
Abstract
The advent of effective antipsychotic medication in the 1950s was a major advance for the treatment and management of psychotic symptoms in individuals with schizophrenia and related disorders. Numerous studies attest to the effectiveness and efficacy of these agents in not only bringing under control the ‘positive’ symptoms of psychosis during acute episodes but also reducing the frequency of relapses and ameliorating the overall prognosis of the disorder [1]. However, with the older or ‘typical’ antipsychotic agents, the therapeutic gains were in many cases offset by the burden of side-effects, especially those resulting from dopamine blockade in extrapyramidal brain pathways, or late complications such as tardive dyskinesia (TD) [2]. The introduction, in the late 1960s, of clozapine – an agent which reportedly causes no, or only limited, extrapyramial side-effects (EPSE) in the majority of patients, spurred researchers to discover further compounds which have antipsychotic efficacy without EPSE [3].
Several such novel, or ‘atypical’, antipsychotics (risperidone, olanzapine, and quetiapine) have been widely marketed in Australia. Uptake of these agents by prescribers has been rapid, with recent surveys showing one half (May 1998) [4] to two thirds (April 1999) [5] of all antipsychotics prescribed in Victorian mental health services being either olanzapine, risperidone, or clozapine. However, there has been little attention paid to establishing the patient profiles associated with the different agents. Furthermore, despite claims of better side-effect profiles and higher acceptance by patients of atypical, as opposed to typical antipsychotic drugs [3], there have been very few studies focusing on patients’ perceptions and attitudes towards them in a naturalistic setting [6–8].
An opportunity to assess patterns of antipsychotic drug use in a large population-based sample, as well as to establish perceived benefits and side-effects of such agents, was afforded by the Study of Low Prevalence (Psychotic) Disorders, a component of the National Survey of Mental Health and Wellbeing, 1996–1999. The details of the study have been published elsewhere [9]; the current report focuses solely on medication use and associated variables, as reported by patients. We analyse and summarize those patient reports with cognizance that medication is only part (though undoubtedly a very important one) of what should be a comprehensive biopsychosocial treatment package for persons with psychotic disorders. Depending on how its benefits and costs (in terms of side-effects) are perceived by the patients themselves, it may either facilitate or hinder the effects of other, including behavioural and social, components of management.
For ease of nomenclature, we henceforward include in the ‘typical’ category the older antipsychotic agents such as chlorpromazine, thioridazine, haloperidol; when used in long-acting intramuscular injection formulation, the term ‘typical depot’ is applied. ‘Atypical’ refers to clozapine and the newer generation antipsychotic agents olanzapine and risperidone (these were the only such agents on the Australian market at the time of the Survey).
Design and methods of the low prevalence study
The study was conducted over four areas; the Australian Capital Territory, Queensland, Victoria and Western Australia as a two-phase survey including: (i) a census and screening for psychosis of all individuals, aged 18–64, who made contacts with mental health services during a period of one month in 1997; and (ii) interviews with a stratified random sample (n = 980) of the screen-positive individuals (n = 3800) using a standardized instrument. Screening took place in mainstream public health services (both inpatient and outpatient services), in private psychiatric practices, and in general practices. Across Australia, a total of 14 inpatient units, 13 outpatient units, 3 residential care units and 20 community mental health clinics, as well as 88 general practitioners and 52 private psychiatrists participated in the data collection. In order to identify individuals with psychosis who were living in marginalized settings and not in current contact with the services, screening was also conducted at 136 other potential points of contact for such persons such as hostels, shelters, refuges, charity services or other stop-gap accommodation. In addition, administrative in- and outpatient records were used to identify individuals with a psychotic disorder who had been in contact with mental health services within three years of the census month but not in the census month. A further 146 individuals among those past but not current users were randomly selected for interview. The bulk of the interviews were conducted between September 1997 and January 1998 by clinical researchers using a specially designed instrument (the Diagnostic Interview for Psychosis (DIP)). Further to a detailed examination of diagnostic symptoms and history of disease, the standardized interview included a wide range of items dealing with psychosocial, economic and quality of life issues, including the level of disablement respondents were experiencing, their use of services and their perceived needs. With respect to medication, respondents were asked about their current use (within one month of the date of interview) of medication for problems related to their mental health. A list containing both the generic and trade names of drugs was used to help participants identify their medication correctly. Further questions assessed their perception of how helpful the medication was that they were using, and sideeffects they were experiencing. Only medications that had been used for at least one month were included.
It is important to stress that the data collection on medication was entirely on the basis of patient reports, and that neither evaluation of efficacy nor assessment of compliance were among the aims of the study. However, appraisal of subjective well-being and of positive or negative attributions related to treatment – an issue rarely discussed in the psychopharmacological literature – was an important aim and we report below the relevant findings of the study.
