
Abstract
Emergency department staff frequently care for patients who threaten violence or exhibit violent behaviour as a consequence of psychiatric illness or acute crisis, often complicated by drug and alcohol intoxication or overdose. It is sometimes necessary to restrain such patients during their period of assessment and observation in the emergency department to reduce the risk of harm arising from violent behaviour to staff, other patients and visitors, and the patients themselves [1].
The incidence of violent episodes in urban Australasian emergency departments is estimated to be 2.8 violent episodes (verbal and physical) per thousandpresentations [2]. While no data are available, it is likely that the rate of patient restraint in urban Australasian emergency departments is of a similar magnitude. The implementation of restraint invokes a number of medicolegal, occupational safety and patient safetyconcerns [1,3–6]. However, no published data exist regarding the practice of restraint in Australasia. The objective of this study was to document the rate of restraint utilization, types of restraint used and the training in and audit of restraint practices in Australasian emergency departments.
Method
A survey was undertaken by mailed questionnaire to 96 emergency departments in Australasia and New Zealand with a specialist director of emergency medicine. In addition, a further survey of 20 emergency departments in regional hospitals with over 200 beds with no specialist director of emergency medicine was undertaken.
Of the 116 hospitals surveyed, 17 were private hospitals, and the remainder public hospitals. Four weeks after mailing the questionnaire, non-responders were contacted by facsimile and telephone.
Recipients were asked to provide information concerning the types of restraint used in their department (manual, mechanical, chemical, seclusion room), the estimated frequency of use for each type of restraint, whether written policies or guidelines concerning restraint were in place, and if so, whether audit of such policies or guidelines was undertaken. In addition, recipients were asked to provide information on the composition of the typical ‘restraint team’ used in their emergency department and which staff members had authority to implement restraint. Information concerning the training, both formal and informal, of medical staff was sought. The rate was calculated by dividing the estimated number of restraint episodes by the combined annual census of the hospitals. Survey responses were collated in a Filemaker Pro database (Filemaker, http://www.filemaker.com) for analysis.
Results
A total of 79 responses (68%) was received from the 116 hospitals. The response rate was highest from public hospitals with a specialist director of emergency medicine with 68 responses (71%). Sevenof 17 private hospitals responded (41%), while 11 of 20 rural hospitals without a specialist director of emergency medicine responded (55%). On account of the small numbers in the other groups, only the responses from public hospitals with a specialist director of emergency medicine were subjected to detailed analysis (n = 68)
Rates of restraint
