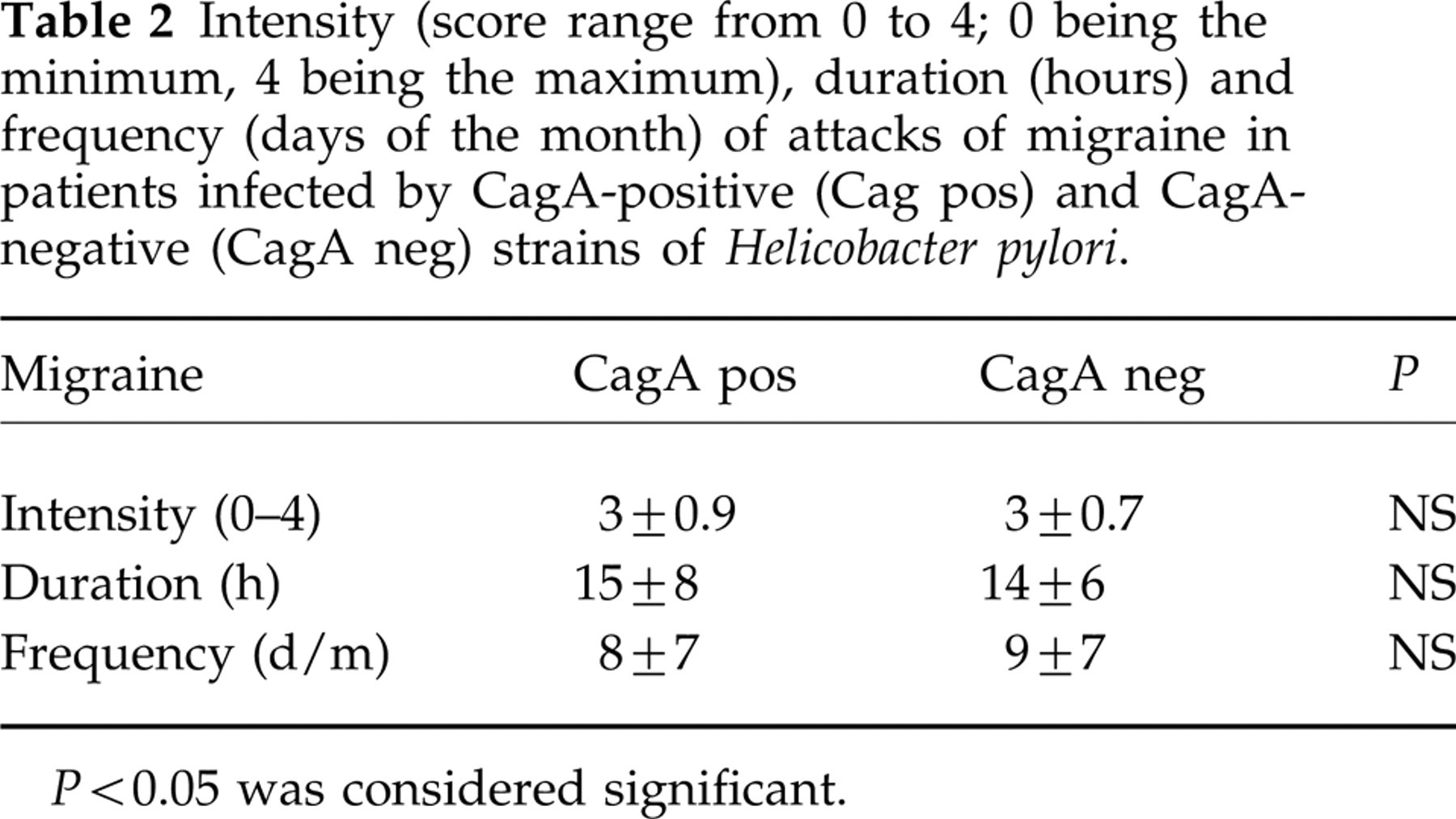
P < 0.05 was considered significant.
