
Abstract
There is a consensus in psychiatry, as in other disciplines, about its mainstream approach to its area of study: it would otherwise be an amorphous collection of approaches to mental illness. Over the years, the mainstream changes: currently psychiatry has an empirical approach using a scientific method applied to a series of syndromes described phenomenologically. In contrast, in the USA in the immediate post-war years, the dominant paradigms were aetiological, based on Freudian and neo-Freudian psychodynamic schools that have generally fallen from favour. In Europe the mainstream approaches were more complex: they included an organic school which hypothesised a molecular basis for, or substantially contributing to, illness and various analytic therapies which emphasised developmental and interactive approaches to illness. These disparate schools were largely displaced by a system, characterised by DSM-IV, in which aetiology was mostly eschewed. Very recently, a new aetiology has been emerging derived from molecular biology but at a highly reductionistic level, leaving unexplained many steps between this ultimate aetiology and actual behaviour. Whether molecular genetics will demonstrate a biological basis for the current phenomenologically based syndromes, or whether the mental illness cake will be cut up quite differently is, as yet, another, and open, question.
Commonly, the practising psychiatrist feels disquiet with an exclusively biological model. They feel social, developmental, psychological factors should enter into any understanding of cause. If pressed, a biopsychosocial model is cited. It is argued here that, while psychiatric syndromes are indeed influenced by biological, psychological and social factors, the concept biopsychosocial is too loose to be satisfactory. A theory capable of integrating these aspects is needed and at present, we do not have one. The components: ‘bio’, ‘psycho’, social and indeed genetic and developmental, start from different premises. The ‘bio’, including genetics, has its roots in basic sciences and their medical offshoots; neuroanatomy and physiology, neurochemistry, psychopharmacology and neuroradiology all use scientific paradigms and methods. Generally, these are highly reductionistic and only distantly related to behaviour and thought. The social component has its roots in sociology, heavily reliant on the supposition that social behaviour is influenced overwhelmingly by environment. Social psychiatry is generally concerned with pragmatic issues. The ‘psycho’ component similarly has its own concepts, not readily related to the others. The problems here are compounded by the multiplicity of psychodynamic paradigms. Development adds yet another dimension. A rarely considered factor is evolution, which imposes influences and restraints on behaviour. While this might logically be encompassed within the genetic component, it deals with a higher level of complexity than is normally encompassed in molecular biology.
Despite vigorous attempts to sidestep theory, neither empiricism nor phenomenology are theory-free. An empirical psychiatrist may say ‘I use this approach because it works’ but the criteria by which success is measured usually involves theoretical assumptions, even for the most dedicated empiricist. DSM-IV is an empirical classification. It has eliminated many aspects that are theory-dependent, particularly those dependent on psychodynamic theory, but the very language of psychiatry carries theoretical suppositions with it. The evident changes in contemporary psychiatric classifications and their various antecedents indicate that they are imperfect and changeable systems. Phenomenology similarly implies selection and value judgements about behaviour, which inevitably carry theoretical implications.
For the psychiatrist, there is perhaps a personal psychological reason for adopting an aetiological classification. Aetiology is more satisfying; ‘why?’ is more interesting than ‘what?’ Implicitly this drives us to seek an aetiological explanation.
Ways out of the dilemma
The way out of this dilemma, we suggest, is the development of a comprehensive theory of psychiatry, which can take into account all of these aetiologies. Now, multiple separate paradigms are used. One multilayered concept is needed which uses orthodox scientific concepts, extending from molecular biology to observed behaviour and including affect, thought, consciousness and volition. Most psychiatrists believe that no such paradigm exists. We believe this to be untrue and further believe that an evolutionary approach to psychiatry based on ethology, can serve this function.
In psychiatry, the methodology of ethology [1] the study of animal behaviour, has been applied only to a minimal extent in humans. Psychiatric paradigms have recently been adopted in companion animal behavioural medicine, but ethological principles have rarely extended to human psychiatry. In their initial observations, ethologists use observations as free of theory as is possible. From this material a detailed description of each animal's behaviour in its individual, social and environmental world and its modes of interacting are described [2,3]. Traditionally these observations are grouped as feeding, agonistic, social, reproductive, developmental and so on, using scientific method to objectify and analyse the behaviour under study. The observations are then used to generate hypotheses capable of further testing and extension to genetics and biochemistry. Ethological concepts have been extended to abnormal behaviour in animals, particularly companion animals, and these are often treated with drugs and behavioural techniques similar to those used in psychiatric medicine [4,5]. The central underlying supposition is an evolutionary one, usually selection for genetic survival [4,5].
