
Abstract
Semantic memory is consistently found to be compromised in patients with schizophrenia [1–4]. The verbal fluency task plays a significant role in the study of semantic memory. It requires subjects to name as many words as possible beginning with a specified letter (to test for letter or formal fluency) or exemplars in a defined category (to test for categorical or semantic fluency) in a limited period of time. During the verbal fluency task, subjects initiate self-directed searches in the inner lexicon to retrieve the appropriate words [5]. Thus it involves two fundamental neurocognitive processes including retrieval process and semantic store. Verbal fluency performance impairment has been consistently reported in patients with schizophrenia [6–8]. The reduction of fluency output can be due to impairment of either one or both processes. Previous studies emphasised only the impairment of retrieval process without any assessment of the semantic store [9,10]. Allen et al. [11] directly examined the semantic store by estimating the lexicon size from the degree of overlap of the word output from repeated verbal fluency tests. They showed that patients with schizophrenia have normal lexicon size but impairment in retrieval process. This impairment correlated with negative schizophrenic symptoms. However, they did not report the effect of medication and illness duration on verbal fluency performance. Previous longitudinal studies [12–14] demonstrated evidence for neurocognitive deterioration in the course of schizophrenic illness, while others support a static course [15]. It is probable that some patients with chronic schizophrenia have impairment in verbal intelligence especially after a long duration of illness. Thus, we sought to replicate Allen et al.'s study in a sample of Chinese patients with chronic schizophrenia.
Method
Subjects
Twenty-one patients satisfying the DSM-III-R criteria for chronic schizophrenia [16], aged 18–65, were recruited from a regional mental hospital (Kwai Chung Hospital) in Hong Kong. Based on the screening of case notes, which showed no acute exacerbation of illness, and on the fact that medication doses in the preceding 3 months had been constant, these patients were rated as stable. Patients with mental retardation, neurological disease, severe physical illness affecting the central nervous system, a history of head injury resulting in loss of consciousness or a history of substance abuse and those who had received recent electroconvulsive therapy were excluded. Eleven control subjects were recruited from hospital staff. They were screened by one of the authors (RYLC) using a questionnaire that asked about demographic information, severe physical illnesses affecting the central nervous system, family history of mental illness and psychopathology of psychosis, mood and substance related disorder. Control subjects were not on any medication on the days of assessments. All subjects gave informed consent and the study was approved by the local ethics committee.
Assessment of clinical symptoms
The clinical status of the patients was assessed using the 18-item brief psychiatric rating scale (BPRS) [17] and High Royds evaluation of negativity (HEN) scale [18]. Depressive symptomatology was assessed by the Montgomery and Asberg depression rating scale (MADRS) [19]. These clinical instruments have been validated for, and used in, Hong Kong patients (for BPRS see [20]; for HEN see [21]). The dosages of antipsychotic medication were converted to daily chlorpromazine equivalent [22]. Daily anticholinergic dosages were recorded in milligrams.
Assessment of verbal fluency performance
Semantic verbal fluency tests for three categories (‘food’, ‘animal’ and ‘transport’) were performed in accordance with the procedure developed by Allen et al. [11]. The test was conducted in Cantonese, which is the first language of all the subjects. Three minutes were allowed for each subject to give as many words as possible of a specified category in each trial. Each subject was assessed on three separate sessions of verbal fluency. The interval between each session was 1 week. During each session, three consecutive trials of the same category were performed, followed by each of the other two categories. Thus there were five trials in each session for each subject. For the subsequent session 1 week later, three consecutive trials were performed for another category which had not previously been tested consecutively followed by each of the remaining two categories. The presentation of categories to subjects were both verbal and by means of cards with the specified category written on them. The output of words was audiotaped for subsequent analysis. Four variables of word output were recorded: (i) the numbers of words in each trial of 3 min duration; (ii) variable words: words that appeared in only one of the five trials; (iii) shared words: words that appeared in all of the five trials; (iv) inappropriate words: words that are not in the specified category.
