
Abstract
Keywords
Bipolar disorder is a highly recurrent disorder with 70–75% of patients having at least one recurrence within four to five years of recovery from mania [1]. The social and economic costs to patients and society are significant with high rates of separation and divorce and a two to three-fold increase in the deterioration of relationships and careers [2]. Following manic episodes, almost onethird of patients cannot work for six months and only one-fifth return to work at their former skill level [3, 4].
Between 91 and 97% of patients with an affective psychosis (most with a diagnosis of bipolar disorder) have been found to reach ‘syndromal’ recovery (i.e. no longer meet DSM-IV episode criteria) after 12 and 24 months, respectively, of their first hospitalization, but only about one-third have reached full symptomatic or functional recovery [5]. Functional recovery by 6 and 24 months was 2.6–2.7 times less likely than syndromal recovery [5]. Such poor functional recovery largely explains the recent ranking of bipolar disorder as the sixth most disabling condition globally in the recent World Health Organization ‘Global burden of disease’ report [6].
Despite considerable advances in pharmacotherapy [7], about 40% of bipolar disorder patients relapse within one year, 60% in two years and 73% over five years [1], indicating the significant limitations of current interventions. Lithium prophylaxis protects only 25–50% of individuals with bipolar disorder against further episodes [8], although the poor treatment adherence rates (18–51%) reported among patients with bipolar disorder may contribute to these high relapse rates [9].
A high correlation has been found between poor medication adherence and low levels of acceptance of the diagnosis of bipolar disorder, suggesting that psychosocial interventions focusing on adaptability to illness may provide a useful means of reversing the trends to relapse [10]. Consequently, a number of psychosocial interventions for bipolar disorder in combination with pharmacotherapy have emerged, with most being reported only in the last decade.
Psychosocial treatments for bipolar disorder
Many psychosocial treatments are psychoeducational (involving prodromal management) [11] and/or family and couples focused [12, 13]. Interpersonal and social rhythm therapy (IPSRT) addresses the impact of biological and social rhythms on life events [14]. Cognitive behaviour therapy has been adapted for the needs of bipolar disorder patients [15, 16] and has been evaluated in controlled trials [17–20]. The aims of cognitive therapy are to alleviate acute symptoms and prevent relapse and recurrence through monitoring and challenging unhelpful thoughts and assumptions. The clinical advantages include its short-term efficacy, coherent theoretical framework, structured rationale for interventions, and enhancement of the individual's sense of self-efficacy through skill development [21].
The psychological impact of bipolar disorder
Most individuals with bipolar disorder find the illness experience traumatic, and experience significant disruptions to their beliefs about themselves, their world, relationships and self-esteem–both during and after episodes [19]. The humiliation, self-exposure and loss of a healthy self-concept, especially with episodes of mania, inevitably have a significant effect on the individual's sense of security [21–23]. The repeated cycles of marked disturbances of behaviour, coupled with a greater likelihood of syndromal recovery and consequent awareness of the ramifications of such behaviour, differentiate this condition from other major psychotic conditions such as schizophrenia.
Risk factors
There are many overlapping risk factors that predispose individuals to bipolar disorder. Biological vulnerabilities to the condition include genetic [24, 25] and neurodevelopmental [26] factors. Temperament has been found to be one of the main factors accounting for polarity of episodes [27]. However, it is unclear whether individuals with bipolar disorder differ to controls on standard measures of introversion, extraversion or neuroticism. Some studies report no significant differences [9, 28] while other studies report higher scores on extraversion [29], neuroticism [30, 31] and hysterical traits [31]. Self and family reported neuroticism has been found to significantly correlate with poor outcome [32, 33]. Euthymic bipolar I disorder patients have been found to score lower on scores of objectivity, ego resilience, emotional stability and ego control compared to controls [31]. Interpersonal sensitivity appears to be more common in bipolar II disorder than in unipolar depression [34].
Cognitive vulnerability to unipolar and bipolar depression arises as a consequence of dysfunctional underlying beliefs which develop from early learning developmental experiences. Life events that have specific meaning for that individual activate these beliefs [21]. An understanding of these formative experiences and how they shape the individual's perceptions and core beliefs is critical when determining appropriate therapeutic interventions [35].
The time in life when disruptions in cognitive processing and development initially occurs has a significant bearing on the schemas activated during major life stresses later on. The Eriksonian model [36] is useful in determining the impact of various negative experiences on the development of early maladaptive schemas according to the individual's developmental stage. Each stage of child development involves the learning of skills through the mastery of challenges. The healthy resolution of life crises is critical at specific time points for adaptive schema to develop [35].