Results
The majority of the sample were identified in mainstream inpatient (23.3%) or outpatient (37.7%) services in the census. A further 15.4% were identified through private psychiatric and general practice settings, and 10.7% were identified as marginalized and not in contact with services in the census month. Another 13.0% had been in contact with mainstream services within three years of the census but not in the census month. The proportion of interviewed patients by catchment area was: 16.3% Australian Capital Territory; 27.3% Queensland; 32.7% Victoria; and 23.7% Western Australia. By research diagnosis (based on DIP interview and the OPCRIT diagnostic algorithm [10]), 52.7% had an ICD-10 diagnosis of schizophrenia; 10.7% had a diagnosis of bipolar affective disorder; and 36.6% had another ICD psychotic illness including schizoaffective disorder and depressive disorder with psychotic features. The mean length of illness in the interviewed sample was 15.0 years (SD 10.9). The percentage of males in the total sample was 58.9%. This percentage varied by diagnostic group: 66.4% of the schizophrenia group were male, 51.2% of those with bipolar affective disorder, and 50.2% of patients with ‘other psychoses’.
Frequency of psychotropic drug use by class of medication
Overall, 998 persons (88.6% of the total interviewed sample) had, in the month prior to interview, been receiving any psychotropic agent (i.e. any antipsychotic, mood stabilizer, antidepressant, or benzodiazepine). Some 54.3% of the interviewed sample were using ‘typical’ antipsychotic agents, with 24.8% of all respondents receiving these in depot form. With respect to ‘atypical’ antipsychotics, 8.3% of the respondents were on clozapine, 13.3% on risperidone, and 8.8% on olanzapine. There was no significant difference in antipsychotic use by gender, but mood stabilizers and antidepressants were more commonly used in women (29.6% and 30.7%, respectively, as compared to 17.9% and 21.7% in men). Table 1 shows that typical and atypical antipsychotics were used in patients of any age, but atypicals tended to be more commonly used in the younger respondents. The breakdown of medication use by length of illness (years since first onset) indicates that the use of typical antipsychotic agents was significantly higher (χ 2 24.1; 1 df; p < 0.000) in patients with total length of illness 15 years and over as compared to patients with less than 15 years of illness, while the use of olanzapine and risperidone showed the opposite trend. The trend for clozapine was one of increasing use in patients with 5 or more years history of illness (Table 1).
Class of current medication† by sex, age group, diagnosis, and duration of illness Medication
Frequency of antipsychotic use varied by treatment setting. The frequency of typical depot medication was highest in the public mental health settings (27.5%), but that a relatively high level of use of typical oral antipsychotic use (46.8%) was also reported in the private sector. The frequency of use of risperidone or olanzapine was around 25.9% in public settings, rather lower (17.9%) in private practice, and very low (5.8%) in those patients who were living in marginal accommodations. The bulk of clozapine prescribing was in the public sector, where 11.8% reported taking it.
Polypharmacy
Overall, 52% of the respondents (58% of those on medication) had used more than one psychotropic medication in the month prior to interview. Around a third of the patients were on psychotropic medication from two different classes (e.g. an antipsychotic and a mood stabilizer, or a typical and atypical antipsychotic), and close to 10% were on psychotropics from three or more classes. Table 2 shows those combinations of medications used by more than one per cent of the sample. Typical antipsychotics were most likely to be combined with another agent, usually a mood stabilizer or antidepressant, or both. Combination of typical and atypical agents was found in around 5% of subjects. Benzodiazepine use was highest in patients on typical antipsychotics.
Combinations of classes of medication used by one per cent or more of the total population in month prior to interview
Use of ‘typical’ and ‘atypical’ antipsychotic agents by diagnosis, current symptom profile and longitudinal pattern of course
Table 1 shows that atypical agents were not being used solely for patients with a diagnosis of schizophrenia. Indeed, 17.4% of patients with bipolar affective disorder, and 25.7% of those with ‘other psychosis’ were receiving an atypical antipsychotic. Mood stabilizing drugs were most likely to be used in patients with bipolar affective disorder. Antidepressant use was reported in 16.4% of patients with schizophrenia and in over a third of those with ‘other psychosis’.
In order to assess whether the use of particular medications was associated with specific current psychopathology, symptoms elicited as present in the last month were grouped into: (i) hallucinations in any modality; (ii) delusions; (iii) depressive symptoms such as pervasive depressed mood or loss of ability to enjoy life; (iv) manic symptoms, including intense elation or pervasive irritability; (v) negative symptoms such as poverty of speech and/or restricted/blunted affect; and (vi) disorganization, including any bizarre behaviour, inappropriate affect, or incoherent speech. Medication use as per each symptom cluster is presented in Fig. 1.
