
Abstract
Schizophrenia and other psychotic illnesses most commonly first emerge in late adolescence/early adulthood [1]. These illnesses often bear high costs for the affected individual as well as for their family and the wider community [2] and the development of preventative strategies towards psychosis has been a long-standing and desirable goal [3,3,4,5].
Mrazek and Haggerty [6] wrote ‘the best hope now for the prevention of schizophrenia lies with indicated preventative interventions targeted at individuals manifesting precursor signs and symptoms who have not yet met full criteria for diagnosis. The identification of individuals at this early stage coupled with the introduction of pharmacological and psychological interventions, may prevent the development of the full-blown disorder’ (p. 154). Thus, providing appropriate preventative interventions to individuals describing signs of emerging disorder, such as attenuated or low grade psychotic symptoms, or a strong family history of psychotic disorder, in conjunction with a marked decrease in functioning may prevent further deterioration [7,8].
For indicated prevention of psychosis to be achievable, three important factors are noted. First, criteria that accurately identify individuals with a high rate of transition to psychosis must be developed. Second, individuals meeting those criteria must be recruited by the service providing the preventative interventions. Finally, and obviously, the preventative interventions that are developed must be effective in preventing psychosis in the short and long-term.
The first of these components has been the focus of previous research by our group. Forty-one percent of young people meeting specific criteria developed a psychotic illness within 12 months of initial referral [11]. It was concluded, therefore, that these criteria identify young people at greatly increased risk of developing a psychotic disorder than the general population. Another study is currently in progress assessing interventions developed specifically for this high-risk population. The current descriptive paper examines the ‘pathway to care’ of young people meeting the ‘high-risk’ criteria who are referred to a clinical service catering specifically for this target group.
Access to care: first-episode psychosis
Numerous studies have reported that delays in treatment of first-episode psychosis extend, on average, from one to 2 years [12,13,14]. Duration of untreated psychosis may be attributed to delayed initiation of help-seeking, the lack of recognition of problematic symptoms by either client, family or healthcare workers consulted, or the failure of primary care providers to refer to appropriate services [15]. Thus, a circuitous route is often taken to find appropriate treatment for the first-episode population. An average of 3 or 4.5 service contact have been made by first episode patients prior to appropriate treatment being commenced according to two studies [16,17]
Implications for the high risk group
The ‘pathway to care’ of high-risk patients might be similar to that described for first-episode patients, protracted and often involving many steps. The subtle and infrequent nature of psychotic symptoms as experienced by the high risk group, in conjunction with the general reluctance of young people to seek health care is likely to hinder help seeking by young people at high risk of developing a psychotic disorder.
Young people describing signs of potentially emerging psychosis but not full-blown disorder might also sometimes be overlooked by mental health services. The current survey was based in Victoria, Australia, where people describing attenuated psychotic symptoms would not normally be eligible for treatment within mainstream psychiatric services, particularly adult services, despite moves by many services towards preventative and early intervention foci. Mainstream psychiatric services are largely structured to treat those diagnosed with a ‘serious mental illness’ according to DSM or ICD criteria [18]. Young people reporting low-grade psychotic symptoms may receive treatment by a primary health practitioner or within the private health system, but this has not been assessed.
This paper describes the pattern of referral to a mental health clinic targeting young people at high risk of psychosis over 20 months of operation. Implications for the structure of the service and strategies for attracting young people at high risk of psychosis to treatment are discussed.
Setting
The PACE (Personal Assessment and Crisis Evaluation) Clinic is a specialised clinical/research service for young people thought to be at high risk of developing a psychotic episode. The program was established in Melbourne, Australia in 1994. Research at PACE addresses the issue of identifying predictors of psychosis in young people [9], as well as the development of appropriate preventative interventions. PACE is affiliated with the Early Psychosis Prevention and Intervention Centre (EPPIC), a clinical/research service targeting young people experiencing a first psychotic episode [10].
Method
From March 1995 to October 1996, young people who were referred to PACE and met inclusion criteria were invited to become involved in the associated research program. The inclusion criteria for the Clinic have been described previously [9] and are summarised in Table 1. In addition to meeting criteria for one or more of the intake groups, research participants must be aged between 14 and 30 years, and have not experienced a previous psychotic episode.
Intake criteria for the PACE Clinic
The 45 young people who met intake criteria and are included in this survey are participants in a larger study aimed at identifying markers of increased risk of psychosis. As described above 41% of a group of young people meeting PACE intake criteria became psychotic within a 12-month period from recruitment [11]. This transition rate confirms that this group is truly at high risk of first onset psychosis within a short follow-up period.
