
Abstract
Keywords
Pre-colonial health care in New Zealand, and the spiritual and communal beliefs upon which that mutual support system was founded, have been described by several authors [1–7]. Colonisation led to the rapid submergence of Maori health values in favour of Western practices [8]. Since the arrival of pakeha in New Zealand, the processes which Maori used to guide their lives and their society have been replaced [9]. Unlike the socially based Maori approach, the pakeha perspective focused on the individual and independence [10,11]. The pakeha approach to land and people focused on their economic importance rather than their spiritual or social value [11,12]. Health became the responsibility of the individual rather than a community concern [6]. Science, rather than spirituality, gave understanding to health [3]. Professionals trained in the Western ‘medical model’ [11] replaced tribal elders as leaders on health issues [6]. Non-pakeha philosophies on health care were perceived by pakeha as primitive and erroneous, and were severely condemned [1,11].
However, over the past two decades, as Maori participation in health provision has developed [5,13], various Maori perspectives of health have been advanced. The one which gained widest acceptance was a four-sided construct: whare tapa wha. The model compares health to the four walls of a house, all four being necessary to maintain strength, ensure shelter and give coherence [13]. It encompasses spiritual [5,11,14–18], mental [5,14,16], family [5,10,13,14,17], and physical [5,13] dimensions. These are referred to as te taha wairua, te taha hinengaro, te taha whanau and te taha tinana [18]. Durie [8] identified two further crucial foundations for mental health: land (whenua) [2,7,11] and language (te reo) [10,11].
Current problems and needs
Maori standards of mental health lag behind those of other New Zealanders [4]. In all settings where mental health professionals are employed, apart from tertiary education and private practice, Maori clients are substantially over-represented relative to their numbers in the general population [19,20]. Maori comprise up to 60% of those in psychiatric institutions [9,21] and up to 50% of those in the criminal justice system [9,22].
The mental health of Maori has changed considerably over the last 40 years [11]. Since 1962, Maori admissions to psychiatric institutions have increased dramatically [23]. Prior to 1960, non-Maori hospitalisation rates were higher than those for Maori. By 1974 the situation had reversed [6]. Maori re-admission rates are particularly high, indicating the ineffectiveness of treatments offered in ‘medical model’ institutions for Maori.
Given the disproportionately high numbers of Maori in poor mental health, and a steadily increasing suicide rate [6,24], the ability of mental health services to deal effectively with Maori clients has been the subject of considerable debate. Psychological tests normed on non-Maori clients has been the subject of considerable debate. Psychological tests normed on non-Maori populations or relying on Westernised content have been shown to disadvantage Maori clients [25]. Even community-based service innovations have been reported to import overseas models without consulting tangata whenua (indigenous people) [26]. The Committee of Inquiry into Procedures Used in Psychiatric Hospitals (1988) noted that staff were rarely educated in taha Maori (Maori culture) [27]. It was further suggested that many professional training programs created barriers to Maori entering the health professions (such as the lack of acknowledgement of Maori therapeutic paradigms and the absence of Maori staff in training programs). Brady [28] suggested that eliminating those barriers may encourage more applicants, but that significantly increasing the number of Maori professionals would take some years. She recommended changes both in services and in the training of professionals.
In 1987 Abbott and Durie surveyed the heads of all tertiary professional courses in health-related disciplines to determine whether students received adequate preparation to work effectively with Maori clients. Although respondents demonstrated good intentions, the overall findings were disappointing in terms of curriculum content, Maori student intake and presence of Maori staff [4,19].
It is widely accepted that members of one culture are likely to be less effective when dealing with members of another culture, especially if they lack an understanding of that culture [10]. Aware of these problems, the Standing Committee on Maori Health issued guidelines to help faculties integrate a bicultural focus [29]. These included the following. 1. Maori health issues can only be addressed by the involvement of a greater number of Maori people in the delivery of health care and the setting of priorities. 2. For Maori people, the health teams should have the support of the Maori community, and must include both Western trained health professionals and people trained in Maori schools of learning. 3. Training programs should reflect the bicultural nature of New Zealand society. If teaching institutions are unable to adequately prepare people, they should contract out to those organisations equipped to do so.
