
Abstract
Research into the effects of mental illness occurring during the postpartum period is increasingly assuming a dyadic perspective where the infant, as well as the unwell mother, is a focus of investigation [1,2]. It is now recognised that maternal mental illness may have a number of potentially deleterious effects on infant development [3,4] and a number of mechanisms of association, including direct impact of maternal symptomatology, have been proposed [5]. This study aims to investigate the influence that a schizophrenic illness may have on the interactions a mother has with her infant. Both positive and negative symptoms of schizophrenia may potentially disturb the quality of these interactions. Our interest in the area arose from a realisation that it is generally an improvement in maternal mental state and an ability to demonstrate safe infant-care practices which determines discharge from hospital when a mother with a mental illness and her baby are admitted to a psychiatric Mother-Baby Unit. The quality of the mother-infant relationship does not appear to influence such decision making unless there are concerns that the infant may be abused or neglected. It is often assumed that resolution of maternal symptoms of mental illness results in normalisation of mother-infant interactions. We have been unable to find any literature which supports this assumption. Much of our existing knowledge regarding maternal mental illness and its effects on mother-infant interaction relates to mothers suffering from postpartum depressive states [4,6]. There is a paucity of studies which have examined this relationship when the mother suffers from a schizophrenic illness.
It is reasonable to suspect that a mother suffering from a postpartum schizophrenic illness may be unable to provide an optimal nurturing and responsive environment for her infant. An infant may be exposed to excesses such as hallucinations, perplexity of affect, delusions, bizarre or disorganised behaviour, or the deficits of blunted emotions, poverty or distortions of speech, avolition and anhedonia. The quality of mother-infant interactions may be significantly influenced by such symptoms; in particular, there may be a lack of synchronous and contingent behaviours which are considered to be essential for the early unfolding of attachment [7]. The relevance of the quality of such interactions to child development is increasingly being understood: maternal schizophrenic illness potentially disturbs the quality of parenting behaviours [8,10], there are a number of potential deleterious effects on infant development secondary to maternal schizophrenic illness such as emotional, behavioural, social, sensorimotor and cognitive impairment [11,14], and there are a number of pathways to such outcomes and disturbance of mother-infant interaction has been hypothesised to be one significant factor [15].
The relationship between manifest schizophrenic symptomatology and potential relational deficits in parenting has received little attention in the literature. Much attention has been paid to the incorporation of a baby into delusional thinking and the potential risks this may entail for the baby such as neglect, abuse and infanticide [16]. The infant may be regarded as a source of persecution or as a potential victim subject to the same malevolent forces as the mother. Blurring of ego boundaries may result in distortion of the ability of a mother to distinguish self from infant. There may even be a delusional failure to recognise the very existence of the child [17]. Occasionally, terrorising attacks on children occur as a consequence [18]. When the onset of psychosis coincides with childbirth there may be a greater risk of a mother attributing the origins of her illness to her baby [2]. In our experience involvement of the infant in a mother's delusional system is relatively rare, and the infant is more likely to be protected from imagined persecutors than be considered the source of malevolence. Often a psychotic mother's relationship with her infant appears ‘encapsulated’ in that its quality is relatively preserved when contrasted to the disintegration of other familial and external affiliations.
Psychotic symptoms may affect the relationship between mother and infant through a number of mechanisms: through involvement of the child in hallucinations, delusions or passivity experiences, by rendering the mother unavailable to her baby when her symptoms demand preferential attention, through behavioural disorganisation, and through abnormal expressions of emotion. Whereas positive symptoms potentially disrupt the mother-infant relationship and adaption to motherhood through presence of unwanted behaviours, negative symptoms tend to exert their influence through absence of desirable behaviours. This may result in the provision of an impoverished maternal and social environment to which the infant is exposed. Psychotropic medications may also result in maternal sedation or restriction of physical means of emotive expression through their side effects.
This clinical problem is best illustrated by a case vignette: ‘Jane’, was a 28-year-old married woman who was admitted together with her 2-month-old baby daughter to our Mother-Baby Unit with an acute relapse of paranoid schizophrenia. Her presentation was characterised by affective perplexity, auditory hallucinations, persecutory delusions, passivity phenomenon, disorganised thinking, and behavioural disturbance. This was her fourth hospitalisation since being diagnosed with the disorder 3 years previously. Although her psychotic symptoms remitted with treatment she displayed marked psychosocial decline. She had been forced to resign from full-time employment as a receptionist, had become isolated and withdrawn socially, and her husband described her as having lost her organisational abilities and self-confidence. Her pregnancy had been planned, and the couple's fantasy was that a child would revive Jane's lost sense of purpose and direction. Delivery was uncomplicated and she successfully established breastfeeding, which she enjoyed.