Current medication use by present state symptom profile. ▪, hallucinations; □, delusions; □, affective symptoms; □, mania; ░, negative symptoms; □, disorganization.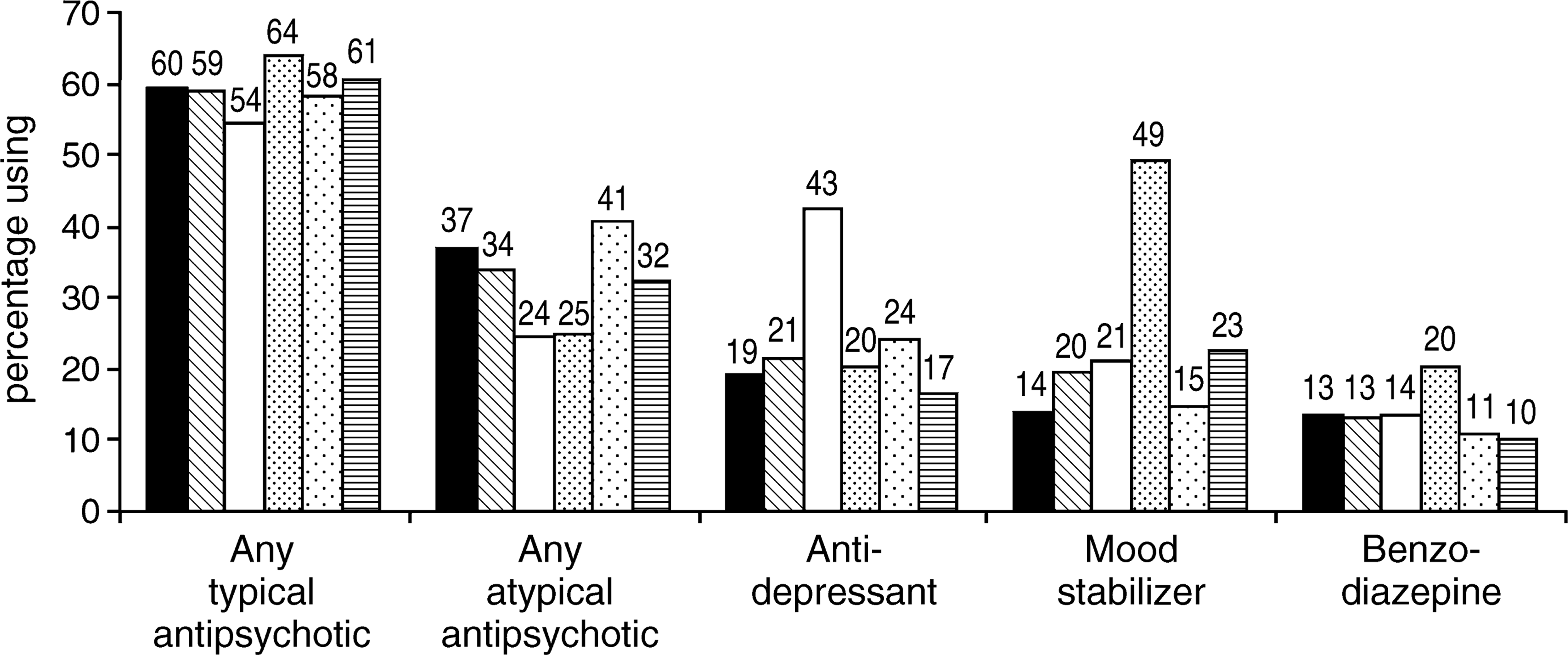
In terms of longitudinal pattern of course, 31.1% of patients who had had only a single illness episode of relatively recent onset were using typical antipsychotics and 19.8% were using atypicals other than clozapine; clozapine was mostly prescribed to patients with a chronic, continuous or recurrent illness course (see Fig. 2).