Despite various attempts to reverse the position of Maori there are still disproportionate numbers of Maori coming into contact with mental health professionals [21,28] who are largely ignorant of Maori mental health perspectives [30]. It has often been argued that bicultural education for practising mental health professionals should be energetically pursued [21,31], but an uneven response has been received from the mental health community [28].
A 1990 survey by Sawrey [31] highlighted the monocultural nature of institutional psychological services in New Zealand. Responses from 163 hospital psychologists and clinical psychologists working in the Justice Department indicated that although over 85% agreed that knowledge of taha Maori was important in determining good psychotherapeutic outcomes with Maori clients, over 75% felt they had an inadequate knowledge of taha Maori. Furthermore, 88% felt that their training had not equipped them to work effectively with Maori clients.
No such survey has been conducted with psychiatrists. The present study attempts to fill this research gap by determining whether psychiatrists feel that their knowledge and training in taha Maori has prepared them adequately for effective work with Maori clients. A simultaneous survey of New Zealand psychologists [Johnstone, 1998, unpublished data] allowed comparisons between the two professions.
Method
Participants
The questionnaires and a covering letter were mailed by the Royal Australian and New Zealand College of Psychiatrists (RANZCP) to all 335 New Zealand based psychiatrists on its membership list.
Questionnaire
The questionnaire was piloted on four Maori mental health workers and a manager of a mental health unit. The questionnaire was also sent to the RANZCP for comment on how it might be rendered most useful to its members. Two questions required rewording; one was leading and another double-barrelled.
Section One contained 14 statements, 10 replicated from Sawrey's survey [31] and five developed from Maori mental health literature. Five-point Likert scales were used to measure the degree of agreement with the statements, followed with space for comments. Section Two consisted of three open-ended questions: ‘What sort of training do you think you need to work effectively with Maori clients?’, ‘Why do you think Maori are over-represented in psychiatric hospitals?’ and ‘If you were the Minister of Health, what two recommendations would you make to improve mental health services for Maori?’. Participants were also asked ‘How much time during training should be devoted to taha Maori (Maori culture)?’.
Analysis
Analysis of the quantitative data (Likert scales) involved two-tailed t-tests for comparison with the mean responses of 445 psychologists surveyed simultaneously. A thematic content analysis [32,33] was used in analysis of the qualitative data. The primary researcher (KJ) read the participants' answers and searched for themes. Responses to the three open-ended questions were also independently categorised by another individual, with no previous involvement in the study. Inter-rater reliability (the number of individual categorisations agreed as a proportion of the total number of categorisations) was 90%. Where there were discrepancies, categorisations were reassessed to achieve consistency.
Results
Sample characteristics
The survey was completed by 247 of the 335 psychiatrists (73.7%). The demographic characteristics of the participants are presented in Table 1. Responses to the items about Maori mental health and related training issues are presented in Table 2.
Demographic characteristics of psychiatrists interviewed
Percentage of total number of psychiatrists interviewed (247).
Percentages of 247 psychiatrists who agree or disagree with 14 statements and mean scores compared with those of 445 psychologists
Difference between mean scores of psychiatrists and psychologists:
p < 0.05,
p < 0.01,
p < 0.001,
p < 0.0001 (two-tailed Student's t-test). A, agree; D, disagree; SA, strongly agree; SD, strongly disagree; U, unsure.
1 = strongly agree, 5 = strongly disagree.
