
Abstract
The ovaries cyclically secrete estradiol and progesterone. Cyclic ovarian estradiol secretion is associated with a bone-saving and vascular protection effect. Endogenous progesterone does not modify the vasodilator effect of oestrogens. At physiological concentrations, the natural sex steroids have low antigonadotropic effects. More potent synthetic derivatives with more antigonadotropic effects were synthesized in the 1950s. After the menopause, there is no longer any need to use hormonal steroids as antigonadotropics. In addition, vascular contraindications are more common in an older population. Contraceptive steroids (particularly ethinyl estradiol) are therefore rarely used. The oestrogen that is most widely prescribed for post-menopausal replacement is a complex formulation of conjugated oestrogens of equine origin that is administered orally in a single daily dose. Improvements in hormone replacement therapy may result from the use of parenteral estradiol (providing sufficient doses are reached) and of a progestogen chemically more similar to progesterone.
Introduction
The risk/benefit ratios of the various natural and synthetic oestrogens and progestogens are still being debated. It is clear that their pharmacodynamics and clinical effects differ in several particulars.
The ovaries, from puberty to the menopause, cyclically secrete 17 β estradiol, a major oestrogen, and progesterone, a progestogen. Ovarian steroids reach the systemic circulation through the efferent ovarian veins. Plasma concentrations of these natural steroids are uniform, except in the ovarian veins, where they are 4- to 5-fold higher. In contrast, tissue concentrations vary and depend on the presence or absence of specific oestradiol and progesterone receptors (which characterize oestrogen-dependent tissues). The recent identification of novel oestradiol receptors (β receptors and nongenomic receptors) has extended the oestrogen-dependent tissues from the uterus and breast to the brain, bone, urinary tract, intestine and cardiovascular system (1, 2).
About 30% of healthy pre-menopausal women use oral contraceptives (OCs) for several years during their lifetime. OCs lower or suppress endogenous oestradiol and progesterone secretion. OCs consist of synthetic steroids with strong antigonadotropic activity: ethinyl-oestradiol in combination with various progestins, such as norethisterone, norgestrel, desogestrel, gestodene, norgestimate, and cyproterone acetate. About 60% of oral ethinyl-oestradiol is metabolized in the liver (first pass). High local hepatic levels provoke a pregnancy-like modification in oestrogen-dependent metabolism that is modulated by the type and dose of the associated progestin (3, 4).
Approximately 20% of healthy post-menopausal women use hormone replacement therapy. Since antigonadotropic steroids are no longer needed, therapeutic possibilities include other, less potent oestrogens (equine oestrogens, 17 β oestradiol) and progestogens, including progesterone. Oral oestrogen causes pharmacological effects on hepatic metabolism: HDL cholesterol rises, often associated with haemostatic disturbances (5, 6). Non-oral oestrogen administration mimics physiological ovarian secretion. Progestogen can modify oestrogen's effects on target tissues, including the breast, the uterine endometrium, and the cardiovascular system (7–9).
Around 80% of menopausal women either do not use hormone replacement therapy or do not use it long enough to obtain any measurable bone and vascular effect. The clinical and biological signs of oestrogen withdrawal vary from one individual to the next, partly because extra-ovarian oestrogen synthesis occurs in the brain, the adipose tissue, the bones and the arterial walls (10–12).
Endogenous hormones
From menarche to menopause, which coincides with the lowest incidence of pathological events in oestrogen-dependent tissues, the ovaries cyclically secrete oestradiol and progesterone.
The mean serum oestradiol (E) concentrations oscillate between 30 and 80 pg/ml during the first week of the menstrual cycle, between 80 and 300 during the second week, between 100 and 150 during the third week, and then drop to around 30 pg/ml again at the end of the fourth week of the menstrual cycle. The mean serum concentration throughout the 28-day cycle is between 80 and 100 pg/ml, both for 17 β oestradiol and its principal metabolite, oestrone. The oestrone level remains close to the oestradiol level by conversion, through the enzyme 17 β OH-dehydrogenase (Fig. 1). Rapid oscillations of ± 50% around these mean values occur daily (13).

After the menopause, plasma oestradiol levels are lower than 30 pg/ml (plasma oestrone levels are only slightly higher). Extra-ovarian oestrogen synthesis may occur in the adipose tissue, the brain, the bone and the arterial wall. Oestrogens are synthesized by aromatization of circulating androgens, which are often of adrenal origin. For some women, this aromatase activity may considerably attenuate the consequences of low serum oestradiol levels in these specific tissues (12).