All referrals to PACE were initially triaged over the telephone. If the referral was thought to be appropriate, a more formal assessment was conducted with the young person and family. As a routine component of the triaging and assessment process, potential clients, their family members and the referrer were asked to indicate previous contacts made with health and allied services prior to referral to PACE. That information forms the basis of this report.
Results
Over the 20-month recruitment period, PACE received 162 referrals. Sixty-one percent of referrals were male and the average age at referral was 18.80 years (SD = 3.39).
As shown in Table 2, the majority of young people referred to PACE were not formally assessed either because they did not meet intake criteria at the triaging point in the referral process (22.8%) or did not attend their appointment (26.5%). A search of the psychiatric services data base has revealed that two people referred to PACE who did not attend their assessment and four who were assessed and met at-risk criteria but who refused further contact became psychotic at some later stage over the next three years. Of the 96 assessment interviews conducted, 58 young people (35.8% of the 162 referred) met inclusion criteria for PACE. Forty-five people who met criteria agreed to be included in the research project, 27.8% of total referrals to PACE and 73.8% of those meeting intake criteria.
Outcome for those assessed at PACE (March 1995-October 1996)
Referral sources
The source of all direct referrals received by PACE in the recruitment period are displayed in Fig. 1. The major referral source was the Early Psychosis Assessment and Crisis Team (EPACT), a specialised early psychosis assessment team (the name of this team has recently changed to Youth Access Team). Referrals were received from generic and mental health services, school and university counsellors and youth housing and employment workers. The source of referrals received by EPACT, subsequently passed on to PACE, is shown in Figure 2.
Source of referrals to PACE, March 1995 to October 1996: did not meet other criteria at assessment;  , did not attend appointment;
, did not attend appointment;  , met criteria, refused research;
, met criteria, refused research;  , agreed to research.
, agreed to research.
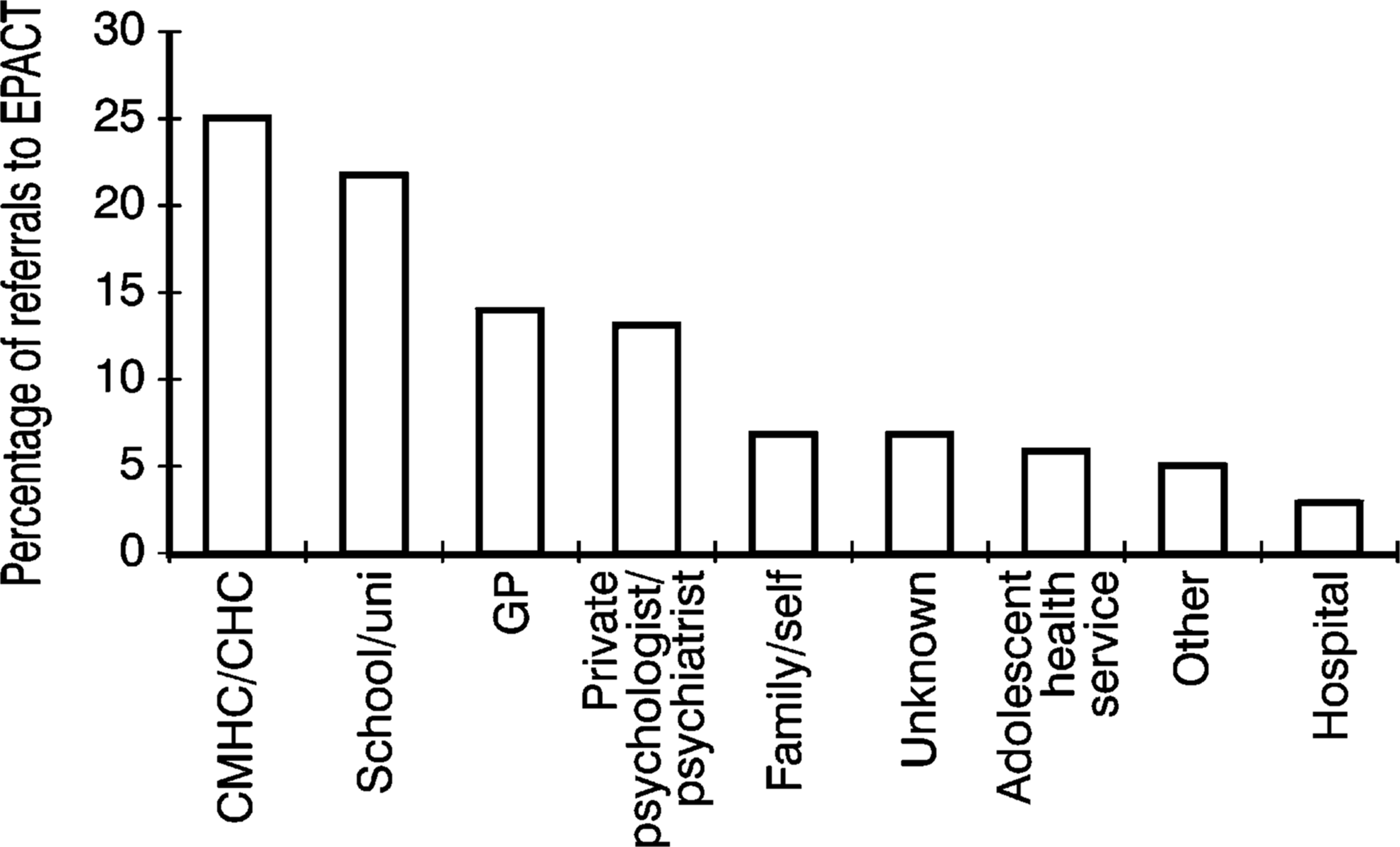
Source of referrals to PACE via EPACT, March 1995 to October 1996.
The ‘appropriateness of referrals’ was examined in some detail (Fig. 1). General practitioner referrals most often met intake criteria followed by referrals from EPACT and adolescent health and welfare services. The percentage of appropriate referrals received from schools and colleges was about 3.1%.
More information is known about the ‘pathway to care’ of the 45 people who met criteria and took part in further research at PACE. The mean number of contacts made with health or allied services of this cohort prior to contact with PACE was 2.36 (SD = 1.32; range = 1–7). This indicates that prior to contacting PACE each person had spoken to approximately two other service providers (general practitioner, private psychiatrist or school counsellor for example) about the symptoms they were experiencing. The patterns of contacts are shown in Fig. 3. This information does not indicate whether services were accessed concurrently, if the search for help was temporarily ceased at any stage, or the treatment received at each step. It does indicate that potential clients tended to access general health services or other professional services early in their pathway to PACE and later accessed mental health services.