Stressful life events and cognitive vulnerabilities
The role of cognitive vulnerabilities and stressful life events precipitating unipolar depression have been well researched [37, 38]. The few published studies on bipolar disorder have suggested that negative coping styles combined with stressful life events can lead to episodes of mania and depression [39, 40]. Bipolar disorder patients with high levels of stress are 4.5 times more likely to have a mood disorder relapse than patients with low levels of life stress [41]. Symptom severity in bipolar disorder is significantly associated with sociotropy, interpersonal events and the interaction of the two [42].
A greater number of dysfunctional attitudes is endorsed by bipolar disorder patients compared to healthy controls even when euthymic [43]. In contrast with the control group, bipolar disorder patients had a more fragile and unstable self-esteem, higher levels of dysfunctional attitudes (particularly related to need for social approval and perfectionism), over-generalized memory and poorer problem-solving skills [40]. This suggests the ongoing presence of dysfunctional attitudes, in addition to mood congruent cognitive changes, are experienced by at least some bipolar disorder patients. It is, however, difficult to determine whether such cognitive dysfunctions are a cause or a consequence of bipolar disorder.
Cognitive adaptation to illness
The individual's cognitive adaptation to chronic illness (be it medical, surgical or psychological) concerns how meaning is assigned to the illness; assumptions of control over the illness and an evaluation of self in a new context [22, 44]. Questions of identity and self-concept are paramount to the adjustment process. Patients have been found to report a change in their sense of self after intense experiences of hypomania, mania or depression leading to vulnerabilities in self-esteem and a confused sense of self. Feelings of stigma, guilt and shame, anger and avoidance are common responses [22, 45].
Cognitive adaptation to the experience of mental illness has been remarkably under-researched in contrast to the wealth of literature published on the adjustment process associated with physical illnesses such as cancer. Three adaptive pathways have recently been identified in relation to the illness experience of cancer patients [46]. Some patients are described as acting against the illness through withdrawal or confrontation (reactance) with anger, blame, resentment, defiance and resistance commonly displayed. Other patients adapt to the sick role, accepting the privileges and protections as well as the limitations (acceptance). A third group experience a major reconstruction of their lives coming to terms with the elements of the illness, understanding the limitations but reconstructing their lives to give it a meaning which reaches well beyond their illness (reorientation). This illness adaptation model includes an analysis of the process of separation and transition: from the shock, confusion, disbelief and bewilderment of receiving a diagnosis (patientness), to the realization that others may never really understand, acknowledge or share their trauma (communicative alienation), to the constriction in space and time and loss of power and status felt as they surrender their usual social and working roles (boundedness).
An innovative cognitive model of dysfunctional illness behaviour has been proposed that examines how patients process information to construct an understanding of their illness [45]. A central role is given to the patient's beliefs about their illness; beliefs about the self, others and the world; and the interaction of these two sets of beliefs that gives the illness its own unique meaning. These components are described as the illness belief triad. Beliefs about the illness incorporate the causes, consequences and control aspects of the illness. Beliefs about self, others and the world incorporate the selfschema as well as their perceptions about competence, vulnerability and whether they deserve to be ill. The interaction between the illness and non-illness related beliefs incorporates the individual's unique meaning of illness, which in turn will determine the nature of social and psychological functioning.
Development of a new explanatory model and treatment for bipolar disorder
The traditional explanatory model of bipolar disorder highlights the role of genetic and biological risk factors interacting with stressful life events in triggering illness episodes. Our proposed model (Fig. 1) highlights not only biological factors but also temperament, personality and developmental experiences as key vulnerability factors. Cognitive and schematic vulnerabilities are seen to act as filters in triggering mood shifts when stressful life events occur. Personality factors such as dependency and self-criticism [47], interpersonal sensitivity [34], need for approval and perfectionism [24] have been found to be more prevalent in individuals with bipolar disorder than unipolar depression. Furthermore, early developmental experiences are considered to impact on the bipolar disorder patient's cognitive vulnerabilities and underlying core beliefs, thereby impairing their capacity to function [23, 48, 49]. On the basis of these findings, it is hypothesized that a significant group of patients with bipolar disorder (particularly those with poor psychosocial functioning) would benefit from addressing their cognitive vulnerabilities and underlying core beliefs in order to reach full symptomatic and functional recovery.