The overall estimated rate of restraint among respondents was 3.3 per 1000 presentations. The estimated rate of chemical restraint in public hospitals with a specialist director was 1.7 per 1000 patient visits, and the estimated rate of use of a seclusion room in emergency departments with a seclusion room was 1.3 per 1000 visits. The estimated rates of manual and mechanical restraint were 0.3 and 0.8 per thousand visits respectively (Fig. 1).
Estimated rates of restraint utilization in Australasian emergency departments.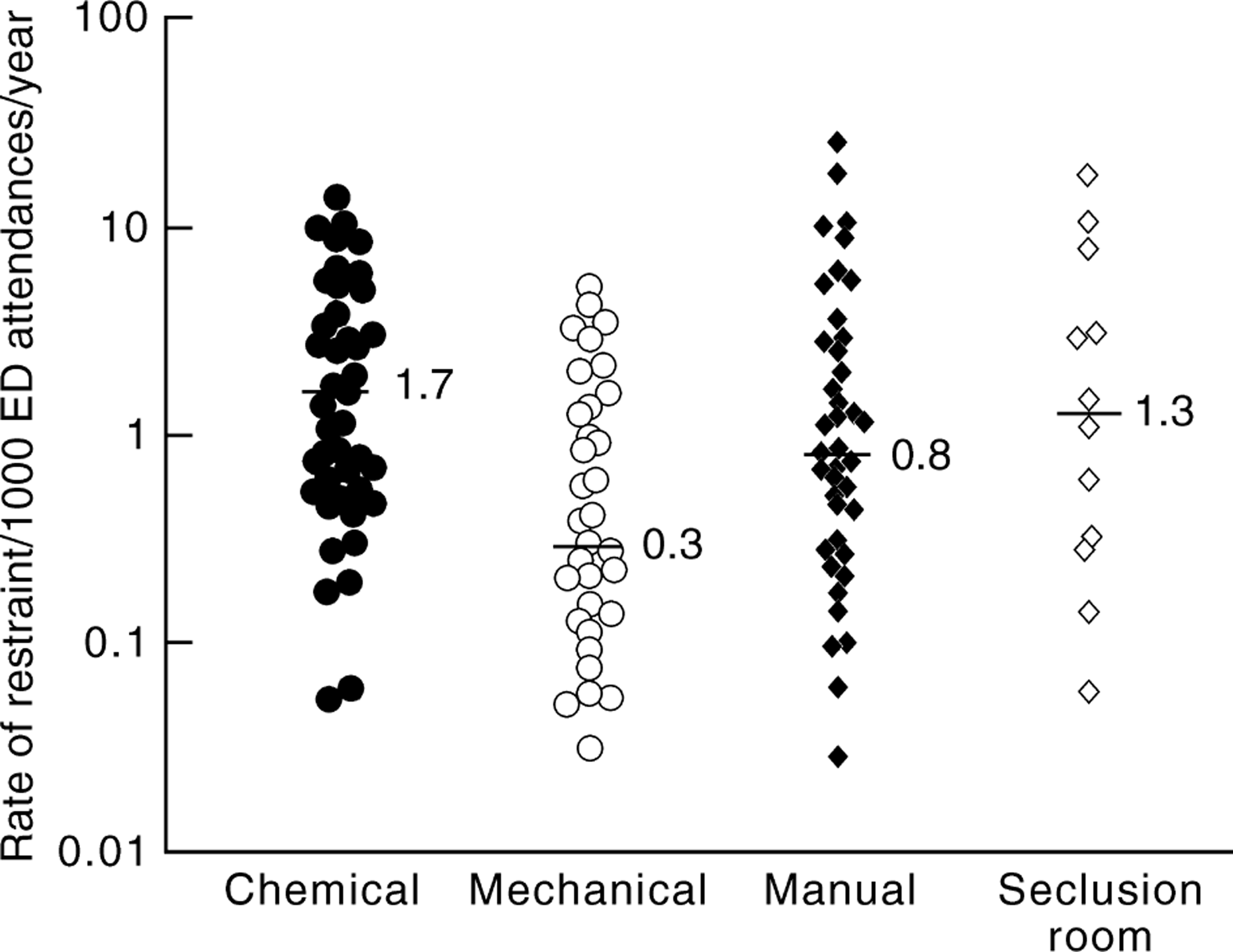
Restraint practices
All responding hospitals use chemical restraint. Restraint practices in the public teaching hospitals with a director of emergency medicine are shown in Table 1. Manual restraint was usually used in the public hospitals with a specialist director of emergency medicine as a prelude to chemical or mechanical restraint.
Restraint practices in Australasian public hospital emergency departments with a specialist director of emergency medicine
Restraint policy
In the public hospital group, 29 of 68 (43%) reported a written policy or guideline for chemical restraint, with similar percentages for manual and mechanical restraint.
Documentation and audit of restraint
A specific form for the documentation of restraint was used in only one department. Reported documentation was otherwise limited to the routine charting of nursing observations, the written prescription of restraint medications and ad hoc medical notes. Audit of restraint practices in emergency departments was uncommon. The rate of audit was less than 15% for each type, with only four hospitals (6%) auditing chemical restraint despite its ubiquitous use.
Drugs used in chemical restraint
The benzodiazepine sedatives midazolam and diazepam were used by 66 public hospital respondents with a specialist director of emergency medicine (97%). Fifty-six (82%) used midazolam and 40 (59%) diazepam. Thirty respondents (44%) reported using both drugs. Sixtysix respondents (97%) reported using major tranquillisers, with haloperidol being used by 63 respondents (93%).
Indications for restraint
Violence or threatened violence was the most frequently cited indication for restraint (52%). Psychiatric illness was the next most frequently cited indication (32%), with acute brain syndrome (10%) and drug/alcohol intoxication (4%) other commonly cited indications. Six responses cited dementia as an indication for mechanical restraint.
Contraindications to restraint
The commonest contraindication to restraint was stated to be the medical condition of the patient. In particular cardiorespiratory instability and head injury were frequently specified as contraindications to restraint. Danger to staff is cited by 36% of respondents as a contraindication to manual restraint.
Training in restraint
One-third of public hospitals with specialist directors of emergency medicine offered formal training in chemical restraint, but lessthan 20% offered medical staff training in other forms of restraint (Table 2). Up to 20% of responding departments offered no training in restraint, while the majority offered informal training. In particular, there was very little formal guidance concerning the use of seclusion rooms.