Current medication use by course of disorder. ▪, single episode; □, multiple episodes, good recovery; □, multiple episodes, partial recovery; ░, chronic, little deterioration; □, chronic, clear deterioration.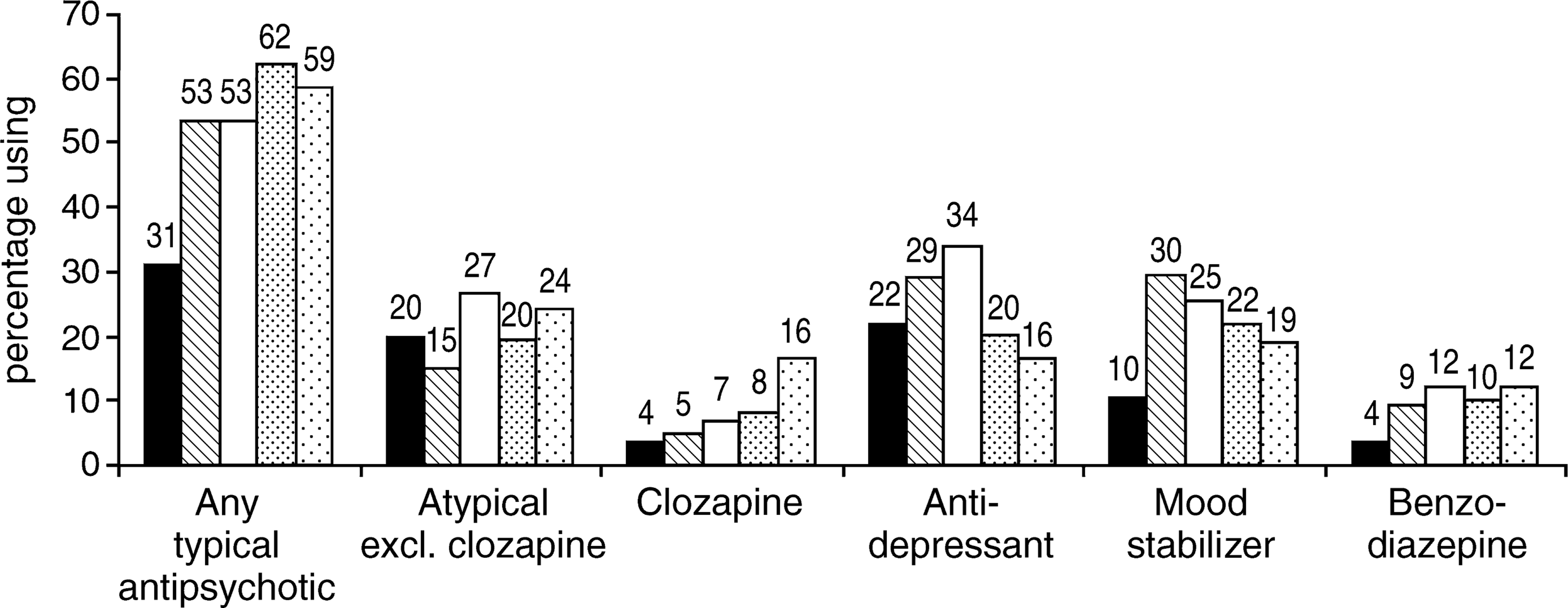
Perceived efficacy
Respondents were asked to rate each of their medications as either ‘not helpful’, ‘helpful’, or ‘very helpful’. These perceptions were analysed in patients with and without insight into their illness (OPCRIT criteria). Figure 3 details these responses. For typical agents, depots received the lowest levels of endorsement as ‘helpful’ or ‘very helpful’. The atypical agents were generally considered more favourably, with both olanzapine and risperidone having only around 10% ratings of ‘not helpful’; only 5.3% of respondents considered clozapine to be ‘not helpful’. Overall, patients without insight rated the usefulness lower than those with insight, across all agents.
Helpfulness of current antipsychotic medication by state of insight. □, not helpful; □, helpful; □, very helpful; ▪, impossible to assess.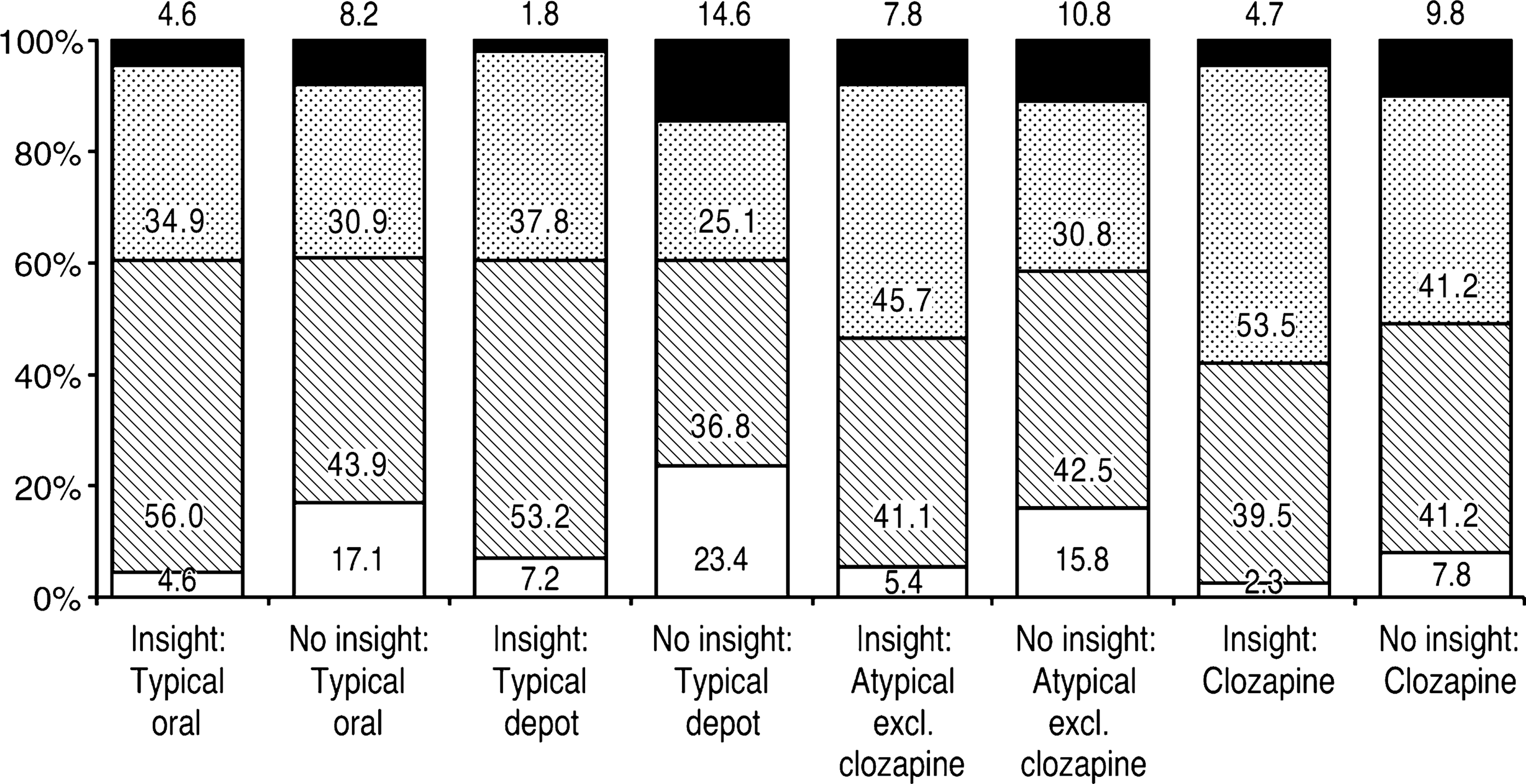
Reported side-effects
Respondents were asked to choose any number from a range of 14 possible side-effects. The wording of the interview questions was: ‘Did any of these medications have effects that you did not like? I will now read some complaints that people sometimes attribute to medication. Have you experienced any of these in the past month? – muscles feeling stiff or tensed up – inability to relax – hands, arms or legs shaking or trembling – feeling of inner restlessness – inability to stand still – drowsiness or sleepiness during the day – trouble with eyesight – dry mouth or mouth more watery than normal – unwanted tongue movement – difficulty swallowing – difficulty starting walking – slowing down of movements – shuffling along – unsteadiness when standing or walking’.
In order to assess side-effects associated with each specific class of medication, analysis was restricted to those 434 (38.5% of the total) respondents who reported being on only one class of medication. The majority endorsed at least one side-effect item, though a sizeable minority, including 21% of those on typical oral and a similar proportion of those on atypical agents other than clozapine, reported no sideeffects. In comparison, lower percentages −17% of those on depot typical agents and, notably, only 8% of those on clozapine – reported no side-effects. However, there was no overall significant difference in the number of side-effects reported for each class of antipsychotic, the mean being around 3.5 (3.9 for typicals, 3.3 for risperidone/olanzapine).
In order to explore whether patients’ subjective reports of sideeffects conformed to expected clinical patterns, we conducted principal components analysis using the dichotomised responses (1 = presence; 0 = absence or impossible to ascertain) from 893 patients reported as being on medication during the month preceding the interview. Because the side-effects items were dichotomous variables, a method that corrects for binary data by employing a matrix of the tetrachoric correlations was used in the factor analysis [11].
After rotation using a varimax orthogonal rotation procedure, three factors were identified which together explained 48.4% of the variance. The item content of the 3 factors shows that, by and large, the clustering of side-effects as perceived by patients corresponds to established clinical syndromes of psychotropic drug side-effects (see Table 3).