Training and knowledge
Approximately half the participants (51.4%) believed they had adequate knowledge of taha Maori (Maori culture) to work effectively with Maori, with 30.0% believing this was not the case. However, considerably less than half (40.1%) believed their training had prepared them to work effectively with Maori. This discrepancy was partially explained by a multivariate analysis of variance which showed that older participants (p < 0.0001) and those with more Maori clients (p < 0.0001) were more likely to feel that they had adequate knowledge of taha Maori. This finding that inadequate training has since been compensated for was illustrated by comments such as:
Training programs provide a basic knowledge which needs to be developed through additional training, like Maori language courses and cultural safety courses.
Land and Language
Most psychiatrists (75.7%) agreed that ‘Maori language is very important in terms of mental health’ with only 17 (6.9%), all men, disagreeing. A similar majority (72.9%) agreed that ‘The loss of land is a strong factor influencing mental health’. However 41 (16.6%) disagreed. Women agreed more than men both on the language and land issues (p < 0.01). Some of the comments suggested a certain lack of understanding among some male psychiatrists:
Loss of land may traditionally have been a problem for Maori – but not now. If it was, why would the tribes be selling their land to the government?
Very few urban Maori, or even others, tell me they have experienced a loss of land.
I have yet to see a Maori patient present with problems as a result of loss of land.
Holism and spirituality
Nearly all psychiatrists agreed with the statements about the importance of spirituality (99.2%) and of considering ‘the whole person’ (95.5%). Comments included:
I agree with this statement, even though my training in the medical model ignores the holistic approach.
and
How can we work holistically? We can't work spiritually, that's a job for a witchdoctor.
Treaty of Waitangi
Psychiatrists were more divided about whether ‘The Treaty of Waitangi should be the basis for the provision of health services for Maori’. While 131 (53.0%) agreed, 75 (30.4%) disagreed and 41 (16.6%) were ‘unsure’. Comments varied:
The Treaty equals partnership. Services should accommodate the needs of Maori and pakeha.
The Treaty of Waitangi is a bit like the Bible – an important historical document that cannot be used as a blueprint for life today.
Need should be the basis for provision of health services, not a bloody 150-year-old document.
Consultation
Most psychiatrists (70.4%) agreed that ‘When working with a Maori client, one should liaise with a Maori consultant/kaumatua,’ with 28 (11.3%) disagreeing and 45 (18.2%) unsure. Again, comments varied:
As there are not enough Maori workers to have only Maori work with Maori, we need to consult.
and
We don't need to consult with Maori just because our client is Maori, otherwise if we have Asians do we have to consult with Asian workers, if our client was homosexual do we have to consult with our homosexual colleagues, where would it stop?
The use of European clinicians and diagnostic systems
None of the 247 psychiatrists agreed with the statement ‘European/pakeha clinicians should not work with Maori clients’ and only 6 (2.4%) were unsure. The remaining 241 (97.6%) disagreed, 114 (46.2%) strongly. Only two (0.8%) agreed that ‘European diagnostic systems should not be used with Maori’, five (2.0%) were unsure and 240 (97.2%) disagreed, 103 (41.7%) strongly. Comments on these two statements included:
Alcohol dependence, substance abuse, anxiety and depression are not biased against culture, these disorders have no cultural barriers.
We can work with Maori as effectively as Maori work with Maori. At least I am a qualified psychiatrist – not a life-experience qualified Maori.
What a racist statement! I mean, just because you have a white face doesn't mean you can only work with other white faces.
Anyone can work with Maori clients. I mean, if they are that picky they can go to Maori-run services.
Psychiatrists' recommendations
Training
Responses to ‘What sort of training do you think you need to work effectively with Maori clients?’ are listed, with examples, in Table 3. Training about Maori perspectives of health (78.5%) and the Treaty of Waitangi (63.6%) were most frequently recommended.
The areas of training which psychiatrists interviewed think they need to work effectively with Maori clients
Percentage of total number of psychiatrists interviewed (247).