A minimum serum oestradiol level of 60 pg/ml is necessary for maximum benefits, including vascular effects. In post-menopausal women, inter-individual variations of plus or minus 10 pg/ml around the mean do not measurably affect vascular risk (14). Before the menopause, low E concentrations of around 30 pg/ml during the first days of the ovarian cycle may coincide, in some women, not only with mood disturbances and migraines, but also with the cyclical re-occurrence of anginal attacks or heart rhythm disturbances. This may be due to a low E milieu that does not permit optimal vasoactive reactions (15, 16). Potential mechanisms for E's rapid vasodilator effect include a calcium antagonist effect on vascular smooth muscle cells and stimulation of endothelial nitric oxide synthesis (17, 18). Primate and human data suggest that optimal effects on vasomotility and atherosclerosis prevention require E levels of ≥ 60 pg/ml.
This physiological E level has little effect on serum lipids. HDL cholesterol decreases slowly and modestly after menopause, while triglycerides rise. LDL cholesterol increases after menopause, but the mean LDL particle size is larger (and more favourable) in women than in men in the same age group (19, 20). High triglyceride levels associated with small LDL particle size positively correlates with an increased coronary risk (21), specifically in post-menopausal women (22).
Physiological levels of oestradiol have a beneficial effect on haemostatic balance by reducing fibrinogen, factor VII and PAI1 in comparison with what would be expected with post-menopausal levels (23).
The very high E levels that occur during the second and third trimesters of pregnancy (> 1500 pg/ml) trigger metabolic changes in the liver: SHBG and angiotensinogen rise, associated with a rapid parallel increase in triglycerides and HDL cholesterol, a decrease in LDL particle size, and an increase in Factor VII and resistance to protein C (24, 25). This short-lasting procoagulant effect may be beneficial in limiting postpartum haemorrhage.
Cyclic ovarian E secretion is associated with a bone-saving and vascular protection effect in women compared with men or post-menopausal women of the same age. This protective effect persists after adjustment for serum lipids, blood pressure, weight and social stress. In both women and female monkeys, the vascular protection is mainly due to the direct effect of sex hormones on the endothelium, smooth muscle functions, and collagen disposal in arterial wall (9, 26–28).
Mean serum progesterone levels are below 1 ng/ml during the follicular phase, rapidly increasing after ovulation to around 20 ng/ml and dropping during the last few days of the cycle preceding menstruation. After menopause, plasma progesterone is always less than 1 ng/ml. Extraovarian synthesis of progesterone does not occur. Progesterone controls oestradiol-induced endometrial growth (7); it also probably benefits the breast tissue (8) and the brain (29). Progesterone is metabolized to 5α pregnanolone, a physiological anxiolytic that modulates GABA receptors (30).
Endogenous progesterone does not modify the vasodilator effect of oestrogens (15). In castrated primates, replacement progesterone does not attenuate oestradiol's vasodilator effect on the coronary arteries (9). Progesterone alone induces endothelium-independent coronary artery relaxation (31). Endogenous or exogenous progesterone does not reduce the beneficial effect of oestrogens on LDL-cholesterol metabolism or arterial wall smooth muscle proliferation (9, 31, 32).
Oral contraceptives
At physiological concentrations, the natural sex steroids have low antigonadotropic effects. More potent synthetic derivatives with more antigonadotropic effects were synthesized in the 1950s.