For psychiatry, when adopting an ethological approach, some linking hypothesis between normal and abnormal behaviour is needed. We propose the following: that much psychiatric behaviour can be understood by using two categories: (i) normal evolved adaptive behaviour, which has become excessively prominent and (ii) a distortion of adaptive behaviours by some pathological process. To the extent that psychiatry is an eclectic discipline, there are likely to be syndromes, which are conceptualised poorly in this way or not at all. The test of the system proposed here would be whether it encompasses a useful proportion of those behaviours currently regarded as within the ambit of a psychiatrist.
Excessively prominent adaptive behaviours
Anxiety
Avoidance of noxious influences is widespread in most so-called higher animals: anxiety mobilises the physiological resources for withdrawal. The presence of fear allows the young to modulate the conflicting behaviours of exploration and protection. Fear of heights is almost ubiquitous [6]. It is seen in the young after becoming mobile but not before. Agitation of the infant after separation from the mother or carer, is similarly common across species [7,8]. It is probable that the neurological and neurochemical substrate of anxiety-like states is similar across a wide range of species, including humans [6]. Generally, the isolated mammal, including the human child, shows high levels of autonomic arousal, with similar behavioural consequences when anxious [6]. According to Marks [6] ‘the same four strategies of defensive behaviour – withdrawal, immobility, aggressive defense and deflection of attack are found in invertebrates and vertebrates. Also common across phyla are the basic forms of learning, such as habituation, sensitisation and classical and operant conditioning’. These strategies also occur in humans.
The deep mammalian structures related to fear are the limbic system, basal ganglia, hypothalamus, brain stem and the cerebellar nuclei. Mechanisms for escape and immobility have different but related circuits.
From a group aspect, a variety of strategies are adopted. These include huddling together, scattering of the group in different directions, panic behaviour, gross over-acting, startle and freeze responses. Each has its own ecological niche and survival value [9] but many are represented in human psychiatric states.
Other classical neuroses
Some depressive syndromes may occur secondarily to changes in social status. Price et al. [10] proposed that a depression-like syndrome occurred after loss of dominance. Jones et al. [11] demonstrated a similar response in the sugar glider (a small marsupial living in a tight social hierarchy) which may constitute a model for human depression. Price et al. [10] and later Daniels et al. [unpublished data] proposed on theoretical grounds that these observations can be used as a basis for an evolutionary approach to self-esteem, arguing that self-esteem may similarly have a biological basis with its counterpart in other species.
Immobility in animals, occurring under stress when more usual responses seem likely to fail, may form an evolutionary basis for various psychiatric states, including conversion disorders [Jones I and Blackshaw K, unpublished data]. Behaviours, at earlier times called ‘hysterical’, have been repeatedly split up into different entities within psychiatry. While the term ‘hysteria’ is not used in IDC-10 and DSM-IV, the clinical entities remain. ‘Hysterical paralysis’ may be understood in terms of stress-induced immobility [Jones I and Blackshaw K, unpublished data], obsessional neurosis has its counterparts in companion animals [4,5]. From the aspect of survival, obsessional behaviour may confer advantages, causing the organism to select the previously experienced (and successful) approach to a task when presented with a choice. The trait can be disadvantageous in a rapidly changing environment where more flexibility is needed. Intentional self-injury is common in vertebrates and may lead to death. There is evidence that this is relevant to human self-injury indicating a biological disposition, the behaviour emerging under similar social conditions [12]. Similarly, abnormal sexual behaviour may become more comprehensible when seen in an ethological context [13]. Close analogies exist between human and non-human exhibitionistic behaviours [13].
Distortion of adaptive behaviour by pathology
Close similarities exist between immobility responses and catatonic states, and between immobility responses and the motor disturbances seen in melancholia. An evolutionary explanation is that in these conditions evolved behaviour emerges in an enhanced form consequent upon some pathophysiology. This becomes clear in rare neurological syndromes such as akinetic mutism where pathology, sometimes demonstrable anatomically, can lead to a gross motor inhibition with mutism and what Benson has described as ‘a stubborn refusal to cooperate’ [14].
In drug-induced syndromes, although the proximate cause (using a sociobiological term) is the drug, the mode of response in the organism to that drug can be understood only by the role of transmitters in the behavioural ecology of humans and other species.
Personality
Variations in personality are not an exclusively human attribute; components such as obsessionality, attention seeking, dependence and aggressivity as pervading traits, have their counterparts in other animals. Human personality disorders may represent more widely held adaptive traits present to an excessive degree. Within a community, the presence of a range of genetically influenced behaviours is likely to increase the adaptive ability of that species, although not necessarily that of the individual should the environment change. The prominence of particular behaviours will vary between species in response to their particular needs.