On admission, Jane was observed during a play session with her baby. She was asked to spend time with her baby as she normally would, but was reluctant to participate in the play session and placed her baby on the floor in front of her. She gazed silently at her baby and her face revealed perplexity and acute discomfort. Anxiously, Jane touched her baby and immediately withdrew. Later, when she briefly held her baby in her arms, there was no moulding of bodies and the posture adopted appeared both awkward and uncomfortable. The baby was held in a manner which did not allow eye contact with her mother. Jane showed no realisation that her baby's grunts and tearful protestations indicated discomfort. There was no attempt on Jane's part to either soothe or stimulate her baby: nearby toys remained untouched. She remained silent apart from occasional inappropriate giggles. The baby was then handed over to nursing staff and Jane went outside for a cigarette.
There was a distinct atmosphere of detachment and discomfort. Jane was hesitant and uncertain in all of her movements. While the baby was clear in her cues, her mother was unable to respond in an appropriate or comforting manner. Physical and emotional distance characterised the interaction between mother and baby. There was a distinct lack of maternal responsiveness or dyadic reciprocity.
At discharge, another play session was observed. Jane's psychotic symptoms had remitted with treatment; however, negative symptoms of inattention, anhedonia, avolition and apathy persisted. Jane immediately placed her baby, who was now 4 months old, on the floor. The baby introduced herself to nearby toys rather than have them presented to her. She made them rattle and appeared to gain much pleasure from this exercise. This was demonstrated through gurgles and smiles. Jane also appeared to derive pleasure from her baby's antics, but made minimal effort to enhance her baby's enjoyment through participation or reciprocal action. Jane spoke to her baby affectionately and laughed frequently. However, she often laughed independently, rather than in synchrony with her baby's expressions of excitement. Although Jane attended to her baby, she tended to be distracted by peripheral unrelated events and noises. The pair made eye contact when the baby was held in her arms, but this was never sustained for a prolonged period. The repertoire of play was markedly restricted. The interaction lacked intensity and we felt we were watching a mother watching her baby.
At discharge, Jane was free of psychotic symptoms but demonstrated a number of deficit features of schizophrenia. Her mothering practices were assessed to be safe and she had been able to display competency in basic mothercraft skills. However, the quality and nature of mother-infant interactions were considered to be suboptimal. While there were no concerns of exposure to hostility or abuse, the baby was considered to be developmentally at risk.
This study was designed to examine the relationship between the mental state of women with a post-partum schizophrenic illness and the quality of mother-infant interactions by collecting descriptive data that measure these variables at two distinct time intervals (admission and discharge from hospital), which traditionally represent a clinical impression of change, and to examine more specifically whether a change in the mental state of these women is related to a change in the quality of their interactions with their baby.
Method
The study sample consisted of women suffering from a schizophrenic illness during their first post-partum year and their infants, who had been hospitalised in the Austin and Repatriation Medical Centre Mother-Baby Unit. The women consisted of both voluntary and involuntary patients admitted for treatment of their illness and/or impairment of their maternal care-taking abilities. Inclusion criteria consisted of: maternal diagnosis satisfying the DSM-IV [19] criteria for schizophrenia, schizophreniform disorder or brief psychotic disorder, adequate command of English, and infant age less than 1 year. Mothers were excluded from the study if they met diagnostic criteria for schizoaffective disorder or a comorbid affective disorder or substance abuse disorder. Diagnoses recorded represented the clinical opinion of the first and seconds authors. Ethics Committee approval was granted for this study and informed consent was obtained from all participants.
The study population consisted of three types of mothers: those with a schizophrenic illness originating postpartum, those with a postpartum relapse of a pre-existing schizophrenic illness, and those with a chronic schizophrenic illness complicating the postpartum period. Of the 18 mother-infant dyads eligible for the study three were excluded: two were not willing to give informed consent and one did not speak English.
Measures
Two main areas were examined: maternal psychopathology and quality of mother-infant interactions. The rating scales employed during the study were: the Positive and Negative Syndrome Scale (PANSS) [20], the Infant/Caregiver Behavioural Scale [Milgrom J: unpublished manuscript, 1996], and the Bethlem Mother-Infant Interaction Scale [21]. Inter-rater reliability was not established as all observations on a particular scale were made by the same examiner and comparisons were not made with other sources of data utilising these instruments. Intra-rater reliability was established prior to the commencement of the study via repeated measures of video-taped material.