Improving mental health services for Maori
Participants were asked what two recommendations they would make, if they were the Minister of Health, to improve services for Maori. Their responses are presented, with examples, in Table 4. The most common recommendations were for more Maori mental health professionals (76.1%) and Maori psychiatrists (49.0%), more mental health funding in general (63.2%) and Maori-run services (44.1%).
The recommendations psychiatrists interviewed would make to improve mental health services for Maori, if they were the Minister of Health
Percentage of total number of psychiatrists interviewed (247).
Over-representation of Maori in psychiatric institutions
Participants were asked why they thought Maori were over represented in psychiatric institutions. Their responses are presented in Table 5. Most (86%) cited socioeconomic status. High drug or alcohol use was cited by 42%.
Interviewed psychiatrists' beliefs about why Maori are over-represented in psychiatric institutions
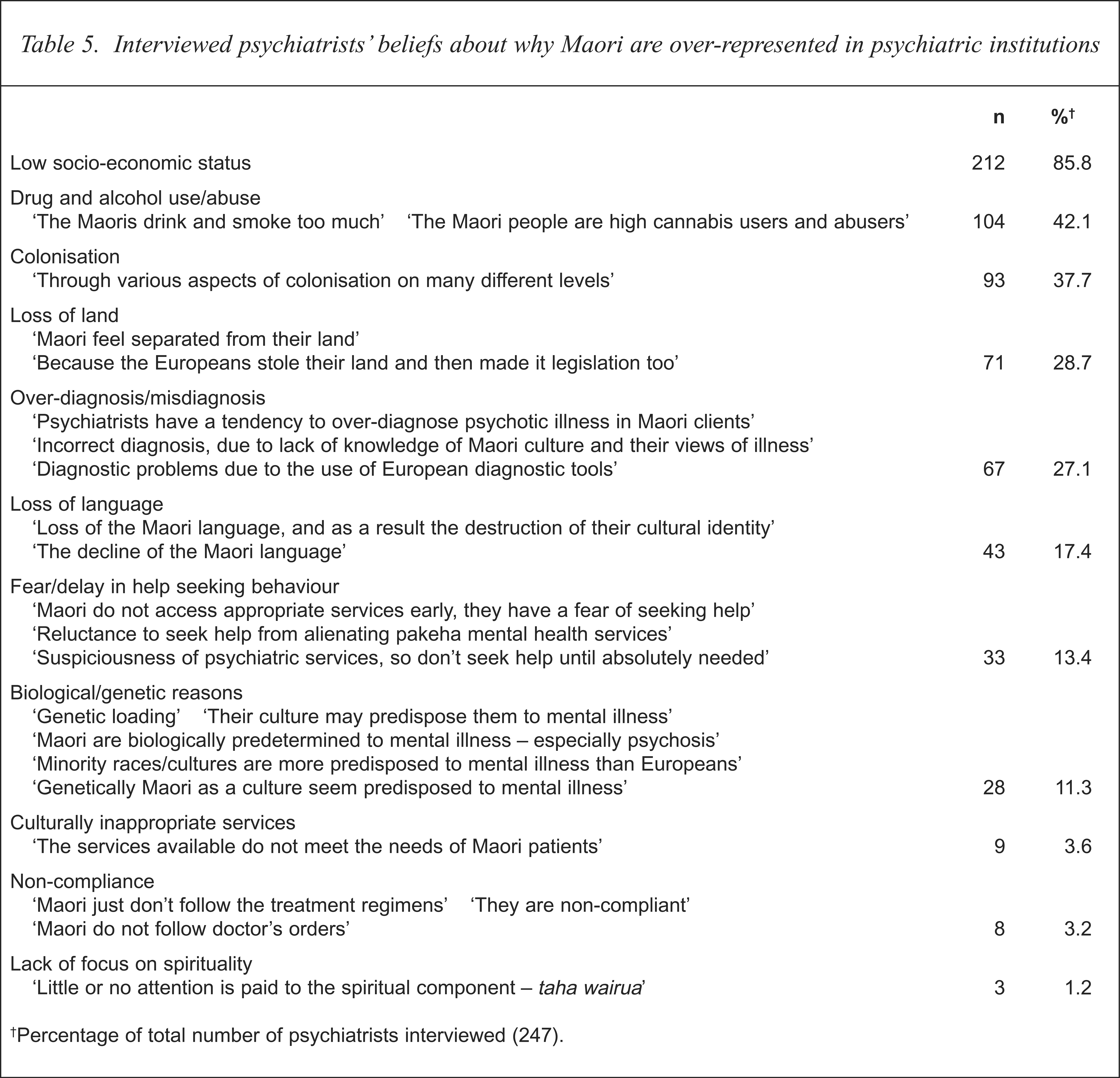
Percentage of total number of psychiatrists interviewed (247).