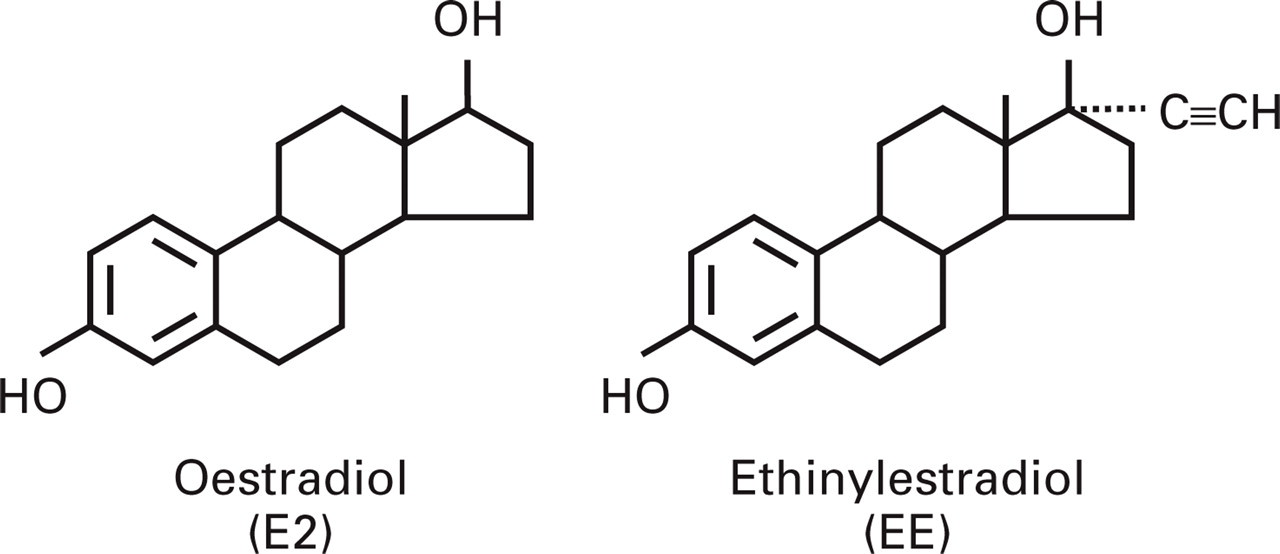
Ethinyl oestradiol (EE) (Fig. 2) has an ethinyl radical on carbon 17. This inhibits 17 β hydroxylation, which initiates oestradiol metabolism in the intestinal wall, the hepatocyte, and most target tissues. Because of its potency and strong antigonadotropic effect with a single daily oral dose, it is the most popular oestrogen used in oral contraception.
Progestins are mainly synthesized from 19-nortestosterone; their effects on the endometrium are similar to progesterone's. They are also strongly antigonadotropic with a single daily dose. The first progestin used in OCs was norethisterone, followed by norgestrel, and, more recently, desogestrel, gestodene, and norgestimate (Fig. 3). Gestodene and norgestimate have less residual androgenic activity than norgestrel and desogestrel (33).

Combined pills inhibit the endogenous secretion of oestradiol and progesterone, which are replaced by ethinyl oestradiol and progestin.
There are large intra-individual differences in EE and progestin plasma concentration, with means of around 100–1000 pg/ml for 50 μg EE and 1–5 ng/ml for the usual dose of the various progestins.
Because of the low clearance rate and the first pass hepatic effect, liver cells metabolize around 60% of the EE dose (34), resulting in oestrogen stimulation comparable to that observed during pregnancy. This stimulation modifies lipids and coagulation factors: triglycerides and HDL cholesterol, Factor VII and resistance to activated protein C increase and antithrombin decreases (35).
The addition of norethisterone or norgestrel, first and second generation progestins that have mild androgenic activity, attenuates the changes in liver metabolism induced by EE; HDL cholesterol and triglyceride levels tend to decrease in comparison with those of individuals who use EE alone, and even in low EE dose users in comparison with non-users. The ‘third generation’ progestins, such as desogestrel and gestodene, do not modify the EE-induced changes in liver metabolism. Thus, mean HDL cholesterol and triglyceride levels and procoagulant effects (specifically, acquired resistance to protein C) are higher in users of third generation OCs than in users of second generation OCs (3, 4, 36, 37).
The potential consequences of the procoagulant effect may be particularly worrisome in women who are older, who smoke, or are hyperlipidaemic, diabetic, obese, hypertensive, or have a past personal or family history of venous or arterial thromboembolic accidents. These woman should not use any formulation containing oral EE (38, 39).
Even reduced EE doses in a young, selected and controlled population of women still have an increased risk of thrombo-embolic accident, in particular phlebitis and ischaemic stroke, in comparison with past users (40) or never-users (41–43).
In addition to smoking, hypercholesterolemia and diabetes, the most worrisome pre-existing factors are obesity, arterial hypertension (in particular during pregnancy), and inherited coagulation inhibitor deficiencies. The vascular risk returns to normal when OCs are discontinued; thus the rare arterial accidents are not primarily associated with atherosclerosis but are thromboembolic in nature (44).