Discussion
The present study shows that infection by the highly virulent CagA-positive strains of H. pylori is significantly greater in patients with migraine with aura, suggesting a possible pathogenic role of these strains of the bacterium in the disease.
In order to explain the reasons for this association, it is important to consider what happens when H. pylori colonizes the gastric mucosa and the different outcomes of the infection by strains with and without the pathogenicity island Cag. In fact, the host inflammatory response to H. pylori is characterized by infiltration of neutrophils, monocytes, and lymphocytes into the gastric mucosa (20). Recruitment and activation of immune cells in the underlying mucosa involves bacterium chemotaxins, epithelial derived chemotactic peptides (chemokines) such as IL-8 and GRO-α, and proinflammatory cytokines released by mononuclear phagocytes (tumour necrosis factor-alpha, IL-1 and IL-8) as part of non-specific immunity. Antigen-specific cellular immunity results in a predominant Th1 lymphocyte response with an increase in interferon-gamma-secreting T-helper cells, whilst humoral responses lead to the production of anti-H. pylori antibodies and complement activation (21). Recent studies seem to confirm the growing importance of H. pylori genetic polymorphism as a major determinant of who develops disease. In particular, it is well known that possessing CagA positivity for H. pylori brings an enhanced virulence and a higher induction of production of cytokines, especially IL-8, and other substances endowed with proinflammatory and vasospastic properties (22). CagA, in fact, is a high molecular mass (120–128 kD) H. pylori antigen, which is part of the pathogenicity island, a complex gene cluster in which other postulated bacterial virulence factors, among them VacA and IceA, are located (11). Many studies have shown a clear association between CagA-positive H. pylori strains and severe forms of gastroduodenal diseases, including peptic ulcer and gastric cancer (11, 12). For these reasons, serological detection of infection with CagA-positive strains is considered, at present, the best practical test for virulence (23). If we take into account the multiplicity and large quantity of vasoactive substances produced, directly or indirectly, in response to chronic infection by CagA-positive cytotoxic strains of H. pylori, it is possible to speculate that these factors act not only at a local level but also on extradigestive areas. On this view, our group have recently found a higher prevalence of these more virulent H. pylori strains in patients affected by ischaemic heart disease (10). In particular, cytokines and other cellular acute-phase response mediators could act as promoters of the various mechanisms implicated in the genesis of the aura, including the spreading depression-like phenomenon (24–27). The relationship between a long-lasting infection and a chronic but recurrent disease, such as migraine, could be explained by considering that the high persistent inflammatory response to CagA-positive strains of the bacterium induces a hyperreactivity of cerebral vessels to various well-known trigger factors such as psychologic or physical stress, peculiar foods, female hormones and others, capable of determining the clinical manifestation of the disease.
Migraine with aura however, is not present in all subjects infected by CagA-positive H. pylori strains. Besides the presence of peculiar strains of the bacterium, in fact other factors may be implicated in the pathogenesis of the disease. In particular, considering the described linkages between peculiar HLA genotypes and the incidence of atrophic gastritis or coronary spasm, it is possible to speculate on the possibility that some individual factors, such as HLA type or other unknown factors, may make an individual more susceptible to the supposed vasospastic triggers induced by H. pylori (28, 29). However, migraine with aura has itself a specific genetic background. In fact, aggregations in families could be due to a combination of environmental and genetic factors, which is thought to alternate the response threshold to specific triggers of migraine (30). Helicobacter pylori infection per se was not associated with differences in GI complaints. Other large-scale trials have previously described how weak the association between infectious status, eradication and non-ulcer dyspepsia remains (31).
In conclusion, a role of the highly virulent CagA-positive strains of H. pylori could be hypothesized in the pathogenesis of migraine with aura. However, a double-blind cross-sectional eradication trial with a long-term follow up, which includes the evaluation of vasoactive molecules and HLA genotype, remains mandatory in order to clarify the rationale of the association.
Footnotes
Acknowledgements
We thank the association Ricerca in Medicina (Bologna, Italy) for the support given to perform this study.