Twenty-eight psychiatrists (11.3%), all male, believed that Maori were over represented because they were more biologically or genetically predisposed to mental illness than were Europeans. One psychologist (0.2%), also male, shared this belief.
Additional comments
Some additional comments are presented in the hope that they may be of value to those responsible for training and monitoring standards within the profession:
I don't think of my clients in terms of their culture.
All people are the same.
The way I work with patients does not depend on the colour of their skin or their ethnicity.
As a European I take offence to your study, why should I learn about taha Maori and not other cultures – New Zealand is no longer bicultural it is now multicultural. Given all the cultures within New Zealand, I would find this very time consuming and tedious.
To run separate Maori-run services only encourages separatism. We are all New Zealanders.
The similarities between all human beings are far more important than any difference. Focusing on differences is the root of prejudice and provides the rationale for unjust and even sadistic prejudices.
I am sick of questionnaires regarding Maori stuff, there is far more important issues than those regarding Maori mental health. Do you really think that psychiatrists need to have an understanding of such concepts like spirituality – come on give me a break.
There is no need for taha Maori in training programs, as psychiatrists we are taught skills and we apply them in a cookbook manner. My effectiveness as a psychiatrist is not dependent on the colour of my skin, my culture, nor my understanding of bloody Maori culture.
I think your study is a waste of time. Why do people like you single out the Maoris for topics of research – what makes them so special?
I wish Masters students would stop sending me crap studies like this, about pointless, meaningless, cultural rubbish. They (Maori) only represent about 10 per cent of the population, for God's sake.
This questionnaire is worthless! I mean the Maoris are always going on about the importance of land etc. etc. so why did they bloody well give it away. They went on about the importance of forestries and lakes and then that bloody idiot cut down the tree on One Tree Hill. I feel that they are getting the appropriate services they need, just not using them, medication is the answer – but they just don't take their pills – if cannabis was prescribed, I'd bet they'd bloody take that.
Discussion
The data summarised above are based on a 73.7% response rate of the 335 New Zealand members of the RANZCP. Although a minority may have responded in order to express their antipathy to the topic, such a response rate seems to represent a high level of interest in the issues. Most psychiatrists were willing, when asked, to make thoughtful and positive recommendations about how to improve their training and services for Maori. This suggests an encouraging level of awareness that change is needed.
It is hoped that their recommendations (already disseminated to the RANZCP and under discussion therein), will be of assistance to those responsible for training psychiatrists and those managing mental health services. The true value of this study can ultimately only be determined by the willingness of the individual members of the profession, and the profession's leadership, to act on their own recommendations. Follow-up studies, conducted with awareness of process issues related to researching Maori issues [34], might include a survey of Maori consumers.