The PANSS consists of seven-point ratings on 30 symptoms and signs for which each item and level of severity are defined. The ratings provide summary scores on positive scale, negative scale, general psychopathology scale, and a composite index. Factor scores are also obtained by summing statistically related items: anergia, thought disturbance, activation, paranoid-belligerence, and depression.
The Infant/Caregiver Behavioural Scale consists of 18 behavioural measures comprising seven maternal measures: response, stimulation/arousal, caregiving, positive affect, negative affect, attention, soothe/comfort; eight infant measures: infant clarity of cues, exploration, smile/excite, fuss/cry, attention to other children, attention to caregiver, aggression, alertness; and three joint mother-infant measures: mutual attention, reciprocity/synchronicity, intensity of interaction. Each measure is rated on a 0-2-point scale after observing a 3-min segment of mother-infant behaviour (0 = occurs zero to 30% of the time, 1 = occurs between 30% and 60% of the time, and 2 = occurs more than 60% of the time). Repeated ratings on each measure were obtained by observing six consecutive 3-min behaviour segments during the one play session. The procedure commenced with the mother being asked to play with her baby as she normally would in a setting secure from intrusion and the observer sat silently at a distance so as to avoid being part of the play interaction. Observation for the purpose of recording began once dialogue with the observer had ceased and the mother-infant dyad were demonstrably comfortable with the procedure.
The Bethlem Mother-Infant Interaction Scale is a nurse rated scale which measures seven variables: eye contact, physical contact, vocal contact, mood, general routine, risk to baby and baby's condition. The overall impression of mother-infant interactions over the past week are rated on a four-point scale. If 1 day varies significantly from another, the ‘worst day’ during the past week is rated. The scale measures global aspects of the mother's contribution to the dialogue with her baby, her capacity to organise and maintain routine care, staff perception of risk to the infant, and the infant's contribution to the interaction. It was designed as a validated measure of mother-infant adjustment in Mother-Baby Units [21] and has recently been demonstrated to be a reliable and valid instrument in the Australian setting [22].
Procedure
Subjects were rated on two occasions: within 1 week of admission, and again once a decision had been made that the mother-infant dyad were ready for discharge from the unit. The PANSS was administered following a semistructured interview which was conducted according to the appropriate guidelines. The Infant/Caregiver Behavioural Scale was completed during the observation of an unstructured play session. The Bethlem Mother-Infant Observation Scale was rated by a registered psychiatric nurse experienced in the use of the scale utilising knowledge gained from all observations of the mother-infant dyad made in the preceding week. Also recorded were psychiatric diagnosis, mother's age, infant's age and gender, mother's marital status, time of onset of symptoms, whether a relapse of a pre-existing illness, state of infant's physical health, method of feeding, admission status (voluntary/involuntary), duration of admission, whether mother and infant remained together after discharge, and involvement of Child Protective Services.
Statistical analysis
As the data was recorded on ordinal (ranked) scales, and the sample size precluded an assumption of normal distribution, non-parametric statistical methods were employed to test the following hypotheses: that the severity of psychopathology in mothers with a postpartum schizophrenic illness correlated negatively with the quality of mother-infant interactions, and that a change in the severity of psychopathology in mothers with a postpartum schizophrenic illness correlated with a corresponding change in the quality of mother-infant interactions.
The PANSS summary and factor scores, and the scores for mother-infant interaction variables, were examined utilising the Wilcoxon rank sum test to establish if there was a statistically significant change between admission and discharge. Spearman's rank correlation coefficients were calculated to determine the association between these variables at both admission and discharge, and for change in association between admission and discharge.
Results
Sample description
Fifteen mother-infant dyads were examined in the study. On admission, the mean maternal age was 28.6 years (SD = 6.0, range = 21–39). The mean infant age, which also represents the number of post-partum weeks at the time of admission, was 16.9 weeks (SD = 15.7, range = 1–44). Seven of the infants were female. Fifty-three percent of the mothers were single, 27% were married and 20% were involved in de facto relationships. Eighty percent of the pregnancies were unplanned and 33% of the mothers were breastfeeding at the time of admission.