Steps in pathway to PACE for 45 subjects in ongoing research (first four contacts shown): first contact (n = 45); , second contact (n = 33); , third contact (n = 19); , fourth contact (n = 6).
Time between onset of symptoms and initiation of help seeking
The 45 people who agreed to take part in further research associated with the PACE Clinic were asked how long they had been experiencing their symptoms. The average time between symptom onset and initiation of help seeking was 85.8 weeks (SD = 132.71). Additionally, the average length of time between making first contact in the pathway and subsequent referral to PACE was 41.4 weeks (SD = 91.4). Therefore, the average time from onset of symptoms to contact with PACE is approximately 2.5 years (127 weeks).
Discussion
This paper has examined the pathway to care of young people referred to the PACE Clinic over a 20-month period. The referral pathway for 45 young people who took part in other research projects was assessed in more detail.
As anticipated, a lengthy delay was found between onset of symptoms and the initiation of help seeking by the high-risk cohort. The young people recruited by the PACE Clinic had been experiencing some change in mental state for over 18 months, on average, before seeking treatment. Reasons for this delay were not assessed but may include: mild symptoms, egosyntonic nature of symptoms, non-referral from other services, a lack of knowledge about PACE, a general reluctance of young people to seek help from mental health services, misinterpretation of symptoms (viewed as a phase of adolescence), self-medication with substances or fear of stigmatisation or labelling. This has potential implications for illness outcome: early treatment in the course of psychotic illnesses may prevent the emergence of further symptoms [19]. Education of young people and their families about mental health and the need for early treatment may reduce this delay, with obvious benefits for long-term outcome.
As well as a delay in the initiation of help-seeking, almost a year passed from initial contact with health services to contact with the PACE Clinic. The average length of the prodrome has been reported between 52 and 104 weeks [17]. In this study, an average of 130 weeks passed between the onset of symptoms and contact with the PACE Clinic. PACE clients, therefore, present for treatment relatively late in the development of disorder, for some at least at a highly incipient stage [20]. Over this time, the high risk cohort had made contact with, on average, two other services-similar to the first-episode cohorts studied [16,17]. Help-seeking began with approaches to general health or counselling services: contact was made with mental health services sometime later.