Calculation of lexicon size
Lexicon size was calculated as the total number of words available to the subject unconstrained by retrieval time and assessed by repeated verbal fluency tasks in accordance with the mathematical model of Allen et al. [11]. In each trial, a subject gave some new words which had not been produced before. When the number of trials increased, these new words were reduced. Eventually, the subject's vocabulary would be exhausted without further production of new word. At this point, the total number of various words the subject had generated became the estimated lexicon size. In calculation, the data from the five repetitions of verbal fluency task was expressed as the reciprocals of the number of new words plotted against the reciprocals of the trial number to form a good approximation to a straight line. The parameter of this line was then estimated using standard regression procedure.
Statistical analysis
The data were analysed by analysis of variance (ANOVA) with repeated measures. The correlation between clinical symptoms and the verbal fluency variables, including number of words in each trial, shared words, variable words, and lexicon size, was determined using Pearson's product moment correlation. Inappropriate words, because of their score distribution, were analysed by non-parametric test.
Results
Demographic information
The patient group consisted of 11 male and 10 female subjects with a mean age of 42.3 years (SD = 11.9) and mean education of 8.1 years (SD = 3.7). The control group consisted of 4 male and 7 female subjects with a mean age of 43.5 years (SD = 8.4) and mean education of 7.2 years (SD = 4.3). There was no statistically significant difference between patient and control group in terms of age (df = 1, 30, F = 0.084, p = 0.775), sex (df = 1, χ2 = 0.744, p = 0.388) and years of education (df = 1, 30, F = 0.398, p = 0.533).
Clinical profile
The patients had an average illness duration of 17.1 years (SD = 8.1). The mean BPRS global score, HEN scale summary score and MADRS total score was 26.7 (SD = 5.9), 11.6 (SD = 3.3) and 2.7 (SD = 3.2) respectively. All patients were taking antipsychotic medication with the average daily dosage in chlorpromazine equivalent 1639 mg (SD = 1701). Twelve patients were on an anti-parkinsonian drug (benzhexol), the mean daily dose of which was 5.7 mg (SD = 3.4).
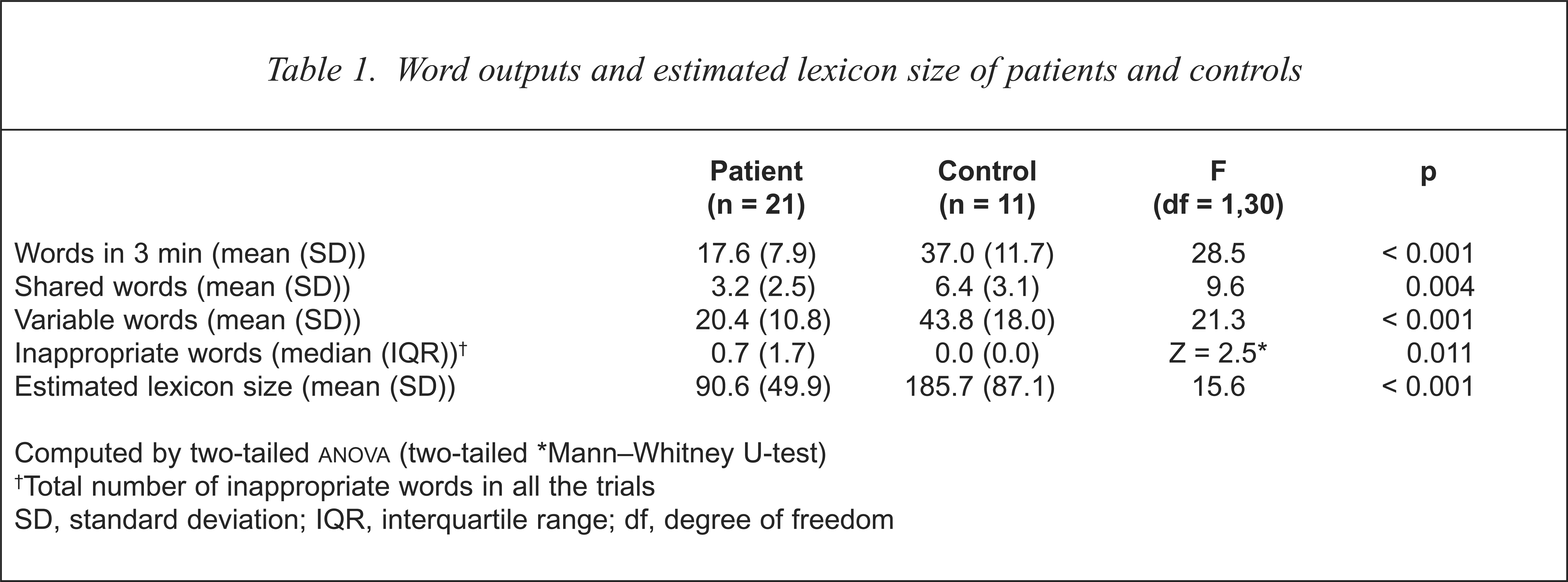
Word outputs and estimated lexicon size
The data of the verbal fluency performance from the three categories were combined for computation. The results of various word outputs and the estimation of the lexicon size of the subjects are shown in Table 1. The patients generated significantly fewer shared and variable words in 3 min, but more inappropriate words than controls.