Protective Services were involved in 40% of the cases; however, 87% of the dyads were discharged together. Two mothers lost custody of their infant: one elected to place her daughter in long-term foster care, and the other was transferred to a more secure facility as her disturbed behaviour could not be handled safely in the unit. The average length of stay for the group was 29.6 days (SD = 21.4, range = 5–70). Four mothers were experiencing their first episode of psychosis (one with brief psychotic disorder and three with schizophreniform disorder), three were experiencing a postpartum relapse of schizophrenia, and eight suffered from chronic schizophrenia. Consideration was given to whether the four mothers who experienced their first onset of psychosis could better be considered to have been suffering from a puerperal psychosis which is commonly considered to represent an affective disorder which is not currently part of DSM-IV [19] nosology. However, given the nature of manifest symptomatology and premorbid features, it was decided that these women would be best considered to be suffering from an illness conceptualised as belonging to the spectrum of schizophrenic disorders.
Illness symptomatology and severity
Examination of PANSS scores revealed that the mothers were heterogenous in terms of symptom nature and severity. There was a moderate degree of variability in both syndrome and cluster scores at both admission and discharge. All but two of the mothers experienced a significant decrease in positive syndrome scores during the course of their admission. The two mothers who deteriorated saw their infants placed into foster care. In all cases but one, there was little change in negative syndrome scores. The mother who had the greatest change in negative symptom score also had the longest admission (70 days).
Examination of the differences between admission and discharge PANSS scores revealed a statistically significant improvement for the positive and general psychopathology syndrome scores, and the thought disorder and activation factor scores (Wilcoxon Z corrected for ties < − 2.32, p < 0.05). The least significant change occurred with the negative syndrome and anergia factor scores.
Mother-infant interaction
The heterogenous nature of the sample was again demonstrated by the large variation between scores on both scales for admission interaction variables. There was a marked reduction in this variability at discharge where the sample was much more homogenous.
Examination of the difference between admission and discharge scores for mother-infant interaction variables revealed a statistically significant improvement for all Bethlem Mother-Infant Interaction Scale variables other than Baby Care (Wilcoxon Z corrected for ties < − 2.86, p < 0.01). In contrast, of the Infant/Caregiver Behavioural Scale variables only the infant variables of exploration, smile/excite, and alertness variables, and the dyadic mutual attention variable showed statistically significant improvement (Wilcoxon Z corrected for ties < − 2.28, p < 0.05). All mothers, other than the two whose mental states deteriorated during the course of admission, showed statistically significant improvement for the remaining dyadic interactional variables, and a number of other maternal variables.
Relationship between the severity of symptoms with the quality of mother-infant interactions
Unless otherwise stated all correlations reported below achieved statistical significance (Spearman's rho corrected for ties < − 0.5, p < 0.05). On admission, the greater the disturbance of maternal mental state in terms of positive schizophrenic symptoms (in particular thought disorder) and general psychopathology, the more likely it was that worse scores measuring quality of mother-infant interaction would be recorded. Such interaction was more likely to consist of maternal unresponsiveness, understimulation, inattention, a lack of expressed positive affect (both physical and verbal), expressions of hostility, disorganised parenting routine, and dyadic lack of mutual attention, reciprocity and synchronicity, and intensity of interaction. At discharge a different correlational pattern emerged. The more prominent the mother's negative schizophrenic symptoms (in particular the anergic aspects), the more likely it was that worse scores measuring quality of mother-infant interaction would be recorded. Such interaction was more likely to consist of maternal unresponsiveness, inattention, disorganised parenting routine, minimal arousal, a lack of expression of positive affect and a dyadic lack of mutual attention. Hostile interactions were more likely to occur when the mother remained psychotic (in particular thought disordered, highly activated and paranoid or belligerent). At neither admission nor discharge did the variables measuring infant contribution to the mother-infant interaction correlate significantly with scores which rated maternal psychopathology.
Relationship between the change in severity of symptoms with the change in quality of mother-infant interactions
An improvement in the quality of the maternal and dyadic contribution to the mother-infant interaction was most likely to be associated with an improvement in maternal mental state in terms of positive schizophrenic symptoms and general psychopathology. Such improvement was more likely to consist of an improvement in maternal responsiveness, infant stimulation, expression of positive affect, attentiveness, organisation of parenting routine, and a reduction in expressed hostility. Dyadic mutual attention, reciprocity and synchronicity, and interaction intensity were also more likely to improve. An improvement in the quality of mother-infant interaction was most likely to be associated with an improvement in thought disorder, activation, and paranoid/belligerence factor scores, rather than a change in PANSS negative syndrome, anergia and depression factor scores.