Proposed explanatory model of bipolar disorder. Oval shapes represent filters and the dotted line highlights the traditional model.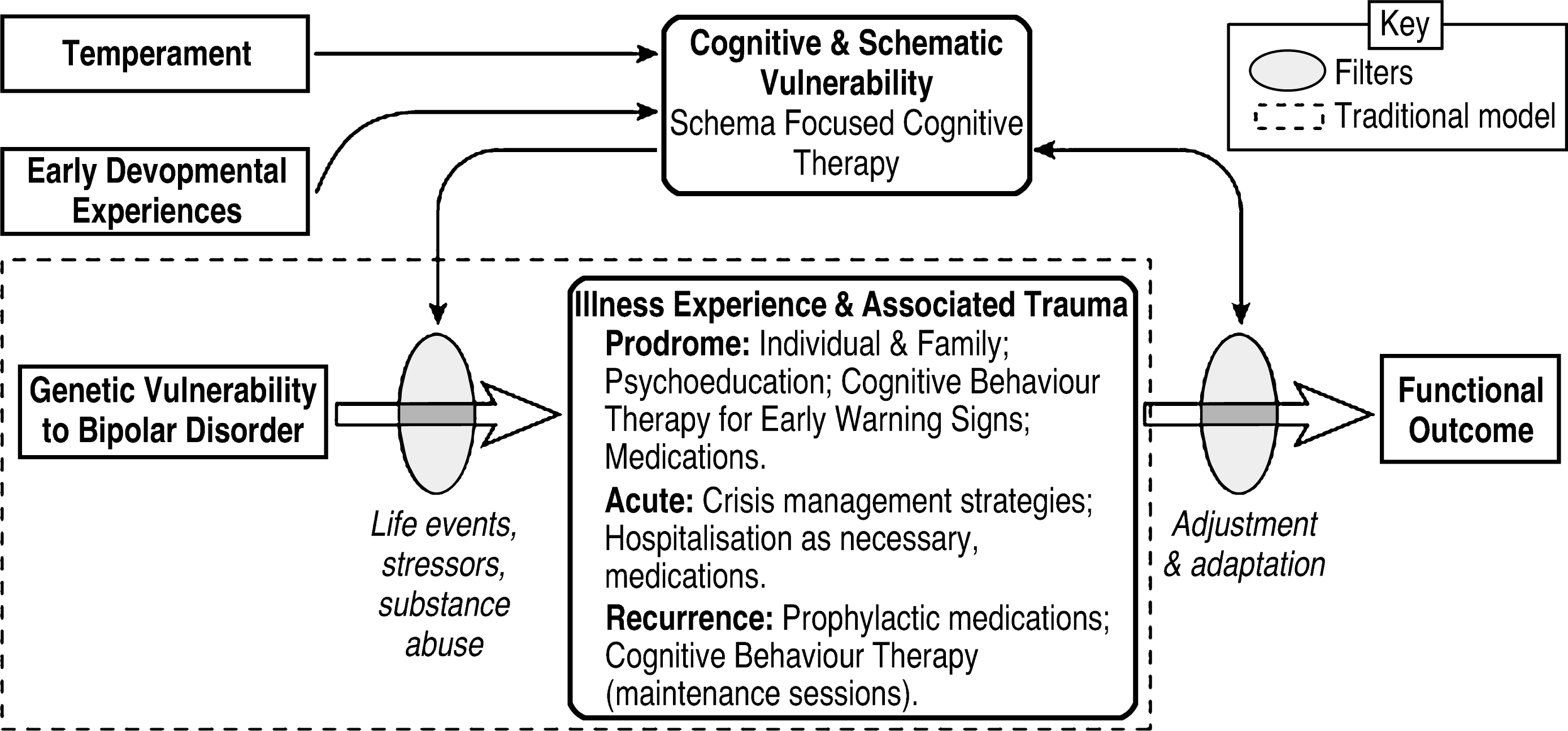
Given the embryonic stage of our model, it remains difficult to determine the degree to which underlying core beliefs have arisen from personality/developmental experiences, or the illness, or an interaction between each of these factors. The effects of personality and illness are most probably circular. Not only do personality factors heighten an individual's vulnerability to bipolar disorder [34, 40, 47], but persistent mood instability itself produces phenomenology consistent with the personality constructs considered to be predisposing (e.g. dependency) [48]. Irrespective of the point of evolution of the schemas, if they are maladaptive then they need to be modified, preferably in the early stages of illness.