Reported side-effects: factors and rotated factor loadings
For further analysis, we then grouped the reported side-effects on the basis of clinical considerations as follows: (i) sedation: drowsiness or sleepiness during the day; (ii) parkinsonism: any of muscles feeling stiff or tensed up; hands arms or legs shaking or trembling, slowing down of movements, unsteadiness when standing or walking, difficulty starting walking, shuffling along; (iii) akathisia: any of inability to relax, inability to stand still, feelings of inner restlessness; (iv) tardive dyskinesia: unwanted tongue movements; (v) anticholinergic side-effects: dry mouth and/or hypersalivation and/or trouble with eyesight; (vi) other: difficulty swallowing.
Reference to Figure 4 reveals that the perceived side-effect profiles of the different classes of antipsychotics were divergent in some domains. Items compatible with parkinsonian side-effects were more commonly endorsed by those patients on typical agents (60% vs 49% for atypicals). Objective and subjective restlessness (akathisia) was also more common in individuals on typical agents. However, there was very little difference between the groups in proportion of patients reporting TD (9–12% variance across the groups). Importantly, around half of respondents on all agents reported diurnal drowsiness. Anticholinergic side-effects (dry mouth/hypersalivation) were least commonly described by those on risperidone/olanzapine (45%); more commonly by patients on typical agents (58%); and most commonly by patients on clozapine (78%).
Side-effects of current antipsychotic medication. ▪, sedation; □, extrapyramidal side effects; □, akathisia; □, tardive dyskinesia; □, anticholinergic side effects; □, other.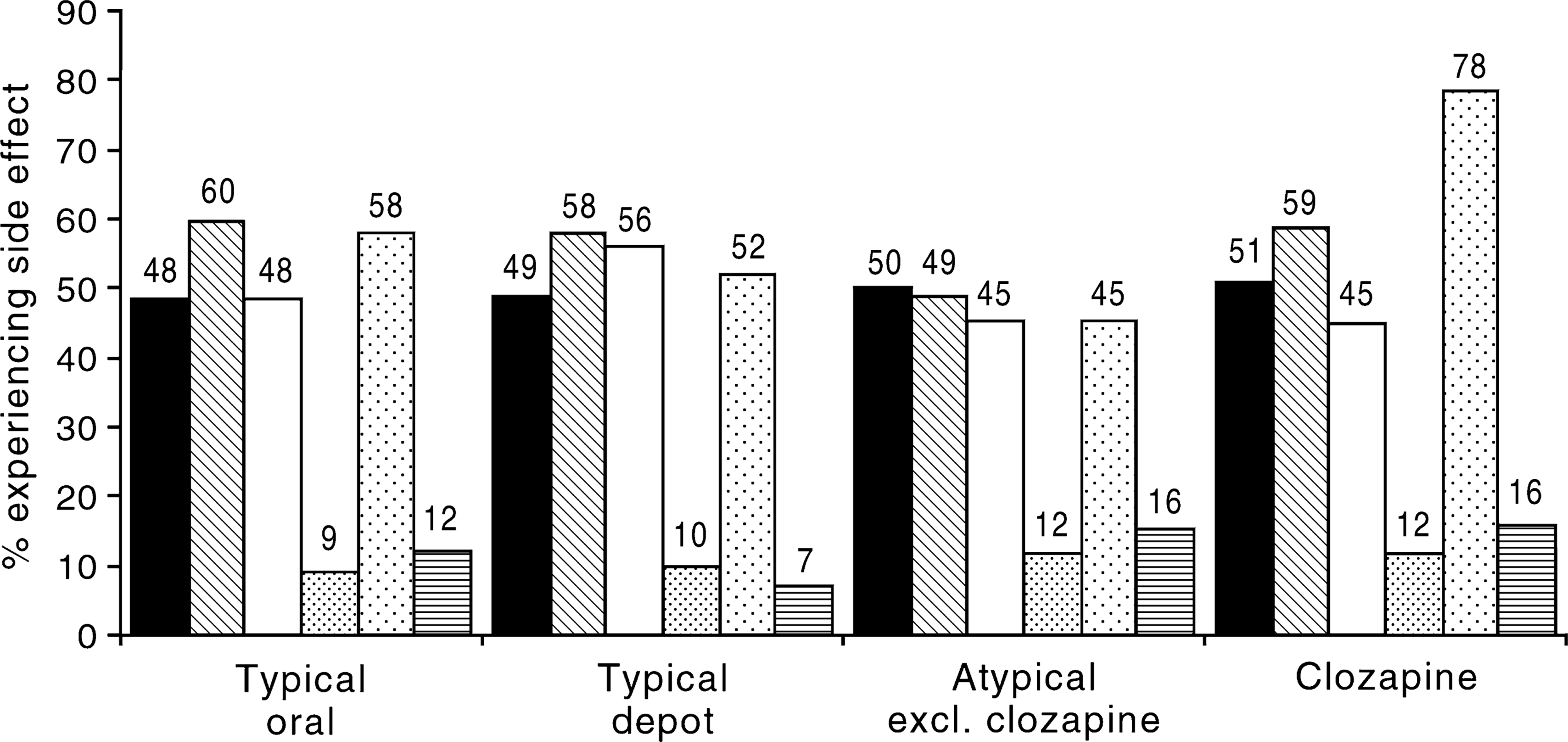
Experience of side-effects and satisfaction with overall quality of life
Respondents who described themselves as ‘mostly satisfied’ with their life in the past 12 months reported, on average, 2.9 specific sideeffects they attributed to antipsychotic medication. In contrast, those who were ‘mostly dissatisfied’, had on average 4.2 side-effects attributable to medication. The difference was significant (t = −6.34, P < 0.000). Thus, there was an association between the experience of side-effects and the subjective evaluation of quality of life.