Figures 1 and 2 demonstrate the relationship between change in the maternal contribution to mother-infant interaction and change in the PANSS syndrome scores for individual mothers.
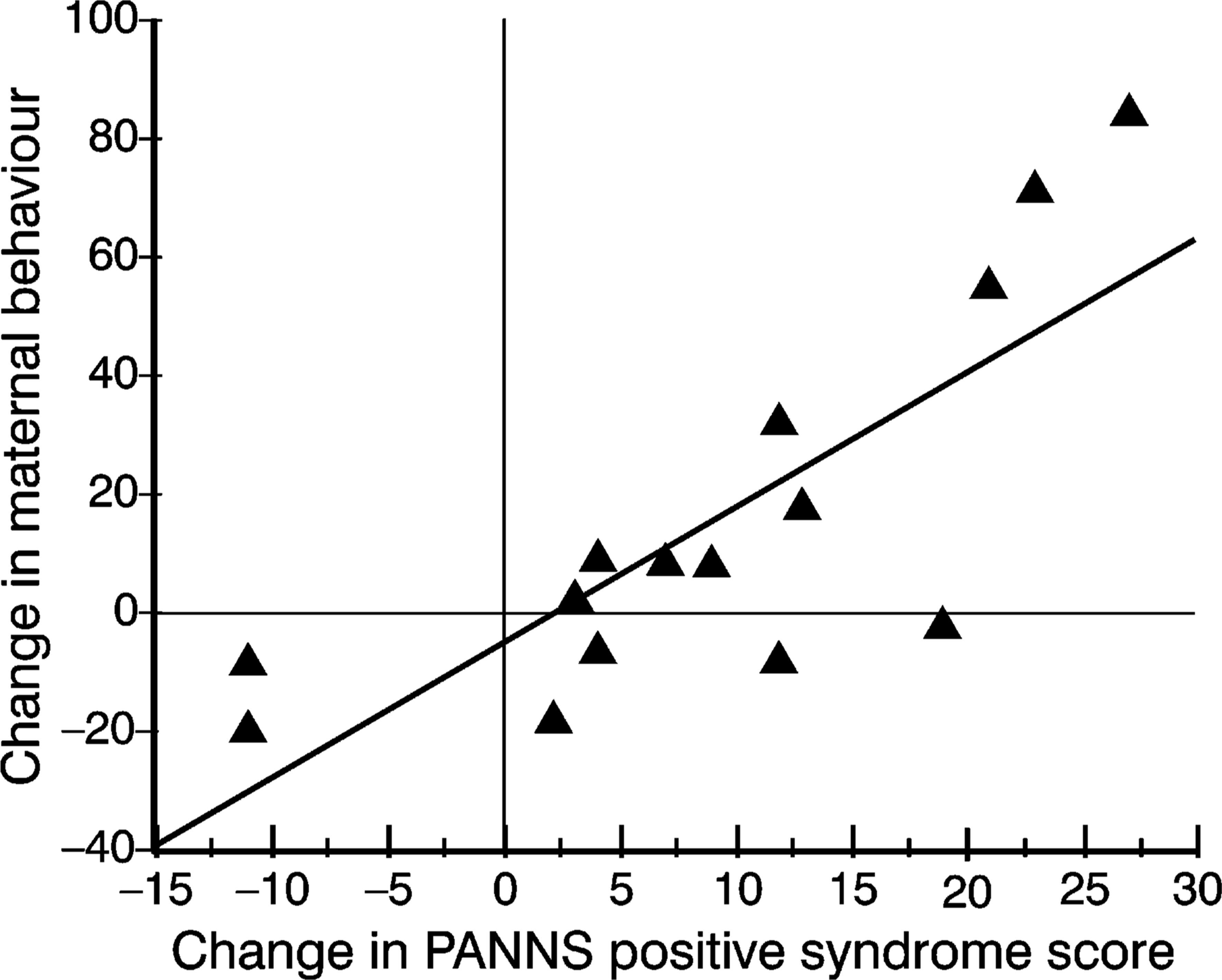
Relationship between Positive and Negative Syndrome Scale (PANSS) positive syndrome scores and maternal contribution to mother-infant interaction (r2 = 0.626).