As yet we do not have sufficient evidence to determine the nature or degree to which core beliefs impact on recovery. We can only surmise from the current literature on personality disorder that maladaptive core beliefs impair the individual's capacity to adapt and function well in interpersonal and vocational domains [23, 50, 51]. It is highly probable that the trauma of the bipolar illness and subsequent losses would activate or heighten selfdefeating constructs in vulnerable individuals. However, it is unclear how the experience of any debilitating illness, such as bipolar disorder, effects those individuals with relatively strong and adaptive core beliefs. Some may have sufficient resilience and social resources to retain a healthy view of themselves and the world, while others may be more negatively effected. Further research is needed to determine why some individuals adapt to chronic illness better than others.
The authors propose that schema-focused cognitive therapy modified for the specific needs of patients with bipolar disorder offers a viable alternative to currently available psychosocial interventions for those who remain dysthymic or functionally impaired post-episodically. The treatment we propose incorporates psychoeducation, cognitive behaviour therapy and IPSRT strategies in the initial phases of therapy and then transcends this through its focus on core beliefs and the psychological adjustment process at a schematic level. Therapy aims to reduce vulnerability to relapse and recurrence through symptom management, and to improve psychosocial functioning through modification of the bipolar disorder patient's cognitive styles and deeper schematic structures. As noted in the literature on personality disorder [50, 52], techniques for schematic change need to be used discerningly. Contra-indications to use would include use with bipolar disorder patients who are, at the time of intervention, significantly depressed, hypomanic or manic; those with borderline personality traits; or dissociative disorders.
Schema-focused cognitive therapy
Schema-focused cognitive therapy [50, 51] is an integration of cognitive therapy with experiential techniques. The approach was originally developed for personality disorders and extends traditional cognitive therapy by emphasizing the therapeutic relationship, affective experience and the linking of early life experiences to present day functioning. Schemas (or core beliefs) are defined as ‘organized elements of past reactions and experience that form a relatively cohesive and persistent body of knowledge capable of guiding subsequent perceptions and appraisals’ [50], p.47]. Schemas are pervasive themes regarding oneself and others originating in childhood and elaborated through life. These experiences are encoded as core beliefs that are manifested later in interpersonal relationships, work and overall functioning, and determine the individual's resilience during times of adjustment, loss and trauma [50]. The beliefs and emotional memories that comprise schemas are generally accepted without question as a central part of an individual's identity and therefore are highly resistant to change [53]. In contrast to underlying assumptions, which are the target of cognitive therapy, maladaptive schemas involve unconditional beliefs. Whereas underlying attitudes hold out the possibility of beliefs being met (e.g. ‘If others approve of me, then I am worthwhile’), maladaptive schemas do not (e.g. ‘I am inadequate, so there is no point in trying’) [50, 51]. Maladaptive schemas or core beliefs are therefore more likely to be associated with poor functioning and avoidance than dysfunctional attitudes. Schemas are circular and self-perpetuating, and when challenged, the individual distorts information to maintain their validity. Rigid maladaptive schemas lead to significant disruptions to the individual's psychosocial functioning [50].
An examination of the individual's cognitive processing may reveal schemas such as those shown in Table 1. Expressed schema may, for instance, be associated with emotional deprivation, defectiveness and incompetence, unrelenting standards, poor self-discipline or emotional inhibition. Initially, the therapist and patient select a primary schema where the solution is likely to have some impact on changing other problematic schema [24]. The schemas are interactive, so that a sense of being defective, may for instance activate the incompetence or unrelenting standards schemas.
Table 1. Examples of schemas typically associated with bipolar disorder
Schemas function within the individual through three processes: schema maintenance, schema avoidance and schema compensation. Schema maintenance serves to perpetuate the schema through highlighting consistent information and minimizing contradictory material. Behaviours generated by the schema (e.g. partner selection) also keep the schemas intact. Schema avoidance refers to the methods used to avoid activation of schema. Cognitive, affective and behavioural avoidance is used to ward off the distress associated with confronting the schema. For example, avoiding disclosure or denial of illness may serve to avoid activation of the defectiveness schema, (e.g. ‘What would people think of me if they knew about my bipolar disorder?’). Schema compensation refers to the process by which the individual acts in ways opposite to what would be expected given the schema. For example, overworking and putting unrealistic pressure on oneself to achieve when feeling well may be an attempt to compensate for feelings of inadequacy. While this may be initially functional, increased psychosocial stress is in turn likely to trigger a further illness episode. The excessive emphasis on external attainments such as academic/financial achievements, appearance or status, may also be used as attempts to compensate for feelings of defectiveness. Underachieving through procrastination in work or study may occur as a compensatory behaviour associated with a fear of failure. It is possible for the individual to function relatively effectively with these schemas operating at covert levels. However, in the context of a significant life stress, the failure to acknowledge the underlying vulnerability is likely to lead to a deterioration in psychosocial functioning.