Discussion
Inevitably, self-reports of medication side-effects might be inaccurate in some cases, but there is no reason to suspect systematic bias in this regard as the overall pattern of patients’ reported side-effects (described by principal components analysis) agrees well with clinical observation. This being an interview-based study which, especially in its medication use inquiry, relied exclusively on information supplied by the respondents, implied that we were unable to independently ascertain doses of drugs used, nor total duration of treatment, though respondents were asked to record only those medications they had been receiving for at least the prior four weeks. In those patients on more than one agent, some difficulty was bound to occur in determining which particular agent was responsible for which sideeffects. Another limitation was that, in this study, we did not collect data on sexual side-effects and weight gain, noted to be particularly problematic for risperidone, olanzapine and clozapine [3]. Despite these caveats, the data provide an insight into the subjective evaluation of side-effects and benefits of antipsychotic agents, as experienced by the patients themselves. Patients’ perception of the side-effects they attribute to medications they are receiving are useful in the clinical setting not least because the side-effect burden is a predictor of noncompliance with medication [12]. The sampling frame of the study was epidemiologically sound, and allowed a comparison of rates of reported use of various agents across treatment settings, as well as an exploration of their clinical correlates such as current symptoms, length and pattern of illness.
It should be noted that the interviews for this study were conducted in 1997–1998 and the data are already dated in terms of the proportion of patients on atypical antipsychotics. Over the last 3 years, there has been a marked increase in the proportion of patients with psychosis who are being prescribed atypical antipsychotics. In a study conducted in May 1998 in an inner-city Melbourne catchment area Keks et al. [4] found that, of 661 patients on antipsychotic medication, already some 53% were being prescribed atypical agents (42% risperidone, 37% olanzapine, and 21% clozapine). The latest published survey [5] of antipsychotic use in an Australian mental health service (Geelong, Victoria) revealed that of antipsychotics prescribed, 30.8% were clozapine, 22.9% olanzapine, and 14.3% risperidone (total 68%). Although successful marketing may in no small measure account for this rapid increase in the prescribing of atypical antipsychotics, clinicians are increasingly compelled by studies showing a lower side-effect burden associated with the atypicals [3, 13, 14] and are choosing them for their patients. Indeed, the Australian National Guidelines for the treatment of first psychosis patients advocates the first-line use of atypical agents, and this practice is now commonplace.
However, the evidence in support of an all-aspect superiority of the atypical antipsychotics, especially when set against the background of their higher cost, remains inconsistent. For example, a recent meta-analysis [15] concluded that low dose haloperidol (< 12 mg/day) was as effective and as well tolerated as typical agents. Evidently, a broader range of factors, including the perception by consumers, need to be taken into account in any debate about the place of the atypical antipsychotics in the management of psychotic disorders. It is thus of interest that, in the current study involving a nationally representative sample of people with potentially disabling psychotic illnesses, 40.8% of the patients taking atypical antipsychotics viewed them, from their own experience, as very helpful compared to 31.7% for the patients on typical agents. It is also of interest that atypical antipsychotics were associated with lower scores on all psychotic and mood symptoms, relative to typical agents. In particular, atypical agents were associated with low rates of affective symptomatology, a reflection, perhaps, of the putative antidepressant and mood stabilizing properties of these drugs [16].
We are not aware of other studies in which patients have been asked to rate whether they believe their medication is beneficial for them. Although we did not specify which particular symptoms we were asking about, and results thus reflect a global satisfaction rating, it is not unreasonable to assume that the overall ‘helpfulness’ ratings by patients is a composite of perceived efficacy weighed against side-effect burden. Thus, the reported higher satisfaction with atypicals is consonant with the findings of lower symptom ratings and overall reduced side-effects of the atypicals compared with typicals. Among the latter, depot antipsychotics fare worst in terms of patient perception of efficacy. This might, in part, reflect the fact that depots tend to be used with patients who would otherwise be non-compliant, lack insight into their illness, and resent the fact that they are on medication at all. On the other hand, depot antipsychotics, being typical agents, would be expected to carry a high side-effect burden (as borne out in the current study).