Progestin only pills
Since progestins, which are capable of decreasing endogenous oestradiol production, appear to be free of increased thromboembolic risk, they are sometimes used alone for women who are at vascular risk (43). Experimental studies suggest that atherogenesis can be enhanced by progestogen in a hypoestrogenic animal. Progestins also may alter endothelium function and reduce the oestrogen physiological vasodilating effects on the brain, the muscle vasculature, and the coronary arteries and should be used with caution (9). The risk for aneurysmal bleeding and haemorrhagic stroke seems increased in users of norgestrel (40). Progestin-only oral contraceptives are also associated with an increased risk of diabetes (45).
Suppressing ovarian oestradiol secretion may induce early menopause-like consequences such as osteoporosis (46), reduced quality of life, impaired vaginal secretions, dyspareunia, and increased risk of sexually transmitted diseases (47, 48).
Hormone replacement
After the menopause, there is no longer any need to use hormonal steroids as antigonadotropics. In addition, vascular contraindications are more common in an older population. Contraceptive steroids (particularly ethinyl oestradiol) are therefore rarely used. The oestrogen that is most widely prescribed for post-menopausal replacement is a complex formulation of conjugated oestrogens of equine origin (CEE) that is administered orally in a single daily dose.
Conjugated equine oestrogens
CEE consists of a number of oestrogenic substances (oestrone, oestrone sulphate, equiline, equilenine, 17α-dihydroequilenine, 17α-oestradiol) whose relative activities have not been clearly delineated. Precise pharmacokinetic studies of the oral formulation have been difficult. Within hours following the absorption of 0.625 mg of CEE, an oestradiol peak at a mean of 40–60 pg/ml is observed; the oestrone peak is three- to four-fold greater (49). Some equine derivatives have a half-life of several days. As demonstrated in experimental models, they have antiatherogenic and vasodilator effects identical to those of oestradiol (9). The vasodilator effect has been confirmed in human studies (50).
A favourable effect on fibrinolytic activity (decrease in PAI1) has also been observed (51), suggesting that oestradiol's beneficial effects on the arterial wall can be obtained with this type of oestrogen therapy. However, the first pass hepatic effect is accompanied by pregnancy-like stimulation of oestrogen-dependent hepatic metabolism. HDL cholesterol increased around 15% within the first months of use, and then decreased to around 5% at the end of 3 years (52). The mean 15% increase in triglycerides is maintained over time, but it may be much higher in patients with vascular risk, in whom it constitutes an aggravating factor (53).
This effect, coupled with a parallel drop in LDL cholesterol and in LDL particle size (19), may have an adverse coronary risk in older women (21, 22).
Women who currently use CEE at a dose of 0.625 mg/day have a significant increase in coagulation factors, such as factor VII, fibrino-peptide A, and prothrombin fragment 1 + 2, and a significant drop in anticoagulant factors, such as antithrombin III and protein S (51, 54).
CEE was initially used short-term (generally less than 3 years), often in relatively young, hysterectomized or oophorectomized women. The first surveys published in the 1970s showed an increase in the frequency of vascular accidents, particularly myocardial infarction and stroke, in CEE users (55, 56). Since then, studies have suggested that the dosing was an essential problem: doses of CEE two-fold lower than those used in the 1960s appeared to produce strong vascular protection (57). However, as with the oral contraceptives, healthy users were carefully selected (6), but this selection process did not avoid the increase in thromboembolic deep venous, pulmonary and cerebral accidents that continues (58–62). The first prospective, randomized, placebo-controlled study using a combination of CEE and a progestin has shown no protective effect in women who are at high vascular risk. Users not only had more venous thromboembolic accidents but also tended to have more myocardial infarcts, and death, during the first year of the study (5).
Oral oestradiol
Despite low bioavailability, oral oestradiol, in micronized or valerate form, produces therapeutic effects, specifically the re-establishment of physiological vasomotricity. However, because of the strong first pass hepatic effect, a dose of 1–2 mg (seven to 14 times more than the intramuscular dose) is required to reproduce the effects of endogenous production of around 100 μg of E. The low bioavailability arises from the rapid metabolism of oestradiol in the digestive tract into barely active or inactive metabolites. Twenty to 25% is metabolized by the intestinal wall and around 70% by the liver. The hepatic cells receive the impact of 75–80% of the active form of the steroid, whereas the peripheral target tissues share only 5–10% of bioavailable oestradiol (63). This produces changes in oestrogen-dependent hepatic metabolism similar to those that occur during pregnancy. The metabolic side-effects are very similar to those of CEE: an increase in oestrone/oestradiol ratio SHBG, angiotensinogen and triglycerides; a decrease in antithrombin; and an increase in fragment 1 + 2 of the prothrombin (19, 64).