Attention-seeking behaviour confers advantages in the chimpanzee [15], companion animals [4] and in humans. An infant's dependence on the mother is widespread, normal and adaptive, but abnormal dependence is found not only in humans but also in many companion animals [4,16]. Aggressivity, both contact and non-contact, occurs widely between species, assuming a pathological degree in a range of social circumstances [17] which can have close similarities between humans and other species.
Consciousness, affect, thought and volition
So far, attention has been given mostly to behaviour, yet psychiatry is primarily concerned with consciousness, feeling states, thought and volition. At first sight, these constitute the most serious barrier to an extension of animal studies to humans and hence to psychiatry. Cartesian philosophy makes a clear distinction between animal responses and human ones, regarding animal behaviour as reflex-like, however complex. In contrast, human behaviour is seen as willed: the consequence of choice and free will. This view has been a prevailing one in modern Western philosophy and has largely been accepted as axiomatic in psychiatry (unlike physical medicine). Treatment of those diseases shown to have a predominantly physical component has tended to pass from psychiatry to internal medicine, where the underlying theory is essentially mechanistic. Now this dichotomy is being questioned on two sides, the first by description of brain lesions that alter volition, and on the other hand, by demonstration of consciousness, affect and of a type of thought in animals [14,18].
Consciousness in animals in a general sense of awareness of the environment is difficult to dispute. Stimulus response as an exclusive paradigm fits very poorly into behaviour of higher animals, which show very subtle levels of choice. There is little doubt that mammals at least and probably many other organisms are aware of themselves, their environment, their relationships within it and the dangers that they currently encounter [18]. They respond appropriately to these perceptions, frequently in ways which have analogies if not homologies with human behaviour.
Chimpanzee, but not macaque monkeys can recognise themselves in a mirror indicating a very precise level of self-perception [19]. At a much wider level, marsupials, for example, have a clear idea of their own world and their rightful access to it depending on their position within the social group [10].
There is an undoubted similarity between the outward manifestations of feeling states (within the animal's behavioural repertoire) in humans and other animals, for example, apprehension, rage, fear and possibly more subtle emotions particularly in those domestic animals intimately observed by humans. Direct knowledge of whether the animal does actually have corresponding feelings is not susceptible to measurement, and indeed is restricted in humans too, except by the intervention and limitations of language. There are two ways of understanding feeling states in evolutionary terms: (i) they provide the motor which drives the organism to do those things that enhance the survival of its genes and (ii) they interpose a feeling state between stimulus and response, allowing the organism to pause in its response and then to mobilise effective resources or alternative strategies before responding [20,21].
Thought in humans is so highly developed that it far surpasses any used in other species but: ‘Nature has built the apparatus of rationality not just on top of biological regulations but from it and with it’ [22]. Each species is likely to have its own modes of perception so that the cognitive world of each will be different. We maintain that there will be themes held in common across species. For human psychodynamics based on evolution a new paradigm must be developed based on these evolutionary stable themes. Components of this paradigm may be:
Thought allows the organism to plan behavioural strategies in safety without performing them. This implies that much thought occurs in response to previously experienced or genetically determined behaviour patterns.
Thought has evolved in animals other than humans.
The structure of language may have a biological basis and by its structure be a further constraint on thought [23].
Behaviours adapted for hunter-gatherer existence may cease to be adaptive in our present environment.
The beginnings of an evolutionary psychotherapy based on these and related ideas have now been expanded at the World Psychiatric Association, XI World Congress of Psychiatry (Hamburg, 1999). The most highly developed psychotherapy is concerned with hierarchy and its pathologies.
We are not arguing that pure reason is impossible, although this has been argued from different premises [24]. Our evolutionary approach maintains that thought is continually influenced by dispositions of behaviour and is potentially subject to distortions of these dispositions by abnormal development or disease.
Abstract thought is not excluded in our paradigm nor is ethical or altruistic thinking. These abstract capacities that humans undoubtedly have, may represent a further stage in thought that can counter genetic influences. Humans' particular capacity for thought allows us to formulate these abstractions even though they may have arisen initially from genetic change. These ethical and altruistic thoughts could theoretically determine our behaviour entirely, but this is likely to be a fragile system since they must compete with powerful genetically determined behaviours.
The ideas expressed above are summarised in the following figure (Fig. 1) which shows an evolutionary approach to behaviour and its distortion in psychiatric states. This starts from a genetic disposition subsequently modified by learning. Affect, consciousness and volition, essential consideration in any extension of ethology to psychiatry, are incorporated in this model.