The present study also revealed that atypical antipsychotics were not prescribed exclusively for patients with schizophrenia. This is similar to the findings of Keks et al. [4] who found that, of all patients on atypical antipsychotics, only 74% met DSM-IV criteria for schizophrenia. Similarly, Callaly and Trauer [5] reported that 11.9% of all prescribed atypical agents were used for patients with schizoaffective disorder; 10% for patients with bipolar disorder; and 2.5% for patients with major depression. These findings suggest that Australian psychiatrists are not restricted in their prescribing practice by the guidelines issued by the Therapeutic Goods Administration, nor the results of the randomized controlled trials which the pharmaceutical industry is required to conduct to have drugs approved for use. The widespread ‘off label’ use of atypical antipsychotics in Australia and internationally suggests that the current policy of rigidly restricting the indications for atypicals to a specified nosological category runs contrary to clinical judgement and may be counterproductive as regards the maximization of benefit from these therapeutic agents.
Polypharmacy is another clinical issue highlighted by the results of this study. While it tends to be considered poor psychiatric practice, it is far from unusual in clinical settings in Australia [4, 5] and elsewhere [16], notably during change-over from typical to atypical agents; in using an atypical to supplement a depot; or in the treatment of comorbid depression in patients with schizophrenia spectrum conditions. These data again suggest that, in the absence of firm data to support or challenge benefit from combinations of antipsychotic agents, clinical judgement often overrides pharmacological purism. The widespread use of mood stabilizers and antidepressants in the current survey reflects, in part, the diagnostic heterogeneity of the sample but also underlines the clinical reality of extensive depressive comorbidity in schizophrenia and related disorders [17].
We draw attention to aspects of the patient-reported profile of side-effects that are somewhat at odds with data from clinical trials. Some form of extrapyramidal side-effects was described by the majority of respondents, for both typical and atypical antipsychotics, although their frequency was slightly lower in those on risperidone/ olanzapine. The latter agents have been shown in the majority of clinical trials to cause less EPSE than typical antipsychotics, though the meta-regression analysis of Geddes et al. [15], cited above, concluded that despite this, typical agents at dose below 12 mg/day of haloperidol (or equivalent) are as well tolerated as the atypicals. However, the high rates of reported EPSE in patients on clozapine are unexpected, as clinical trials suggest that this agent causes little or no EPSE [3]. Notwithstanding the possibility that some patients, especially those who had recently been switched over from a typical antipsychotic to clozapine may have inaccurately attributed side-effects experienced earlier to clozapine, we suggest that further studies, using existing clozapine prescribing databases, are needed to clarify this issue. Similarly, akathisia – one of the most distressing sideeffects of antipsychotic medication – was predictably reported most commonly by patients on typical depot agents, but, unpredictably also by nearly half of those on any of the atypical agents. This appears contrary to both clinical practice and trial data, which show much lower rates of akathisia with the newer antipsychotics [3]. It is likely that respondents were interpreting restlessness due to other causes (e.g. anxiety) as caused by medication, and thus it being labelled as ‘akathisia’. Finally, the reported frequency of symptoms related to putative TD is not inconsistent with their expected rate of occurrence in a relatively severely affected sample such as this [18]. The finding that there was little difference between the agents with respect to rates of TD might well be a reflection of prior medication exposure, rather than being directly consequent upon current use.
Conclusions
We report here findings from a representative Australian sample of patients with psychotic disorders, related to the patients’ subjective perception and evaluation of the benefits and adverse effects of pharmacological treatment. The vast majority were receiving antipsychotic medication, and a substantial proportion were also on antidepressant and mood stabilizing agents. Atypical antipsychotics tended to be associated with lower levels of psychotic and affective symptomatology, and a generally lower side-effect burden. However, even these newer antipsychotics are neither free of side-effects nor associated with a full resolution of symptomatology. More work needs to be done in determining the optimal medication regime for each individual patient, and in exploring psychosocial treatments which can augment medications in the holistic care of people living with psychosis.
Footnotes
Acknowledgements
The present paper is based on data collected in the framework of the Collaborative Study on Low-Prevalence (Psychotic) Disorders, an epidemiological and clinical investigation which is part of the National Survey of Mental Health and Wellbeing, Australia 1997–1998. The study was funded by the Commonwealth Department of Health and Aged Care, the Australian Capital Territory Department of Health and Community Care and the Psychiatric Epidemiology Research Centre, Australian National University.