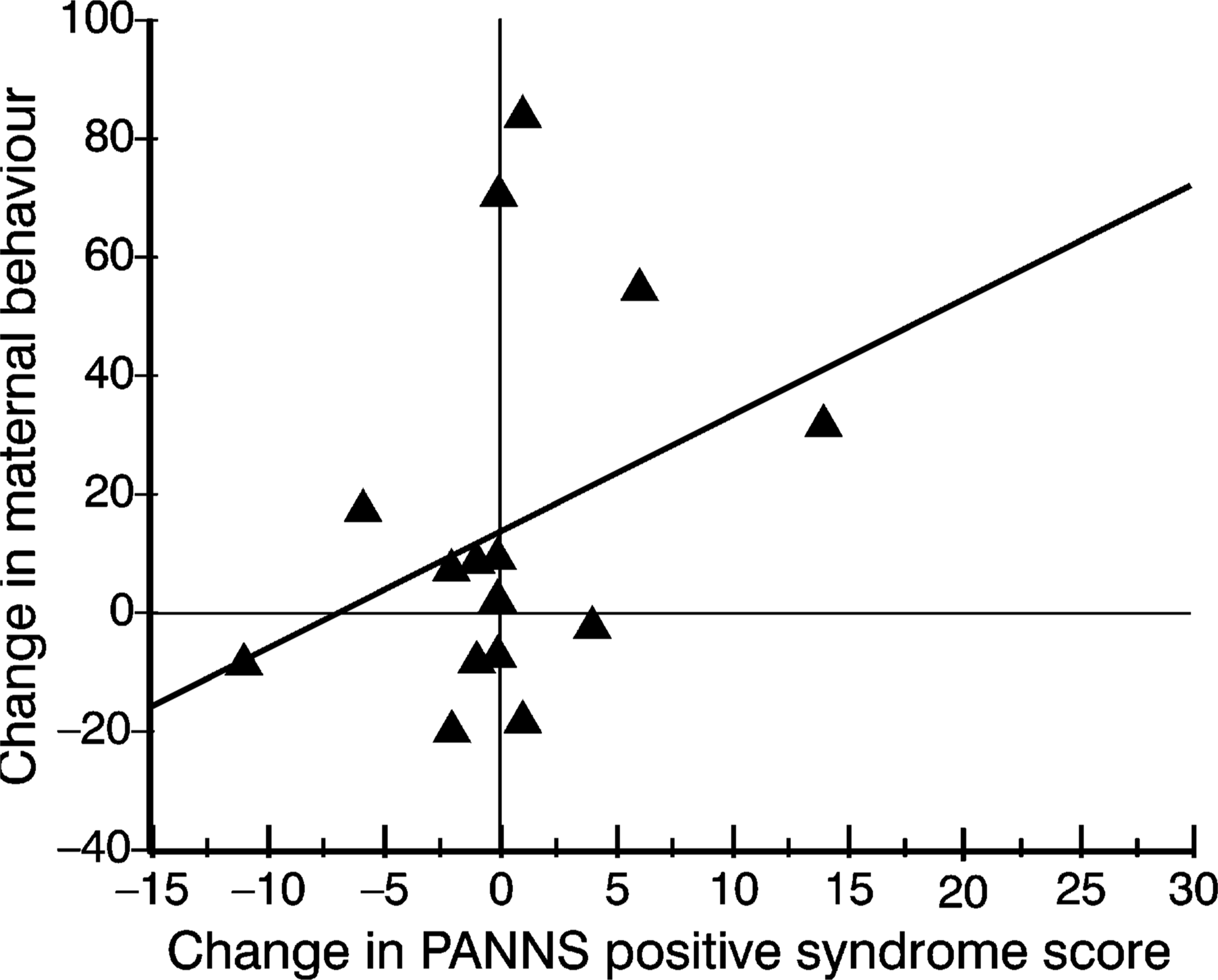
Relationship between Positive and Negative Syndrome Scale (PANSS) negative syndrome scores and maternal contribution to mother-infant interaction (r2 = 0.075).
Discussion
It was not surprising to find that during the period of hospitalisation there was a significant decline in the mothers' positive symptoms, and minimal change in negative symptoms. While positive symptoms generally respond well to treatment, the deficit features of schizophrenia are much less amenable and slower to change. The sample, although small, demonstrated the heterogenous nature of schizophrenia in that patients varied in terms of manifest symptomatology, illness severity, chronicity, and prominence of deficit features. The finding that more than half of the mothers were single parents, and that the majority had not planned their pregnancies was not unexpected given that psychosocial decline and difficulty maintaining intimate relationships are often associated with schizophrenic illness. It was not surprising to find that Protective Services were involved in a significant number of cases as the children of mothers with schizophrenia are generally considered to be at risk. However, the fact that the majority of mothers retained custody of their infants after discharge contrasts significantly with the findings of Kumar et al. [23], who found that 50% of their mothers with schizophrenia were discharged without their babies. This finding was encouraging as it highlights the need for specialist Mother-Baby Units which avail mothers with schizophrenia of their services.