The majority of referrals received by PACE over the 20-month period under observation were received from EPACT, a specialised assessment team identifying young people experiencing a first psychotic episode, or generic mental health services. The high number of referrals from EPACT is not surprising given the bias of this assessment team towards identifying first episode psychosis. In addition, PACE has been affiliated with EPACT throughout its development. The large proportion of referrals from other mental health teams suggests that it is useful for a service targeting a high-risk group to maintain close links with other mental health assessment teams, certainly not a novel suggestion. A centralised or combined triaging system might decrease the number of contacts made by clients in their search for treatment, as well as reducing the potential trauma associated with contacting mental health services and delays in receiving appropriate treatment.
Only 70% of those offered an assessment at PACE actually attended the session. It is unknown why the remaining 30% did not attend, an obvious limitation to this discussion. At least two of these people subsequently developed a psychotic illness and may have met intake criteria if assessed. A flexible approach to assessment including an outreach capacity and conducting joint assessments with referral services would potentially decrease the proportion of non-attendees, some of whom may also be at high risk of transition. Young people who were assessed at PACE but did not meet criteria were often referred elsewhere for treatment, another step in their own pathway to treatment and further delay before appropriate treatment. A generic youth mental health assessment system that directs clients to the most appropriate clinical service would facilitate the pathway to psychiatric care, potentially reducing the frustration experienced by clients and families when accessing mental health services. Two recent papers outline a model for such a service [21,22], suggesting that it might be appropriate for psychotic disorders as well as a wide range of psychiatric disorders affecting young people.
Community development and education about PACE has been an integral component of the service. This involves speaking with workers who are in contact with young people about PACE and possible indicators of emerging psychosis. The number of appropriate direct referrals, those that have not been referred to EPACT, initially indicates that these activities have been somewhat successful. Many referrals have been required to yield the actual PACE group, however, which has economic implications for the clinic in time spent assessing inappropriate referrals. Continued education, and links with, allied services are required to ensure appropriate referrals are obviously required.
The need for continued community liaison and promotion of PACE to potential referrers is also reflected in the average of two contacts made by patients prior to being referred to PACE. This is lower than the number of contacts made by a first episode population prior to receiving appropriate treatment [17] and suggests that young people who contact PACE are a subgroup of the entire prepsych-otic population. They might be more open to help seeking than other people in the prepsychotic phase.
The high-risk cohort tended to access non-mental health professionals relatively early in their pathway to care and later sought assistance from psychiatric services. This replicates the pattern observed in a first episode psychosis [23]. Education about emerging psychotic processes targeting non-mental health services providers aimed at youth may reduce the extra steps taken to access care. The extended length of time between symptom onset and initiation of help-seeking suggests that population based education programs addressing mental health issues is required.
The examination of referral patterns to the PACE Clinic indicates the need for certain strategies to enhance the number of direct referrals received and to reduce the amount of time between onset of symptoms and referral. These are: (i) further community development activities aimed at health professionals and allied services; (ii) separate education programs targeting young people and carers about services available to those experiencing symptoms indicative of high risk for a range of potenitally serious mental disorders (not just psychosis) and about mental health in general; and (iii) the establishment of a generic, integrated youth assessment service.
The experience at the PACE Clinic indicates that it is possible to provide a clinical service for young people at risk of developing a psychotic illness. Since this has not been possible anywhere until recently, it is obvious that there is a degree of difficulty in accessing this population. Further, only a small proportion of those young people who are experiencing the prodromal phase of a psychotic illness (true positives) actually come into contact with the PACE Clinic. Further community education and a flexible approach to accessing young people who fulfil the intake criteria, should ensure that more appropriate referrals are received. Thus, it might be possible to establish mental health services with a preventative framework, potentially in partnership with primary carers and focusing on the onset phase of other potentially serious mental health problems, such as depressive or anxiety disorders which also tend to emerge for the first time in the 12–26 years age range [6,22].
Footnotes
Acknowledgements
This work has been conducted with the support of the Victorian Health Promotion Foundation, Janssen-Cilag, RADGAC, Department of Human Services Victoria, North-west Healthcare Network, the Centre for Young People's Mental Health and the Centre for Adolescent Health.