Conclusions
It is proposed that psychiatry can again take an aetiological approach to its area of study, but in doing so psychiatric syndromes may become reassembled from the existing classification to a different structure. The aetiology proposed here has an evolutionary basis and involves systematic use of animal behaviour concepts, quite unlike those currently used in contemporary psychiatry. Consciousness, feeling, thought and volition, we maintain, represent one further evolutionary step from behaviour, giving the organism greater flexibility to deal with the environment in a way which augments its chances of replicating its own genes. This approach, when applied to psychiatry, would bring us closer to other sciences and opens up new insights into psychiatric disorders.
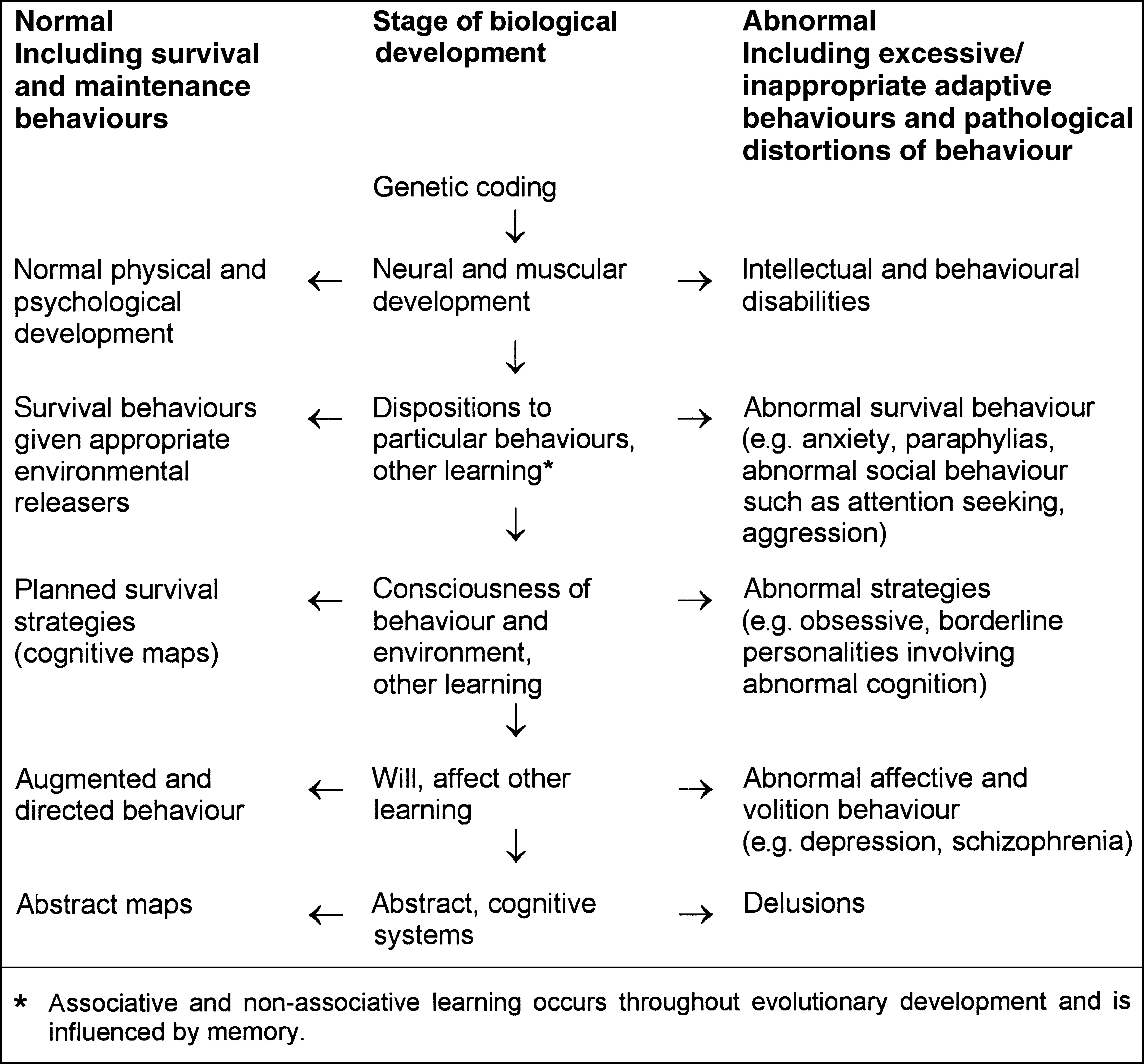
Evolutionary approach to behaviour, showing the normal and abnormal consequences that may follow increasingly complex biological development