Racist beliefs in nearly one in five male psychiatrists
Alongside the many positive contributions of the majority of participants it is of concern that 11.3% of New Zealand's psychiatrists believed that Maori were over-represented in psychiatric institutions because they were genetically more predisposed than others to become ‘mentally ill’. The participants expressing this view were all male and all identified as European. Thus nearly one in five male psychiatrists (28 out of 151, 18.5%) expressed this view. All 28 were born in New Zealand and all had 10 or more years of clinical experience. Thus nearly one-third of New Zealand born male psychiatrists (28 out of 86, 32.6%) and well over half of New Zealand born male psychiatrists with 10 or more years experience (28 out of 46, 60.9%) believed that Maori were more biologically or genetically predisposed to ‘madness’ than others. That such a simplistic and unsubstantiated application of the biological paradigm is held by a significant proportion of psychiatrists is a matter of grave concern. Is the belief that a particular race is more genetically predisposed to ‘madness’ than other races any less racist than the belief that a race is genetically/biologically inferior?
This alarming finding, in combination with some of the more ignorant comments cited earlier, raises questions about the effectiveness of procedures for selection into professional training programs to screen out applicants with overtly racist attitudes.
To take a more positive perspective, it is worth noting that no psychiatrist with less than 10 years clinical experience (i.e. no recent graduates) shared this belief in genetic inferiority.
A recent survey [35] found that 96% of Australian and New Zealand psychiatrists believe ‘senior psychiatrists have wisdom to offer to junior colleagues’ but that ‘increased “respect and tolerance” of patients as a benefit of experience was more likely to be reported by respondendents who were more experienced’. Our findings suggest that on bicultural issues less senior psychiatrists may have something to offer their more senior colleagues.
Differences between psychiatrists and psychologists
The differences in opinions between the professions may be a result of their training. Psychiatrists' training may not cover social, economic and cultural causal factors as much as psychology training programs. An example of how aetiological beliefs can influence attitudes is the finding that those espousing biological beliefs about the aetiology of mental health problems are less likely than those with a psycho-social perspective to welcome consumer participation in planning and managing services [36].
Psychiatrists were more satisfied with the bicultural component of their training (mean agreement 3.2) than psychologists (3.7) (p < 0.0001). This discrepancy may be explained by different levels of expectation about what should be offered during training. The mean response of psychiatrists to ‘How much time during training should be devoted to taha Maori?’ was 4.2%; whereas the psychologists' mean was 10.7% (p < 0.0001).
Details of the psychologists' responses are available [37].
Conclusions
There are clear implications arising from this study for the training and practice of mental health professionals in New Zealand, and for the provision of effective mental health services for Maori. This study confirms that there is a need for more than a tokenistic inclusion of Maori values in professional training programs. The rationale for a Maori component within training programs comes from Maori/non-Maori disparities in mental health standards, as well as the Treaty of Waitangi, which laid the foundation for a partnership between Maori tribes and the State [6,38]. There is also practical motivation for trying to understand a group of people who constitute a significant part of the professionals' client group [39]. There are still training programs that take an ‘add on approach’ [40] thereby fooling ourselves that learning a bit of te reo (Maori language) and a few waiata is sufficient [41].
There is clearly some way to go before Maori mental health professionals approximate the ratio of Maori in the wider community, and before the majority of graduates are able to relate comfortably and competently to Maori clients. There is a continuing need for mental health professionals to recognise that as tangata whenua Maori people have the right to be culturally different from the majority [3,28,42–44].
Brady (1992) stated that, while Maori are striving for cultural parity generally, within mental health services and professional training programs there is a longstanding need for a health perspective which reflects and encompasses Maori culture and values [28]. The results of this study confirm Brady's view that it is time to accept a bicultural component and look realistically at the processes and structures of professional training programs and to refashion these programs collaboratively with Maori to meet the needs of Maori and pakeha students for the benefit of all prospective clients. While Maori mental health stands to benefit from appropriate institutional responses to Maori mental health needs, Durie [45] added that a Maori contribution has positive implications for the mental health of the nation as a whole and for the standard of practice of all mental health professionals.
It is hoped that the time taken by the 247 psychiatrists to complete the questionnaire, and their invaluable and varied recommendations, will be of assistance to the increasing number of people trying, in various ways, to improve mental health services for Maori.