Training in restraint practices in public hospitals with specialist directors of emergency medicine (n =68)
Discussion
In our study, the estimated rate of restraint in Australasian hospital emergency departments was 3.3 per thousand patient visits, a figure of the same order of magnitude to the published rate of episodes of violence in Australasian emergency departments [2]. This figure is 10 times lower than the rate of physical or seclusion restraint usage (34 episodes per thousand presentations) in an urban teaching hospital emergency department in USA [7]. The difference may reflect sociodemographic differences in addition to differences in restraint indications and practices.
In a 1988 study of 127 emergency departments in the USA, each with an annual census of over 40 000 visits, 98% of the hospitals used ‘4 point’ physical restraints, 77% used chemical restraints and 61% used a seclusion room [8]. Eighty eight percentage of the departments had a written policy regarding management of violent patients and use of restraint, but in only 40% of the institutions did nurses receive formal training in the management of violent patients. Training of medical staff was not reported. Our survey of current Australasian practice shows a much lower use of seclusion rooms and a greater reliance upon chemical restraint compared to the USA figures. However, it should be noted that the reported rate of restraint varied enormously, particularly for manual restraint and the use of seclusion rooms (Fig. 1). This is likely due to the fact that responses were solicited without references to formally collected data. Of note in this respect is the fact that many reports of higher rates of restraint came from regional hospitals rather than large urban departments. In the absence of audit data this observation is of uncertain value. One would expect that violence and intoxication would be less frequent in rural hospitals compared with busy inner urban facilities.
Although seclusion rooms were used quite frequently in departments that have them, they are uncommon in modern Australasian emergency departments. Possible reasons for this include an opinion that the risks to patients are less well controlled with this technique than with chemical restraint. Additionally, essential physiological observation is much simpler and safer for both the patient and staff when chemical restraint is used in concert with modern physiological monitors than is possible with external observation complemented by periodic incursions into the seclusion room to elicit vital signs.
In many cases, the drugs used to chemically restrain an agitated patient may be considered to betherapeutic [9, 10]. The adverse effects are generally predictable and manageable by skilled emergency department staff. Physical restraint has a low but well described risk of sudden death [4, 5, 11].
The decision to implement restraint must be made unequivocally and implemented rapidly and expertly to minimize the risk to patients and staff. Well-defined and practised guidelines are essential if harm to patients and/or staff is to be avoided [1, 3, 6, 12].
Interpretation of the reasons cited as indications for restraint was impeded by the general brevity of responses. The frequent mention of ‘psychiatric illness’ as an indication for restraint should, we believe, be interpreted as the underlying diagnosis, and would be accompanied as well by a threat of self-harm or violence. Similarly, where drug intoxication, acute brain syndrome or dementia are cited, a risk of harm to self or others would be the immediate indication for restraint.
Medical instability was described as a common contraindication to restraint. Cardiorespiratory insufficiency and head injury were frequently cited as the underlying conditions which contraindicated restraint. This is of particular significance when chemical restraint is employed, but may be of concern when using any kind of restraint. While sedation may obscure significant clinical findings in patients with altered conscious state, it may be necessary to enable definitive investigations (e.g. head scan, lumbar puncture).
This study indicates that the implementation of restraint is a common procedure in large Australasian emergency departments, yet the use of formal policies, training, documentation and audit appears quite low compared with USA figures. The lower response rate we obtained from private hospitals and public hospitals without specialist directors of emergency medicine precluded meaningful analysis of restraint practices in these institutions. However it is unlikely that the use of policies, training, formal documentation and audit is higher in this group than in hospitals with specialist directors of emergency medicine.
A significant limitation of this study is that the low rate of audit reported by respondents suggests that a significant number of survey responses were based on estimates rather than documented figures, and thus may not accurately represent the true figure. However, in the absence of restraint registries, it is not currently possible to gather more accurate data regarding practice. Also, data gained by survey is by its nature retrospective and subject to recall and other biases. Despite these limitations however, the following conclusions may be made: (i) restraint, and particularly chemical restraint, is commonly used to ameliorate the risks to patients and staff in Australasian emergency departments arising from threatened or actual violence and acute psychiatric disorders; (ii) benzodiazepines and neuroleptic tranquillisers either alone or in combination are the drugs used in almost all emergency departments surveyed; (iii) it is usual for hospitals to have a written policy for restraint; (iv) the practice of restraint is rarely audited; and (v) there is little formal training of medical staff in use of restraint in Australasian Emergency Departments.
Footnotes
Acknowledgements
The authors would like to thank Dr John Reilley for his helpful comments.