The hypothesis that the severity of psychopathology in mothers with a postpartum schizophrenic illness correlates with the quality of mother-infant interactions was supported by the study findings. Of greatest interest is the different correlational patterns found on admission and at discharge.
On admission, mothers with the greatest positive symptoms had worse interactions with their infants. Such interaction was more likely to consist of maternal unavailability in terms of unresponsiveness, understimulation, inattention, and limited expression of positive affect. The infant was also more likely to be exposed to expressions of hostility and disorganised parenting. The mother-infant dyad were also more likely to have less intense interactions which lacked mutual attention and synchronicity. At discharge, however, the mothers with more prominent negative symptoms, in particular the anergic aspects, had worse interactions with their infants. These mothers were similarly inattentive, unresponsive, understimulating and disorganised. While positive affective expression was more likely to be lacking, hostility was more likely to be present if the mother had persistent positive symptoms.
These findings support the research literature on maternal schizophrenia and mother-infant interaction. What this study is able to add is demonstration of an association between the severity of mental state disturbance of a mother with schizophrenia and the degree of impairment of the quality of mother-infant interactions. While the study design does not allow conclusions regarding causality to be made, it is interesting to note that the strongest correlations between disturbance of mother-infant interaction and schizophrenic symptomatology were with thought disorder on admission and anergia at discharge. The relevance of this observation is that thought disorder was also shown to respond well to treatment, while the anergic aspects of schizophrenia were more treatment resistant.
It is interesting to note that on admission an association between severity of negative symptoms and the extent of disturbance of the quality of mother-infant interactions was not demonstrated, while it was at discharge; even though negative symptoms were also demonstrated to show no significant change during the period of admission. We propose that the influence of negative symptoms upon the quality of mother-infant interaction is concealed by the presence of positive symptoms and that in clinical practice re-assessment of both sets of symptoms should occur at discharge and not only on admission.
It is relevant to consider that for any meaningful exchange to occur between mother and infant maternal responsiveness and dyadic mutual attention are prerequisite. Without this a ‘dialogue’ cannot begin. Impairment of both of these interactional variables has been shown to be associated with the severity of disturbance of mental state in mothers with schizophrenia. It can be hypothesised that a floridly psychotic mother may not be appropriately available to her infant as her inner experiences demand preferential attention. Even when a mother is relieved of such symptoms she is more likely to remain unavailable to her infant if deficit features persist. It can also be hypothesised that negative symptoms impair a mother's relational capacity through limiting her motivation and ability to attend to others, her range of emotional experience and expression, and her capacity to experience pleasure. These symptoms may impair such ‘dialogue’ through limiting both the interactive repertoire and the emotional behaviours required to both stimulate and engage an infant.
Of interest, at neither admission nor discharge did the variables measuring infant contribution to the mother-infant interaction correlate significantly with scores which rated maternal psychopathology. This finding is difficult to interpret as there are a number of possible explanations and normative data for infants of well mothers was not available. It may support the notion that infants are able to accommodate maternal schizophrenic illness without any initial deleterious effect. While infant behaviour may appear adaptive within the given context it may be maladaptive developmentally and within other contexts which would not have been detected given the study methodology. There may be a delay between changes in maternal mental state and effects on infant behaviour which the study was unable to detect due to the timing of observations. This finding may also vary with infant age and their stage of social development. The enriched environment of the hospital ward may have been a protective factor. It is also worth noting that scales used to measure parent-infant interaction do not necessarily represent an indication of infant mental health. Furthermore, had the research methodology been designed to measure variables such as attachment, infant temperament, and other aspects of infant mental health another picture may have emerged.
The study further demonstrated that an improvement in maternal psychotic symptomatology was associated with an improvement in the quality of mother-infant interaction. However, the study results highlight the need for ongoing intervention after discharge from hospital when the mother suffers from prominent deficit features of her schizophrenic illness. This research identifies infants of schizophrenic mothers with prominent deficit features to be at risk as they will potentially be exposed to ongoing suboptimal interactions with their mothers.