Percutaneous oestradiol
Cutaneous oestradiols in gel form (daily application) or in patch form (once- or twice-weekly application) closely simulate the physiological ovarian model. They deliver 17β oestradiol into the vessels of the dermis, then into the general circulation. There is no first pass hepatic effect in oestradiol metabolism; the oestrone/oestradiol ratio and regulation of hepatic metabolism are more physiological. In particular, a slow increase in HDL cholesterol occurs without a parallel increase in triglycerides; a decrease in LDL cholesterol occurs without a decrease in LDL particle size; and a decrease in fibrinogen and PAI occurs without an increase in factor VII and a decrease in antithrombin III (19, 23, 64).
Subcutaneous oestradiol implants reproduce, in primates, all the antiatherogenic and vasodilator effects of endogenous oestradiol (9). The favourable effects on lipids, haemostasis and vasodilation are clearly dose-dependent and require an oestradiol plasma concentration greater than 60 pg/ml (15, 23, 65).
Individual adaptation of the dose is essential since the patch systems only deliver small quantities of oestradiol and there is great inter-individual variability in oestrogen bioavailability by any route of administration (23, 66). Gel formulations are invisible, can be applied on large skin surfaces, and are better adapted to delivering doses that maintain serum oestradiol levels ≥ 60 pg/ml. No studies have been performed in a sufficient number of users of cutaneous oestradiol to assess the incidence of vascular accidents.
Associated progestogens
The progestogen most commonly used in North America to protect the endometrium of non-hysterectomized post-menopausal women is medroxy-progesterone acetate (MPA).
Most experimental and human studies of progestogens used for hormone replacement therapy show an effect of MPA that differs greatly from that of natural progesterone. Added to replacement doses of oral CEE or subcutaneous oestradiol, current MPA doses negate the antiatheroma and vasodilator benefits of oestrogens. At current doses, however, natural progesterone maintains all of oestrogen's benefits; the benefits are only negated at supraphysiological concentrations (9, 67).
Several human studies have come to similar conclusions (52, 68–70). The longest prospective controlled study (PEPI) shows a significant decrease in HDL cholesterol without the reduction in triglycerides and perturbation of the 2-h glucose test that is provoked in MPA users, whereas oral micronized progesterone users had no metabolic side-effects at doses ensuring identical results on the endometrium (52). Two other studies confirm that MPA reduces or negates the vasodilator effects of the associated oestrogen (68, 69); this is not observed with exogenous or endogenous progesterone (15, 70). The choice of the progestogen may therefore be as important as the choice of the oestrogen in the modulation of cardiovascular effects of various forms of hormone replacement therapy (9).
Conclusion
Different oestrogens at different doses administered by different routes do not have the same pharmacodynamic effects and do not have the same influence on the risks of arterial and venous thrombo-embolic accidents.
The most common prescriptions of oral conjugated equine oestrogens or ethinyl-oestradiol may not be the best choice for vascular prevention in individuals who are at risk and should be reserved for a selected healthy population.
Progestins have different effects depending on whether they are used with contraceptive doses of ethinyl-oestradiol or with replacement doses of varying oestrogens. Some progestins may negate all the expected vascular benefits from relatively weak oestrogens, but when given with relatively strong oestrogens they may be beneficial in reducing their thrombogenic effects. The most current progestin, medroxy-progesterone acetate (in hormone replacement) or ‘third generation’ progestogens (in contraception) are not perfect.
Improvements in hormone replacement therapy may result from the use of parenteral oestradiol (providing sufficient doses, probably closer to 80 rather than 40 pg/ml, are reached) and of a progestogen chemically more similar to progesterone than medroxy-progesterone acetate. All ongoing prospective controlled studies of HRT use a form of oestrogen therapy that creates pregnancy-like pharmacological effects. None are investigating hormone replacement that would re-establish the hormone physiology of pre-menopausal women.