Word outputs and estimated lexicon size of patients and controls
Computed by two-tailed
Mann–Whitney U-test)
Total number of inappropriate words in all the trials
SD, standard deviation; IQR, interquartile range; df, degree of freedom
Relation with demographic profile and clinical symptoms
There was a correlation between education and lexicon size in controls (r = 0.66, p = 0.027), but not in patients (r = 0.43, p = 0.052). Male and female subjects did not differ in verbal fluency performance. No significant correlation was noted with age.
In a previous study on 204 patients with chronic schizophrenia, we found BPRS consisting of five symptom factors (positive, negative, affective, anxiety and disorganisation symptoms)[23]. Verbal fluency variables (total output, lexicon size and inappropriate words) were correlated with illness duration, dosage of medication and clinical symptoms (the five factors from BPRS, global ratings of sub-scales and summary score from HEN scale and MADRS global score). No significant correlation was found between the verbal fluency variables and the clinical profile. Results remained the same after controlling for the potential confounding factors as education, age, and illness duration.
The relationship between clinical symptoms and verbal fluency performance was further explored by dividing the patients into two groups according to the presence or absence of inappropriate words, positive, negative and disorganisation symptoms from BPRS. No significant difference was found between the two groups.
Categories, trials and interval between trials effect
There were significant differences among the three word categories (df = 2, 29, F = 32.7, p < 0.001) with increasing numbers of items generated from ‘transport’, ‘animal’ and ‘food’ respectively by both patients and controls. Patients generated 13 words (SD = 6.3) in ‘transport’, 17 words (SD = 7.8) in ‘animal’ and 22 words (SD = 11.7) in ‘food’; while controls produced 27 words (SD = 8.4) in ‘transport’, 36 words (SD = 13.7) in ‘animal’ and 47 words (SD = 16.2) in ‘food’. Difference across categories were noted between the two groups (df = 2, 29, F = 3.8, p = 0.034). There was no significant difference in word generation among the five trials (df = 4, 27, F = 2.3, p = 0.081) and the two intervals between trials (df = 1, 30, F = 0.1, p = 0.739). There was no interaction with other factors.
Discussion
We attempted to replicate Allen et al.'s study [11] in a sample of patients with chronic schizophrenia in Hong Kong. In contrast to the original study, we found that in addition to having a lower semantic verbal fluency output, the patients also had a reduced lexicon size. This finding suggests that at least for some patients, there is evidence for semantic store reduction. Allen et al. did not report the illness duration of their patients. Our patients had a higher mean age (42 years) than those in the Allen et al. study (35 years). This probably also reflects longer illness duration in our sample. The course of neurocognitive deficit in schizophrenia is still controversial. In early longitudinal studies, progression of neurocognitive impairment was reported, but these studies were conducted before the implementation of standardised diagnostic criteria for schizophrenia [12–14]. Recent longitudinal studies did not find any significant neurocognitive decline throughout the follow-up periods [15]. Since the results of these recent studies were limited by their relatively short follow-up period, the possibility remains that in a subgroup of patients with chronic schizophrenia, significant cognitive deterioration may occur. In contrast to previous findings [11,24], we did not find any correlation between negative symptoms and verbal fluency in our sample. This may be due to the fact that our sample consisted of more chronic patients and most of them had marked negative symptoms.