Several factors limit the ability to generalise these findings. The small sample size and the large number of variables measured exposes the study to type I and type H errors. Selection bias was operational as only those mother-infant dyads admitted to a Mother-Baby Unit were studied. Excluded were the least and most severe ends of the schizophrenic illness spectrum (i.e. mothers well enough to be managed in the community, and mothers too disturbed to be managed in an open ward setting). The study lacked a control group and therefore inferences regarding causality cannot be made. Given the study design patients in effect acted as their own controls.
The rating scales used and the observational techniques employed have their own limitations. While the PANSS proved simple to use and was sensitive to change, its use has not been validated in postpartum populations, nor have the mother-infant interaction scales; however, there is no reason to suspect that they would not prove to be valid instruments in this context. The degree of subjectivity required to score the scales rating mother-infant interaction potentially introduced observer bias.
While the mother-infant interaction procedures were relatively unintrusive a number of demand characteristics need to be considered. Potentially, a mother may have performed worse than usual in the play session if she felt paranoid or anxious. Conversely, her performance may have been enhanced by a belief that results would be used to determine aspects of her management such as discharge planning or reports to Protective Services. A better than usual performance may also have been encouraged by the demand characteristic of focusing on one defined goal: playing with her infant. Our impression was that mothers were comfortable with the observational procedure and this was encouraged by the simplicity of the instructions given prior to the play session.
Another group of confounding factors are those which relate to the assumptions underlying the study: that an observed unstructured play session is a good measure of the quality of mother-infant interactions more generally, and that behaviours observed in the ward setting are typical for the dyad and are representative of interactions which occur in more naturalistic settings.
Children of mothers with schizophrenia have been identified to be at risk of abnormal development and later psychopathology. Heredity can only account for part of this increased risk. While this study is unable to contribute to a clarification as to which environmental factors are important aetiologically in increasing this risk, it has been able to provide preliminary data which identifies quality of mother-infant interaction as a variable which changes with the nature and severity of maternal schizophrenic disturbance. If the quality of mother-infant interaction contributes significantly to infant outcome then this finding has a number of significant clinical implications. First, primary prevention needs to be a priority given that many women with schizophrenia do not plan their pregnancies. Contraception and family planning issues should be addressed with any woman with schizophrenia of child-bearing age. Second, assessment of mental state and psychosocial functioning of a mother with schizophrenia should always include joint assessment of mother and infant, in particular the nature and quality of their interactions, at both admission and discharge from hospital. Third, the greatest effort needs to be directed towards early detection of those mothers with schizophrenia who are likely to have the most disturbed interactions with their infants (i.e. those with florid positive symptoms and those with prominent negative symptoms). While the former group tend to present early for treatment, the latter group often do not present or are lost to follow up. Thus, without assertive outreach programs staffed by clinicians who also have the skills to identify such maternal pathology and associated disturbances of mother-infant interaction an opportunity for intervention is lost. Finally, this research highlights the need for ongoing therapeutic intervention postdis-charge which focuses on not only the mother, but also the mother-infant dyad.
Many Mother-Baby Units are unable to offer continuing care after discharge and exist solely as an inpatient service. Presently many community based psychiatric services do not possess the skills or expertise required to intervene meaningfully when a mother with schizophrenia displays disturbed interaction with her infant. In our experience, family services and other early parenting outreach programs which could assist such mothers and infants rarely exist in an integrated form with psychiatric services, and links between separate services are poorly developed [24]. Development of such integrated services is particularly relevant given recent changes to mental health and child protection legislation which demand that care be offered in the least restrictive environment possible. An integrated service would also need to be positioned to address non-illness-related factors not investigated in this study which are likely to influence maternal and infant outcome such as comorbidity, dysfunction within other familial relationships, and socioeconomic disadvantage.
In summary, mothers with florid psychotic symptoms and prominent negative symptoms of schizophrenia and their infants have been identified as being at particular risk of displaying disturbed interaction. The adverse contribution of negative symptoms is often not evident until after the psychotic symptoms have resolved. Given that negative symptoms are treatment resistant, optimal clinical care of mothers with schizophrenia and their infants needs to involve ongoing therapeutic intervention which specifically addresses disturbances of mother-infant interaction. Further research is required to identify which interventions are likely to be of greatest benefit.
Footnotes
Acknowledgements
We wish to thank Jeanette Milgrom for allowing us to use the rating scale she developed which measures components of mother-infant interaction, Wynne Stamboulakis for assisting with data collection, and the staff of the Austin and Repatriation Medical Centre Mother-Baby Unit for their assistance and support.