Whereas cognitive therapy employs more directive attempts for altering distorted beliefs, schema-focused cognitive therapy uses emotive, interpersonal, cognitive and behavioural interventions. Schemas are most effectively challenged during times of affective arousal [50]. The emotive techniques are derived from the experiential and Gestalt therapies and involve the use of imagery, role playing and current life experiences to express affect. The therapist also provides a therapeutic relationship that counteracts the schema and tests the reality of beliefs through direct interaction. Cognitive techniques are also used in changing deeper structures through tracing the schema and its origin in childhood and examining how they have been reinforced through adolescence and adulthood. While empathizing with the patients, the therapist also confronts them with evidence that discredits the schema. Finally, behavioural patterns that reinforce the schema are targeted in addition to environmental changes when necessary. Fundamentally, the approach helps patients to let go of beliefs based on fear and emotional memories and become more adaptive in their decision making, work and dealing with others.
Modified schema-focused cognitive therapy for bipolar disorder
Based on a model originally developed for personality disorders [50], the authors have devised a modified schema-focused cognitive therapy incorporating cognitions associated with adaptability to illness [45] and adaptability styles [46].
Illness phase: The first aspect of treatment focuses on symptom management and the patient's experience of illness. Particular attention is directed towards fostering an understanding of what it means to have a diagnosis of bipolar disorder and how it has affected the individual's life. Interventions include psychoeducation, crisis intervention strategies, identification and management of prodromes, and cognitive and behavioural strategies for managing depression, hypomania and mania.
Self-schema phase: The second phase of treatment examines the patient's self-schema eliciting cognitive vulnerabilities that may be impairing their acceptance of themselves, their illness and their functioning. Particular attention is directed to identifying core beliefs such as those associated with the need for approval, worth based on achievement, defectiveness/failure, alienation and the trustworthiness of others. The expression of affect is encouraged as a mechanism for modifying such schema. The Young Schema Questionnaire [50] is used to identify the patient's schema. Emotional empathy or validation [52] is used by the therapist to convey to the patients that their behaviours and choices are understandable. The current adaptability of such choices is then examined.
Illness and self-schema phase: The final phase of the treatment module considers how the patient is assimilating past experiences of illness, trauma and vulnerability, and the current meaning assigned to the illness experience. Therapy focuses on the patient's assimilation of their bipolar disorder (i.e. looking back in time) and adaptation (i.e. managing the present and planning for the future). It considers the patient's new insights, new relationships with partner, family and friends, work colleagues and the eventual construction of a healthy selfconcept.
Treatment outcome
The use of schema-focused cognitive therapy has been described in case reports for personality disorders [54, 49] and bipolar disorder [23] with encouraging results. Although the approach was originally reported over 10 years ago [50], few randomized controlled trials of this technique for any psychiatric conditions have as yet been conducted [55], and none in bipolar disorder.
The Bipolar Disorders Clinic at Prince of Wales Hospital, Sydney is currently conducting a randomized controlled trial evaluating schema-focused cognitive therapy for bipolar disorder, in combination with pharmacotherapy. Patients receiving schema-focused cognitive therapy participate in 20 sessions of therapy on a weekly basis according to the above treatment regime. The comparison group receives treatment as usual sessions as required with the patient's general practitioner or psychiatrist; the objectives being simple psychoeducation, medication adherence and mood monitoring. The treatment period for all patients is 6 months with a 12-month follow-up period. The primary outcome measures are time to relapse, number of days unwell, number of recurrences, index hospitalizations, clinical global impression and psychosocial functioning. Secondary measures include mood (depression, hypomania and mania), hopelessness, extent of helpful versus unhelpful automatic thoughts, dysfunctional attitudes, self-control and medication adherence.
Conclusions
It is hypothesized that modified schema-focused cognitive therapy holds considerable potential in addressing the poor functionality associated with a subgroup of patients with bipolar disorder and may offer an innovative treatment option for patients with this condition in the future.
Footnotes
Acknowledgements
We thank the Australian Rotary Health Research Fund for financially supporting the research.