Previous studies tended to emphasise the impairment of retrieval process in verbal fluency, but could not totally exclude the possibility of store reduction in patients with schizophrenia. In regard to the assessment of retrieval process, Robert et al. studied the clustering of related words generated from a semantic verbal fluency task [10]. They defined semantic cluster as the consecutive association of words belonging to a given subcategory (e.g. ‘hen’, ‘rooster’, ‘goose’ as ‘farm animal’; ‘fly’, ‘cockroach’, ‘black beetle’ as ‘insects’). Patients with schizophrenia were found to have a significantly smaller number of words produced in the 2 min verbal fluency task and also a smaller number of semantic cluster than did controls. Robert et al. claimed that patients were inefficient in retrieval process during the verbal fluency task. However, it can be argued that the number of closely related words and the number of cluster headings may be reduced in parallel with semantic store impairment in patients. There was no assessment of the semantic store to control for this.
Another method to study retrieval processes is to provide cues of semantic dimensions to the subjects during verbal fluency tasks. Joyce et al. compared schizophrenic patients with healthy controls for verbal fluency performance, with and without semantic cues (e.g. ‘animals’ found ‘on a farm’, ‘in a house’ and ‘in the jungle’) [9]. They showed that impaired performance of categorical verbal fluency in patients with schizophrenia could be improved by the cueing method. They claimed this result as evidence for a retrieval processing deficit. According to their findings, both patients and controls had significant improvement in cued condition, but the interaction effect between groups (patients and controls) and conditions (cued and uncued) did not reach statistical significance. There was only a trend showing a direction of superior response to cueing in the patient group. Therefore their results could only argue that both patients and controls can benefit from cueing in the verbal fluency task. Since the magnitude of improvement in patients when using semantic cues may not have totally accounted for the deficit in verbal fluency performance, the possibility of lower semantic store could not be totally excluded. Furthermore, Joyce et al. administered the Boston naming test [25] and found that patients had significantly poorer performance compared with controls on all conditions including uncued, semantic cueing and phonemic cueing. Since the Boston naming test is less dependent on retrieval processes than on the semantic verbal fluency task, it can better assess the semantic store directly, especially after cueing methods. Thus, the results from Joyce et al. may be consistent with a fundamental impairment of semantic store. The correlation of the Boston naming test with uncued verbal fluency only occurred in normal subjects but not in patients. This may support retrieval process impairment but cannot totally exclude the underlying semantic store reduction.
Frith et al. [26], drawing from the results of their positron emission tomography (PET) study, postulated that the semantic store was located in the temporal lobe, and the pre-frontal cortex was essential for searching for appropriate exemplars from the semantic store. Our results may allow speculation that in some patients with chronic schizophrenia, semantic store impairment may be associated with temporal lobe dysfunction. Martin et al. used an interference task during categorical and lexical verbal fluency to show that temporal lobe function was more important than frontal lobe function in semantic verbal fluency as compared to lexical verbal fluency [27]. The generation of words in response to a specified semantic category requires more demands from temporal lobe-mediated semantic knowledge than frontal lobe-mediated strategic search. Thus in an impairment of semantic verbal fluency, semantic store reduction can be a more significant factor than the strategic search inefficiency. This is further supported by Troster et al.'s study on patients with temporal lobe epilepsy who generated similar numbers of shifts between categories, but a lower ratio of exemplars to category label than normal controls [28]. This implied normal retrieval process but semantic store reduction. There have been numerous reports on the temporal lobe pathology from postmortem and neuroimaging studies in patients with schizophrenia (reviewed by Roberts [29]). All these findings may lend support to the relationship between semantic store and temporal lobe dysfunction in schizophrenia.
Conclusions
We found that verbal fluency impairment in patients with schizophrenia is at least partly related to semantic store reduction. This relationship is compatible with current neuropsychological and neuroimaging results. The importance of temporal lobe involvement in semantic verbal fluency deficit needs to be emphasised as an integral part of the neurobiological basis of schizophrenia research.