
Abstract
A large number of reviews have documented the efficacy of cognitive-behaviour therapy (CBT) for depression [1–5]. The general finding is that CBT for depression is at least as effective as alternative major treatment approaches such as drug therapy or interpersonal therapy. The efficacy of CBT is, therefore, now widely accepted, and is generally no longer at issue. Significant debate has emerged, however, about the theoretical status of the cognitive theory of depression, and the relationship between cognitive theory and cognitive-behaviour therapy. Some authors have criticised a lack of adequate specification of how therapeutic change may occur during CBT [6–8]. The debate is of some importance, since a well-developed theoretical explanation is a necessary basis for a persuasive rationale for the treatment of depression through CBT.
One challenge which arises for the theoretical validation of cognitive-behaviour therapy is a range of findings which indicates that cognitive change accompanies other treatments for depression besides CBT [3,[9–11]]. Oei and Shuttlewood [8] note also the repeated findings that different forms of therapy have comparable levels of efficacy for a given psychological disorder. In this context, the lack of a precise specification of the imputed process of therapy leaves open the possibility that the therapeutic change documented for CBT for depression may be due to factors other than those attributed to cognitive-behaviour theory [8]. Accordingly, such a lack challenges cognitive-behaviour theorists to carefully demonstrate the postulated change mechanisms of CBT.
Thus far, relatively few empirical studies have reported findings that directly link cognitive change in CBT to improvement in symptoms of depression. In their meta-analysis of 44 process studies of therapy for depression, Oei and Free [9] report that only 21 studies satisfactorily examined the relationship between change in cognition and change in depression. These studies included cognitive therapy, other psychological therapies, drug therapy and a waiting-list control condition. They concluded that positive cognitive change occurred for all groups. However, improvement in depressive symptoms occurred only for the treated groups, with no evidence of superiority of any one of the three classes of treatment. When the relationship between cognitive change and change in depression was considered, Oei and his associates [3, [7], [9]] found a clear positive relationship both for cognitive therapy and other psychological therapies, and a less clear association in the case of drug therapy. The authors concluded that the investigation provided some support for the basic tenet of cognitive theory, that cognitive change occurs during therapy for depression. Although cognitive change was linked to change in depression, these changes happened in a minority of the studies, and were not limited to CBT.
The comparisons made in these studies of cognitive change and its relationship with depression were with control groups or with other treatment groups. A more theoretically revealing comparison would be between recovered and non-recovered groups. In other words, the design of the study changes from a treatment outcome type to a process of change type (see [12–13]). To date, very few studies appear to have focused on the cognitive change and recovery status of patients after receiving CBT. The present study seeks to address this lack. If a cognitive account of recovery due to CBT is to be supported, there should be differences between recovered and non-recovered patients on cognitive change so that recovered patients show a greater reduction in negative thinking, especially in automatic negative thoughts, which are the supposed proximal trigger for depressive symptoms. Two specific hypotheses were proposed. First, scores on negative cognition should be lower for recovered patients than non-recovered patients by the end of a group CBT program. Secondly, the rate of cognitive change should be faster for the recovered group than for the non-recovered group.
Method
Participants
The participants were 67 patients who completed group CBT programs for depression conducted between 1992 and 1994. Patients were identified as ‘recovered’ if their end-treatment score on the Beck Depression Inventory was less than 10, which is the lowest or ‘minimal’ category of depression, or ‘nonrecovered’ if their score was 10 or more, which comprises the ‘clinical’ range of 10–63 [14]. The criterion of 10 for clinical effect has become a widespread convention, and is supported through the normative work of Nietzel, Russell, Hemmings and Gretter [15], and Jacobson and colleagues [12–13].
Biographical characteristics of the subjects
Procedure
Participants in the group CBT component were recruited from the Brisbane community through local media release seeking persons suffering from depression who were willing to participate in a research project. Before acceptance into the group CBT program, patients had been initially screened through telephone interviews and were subsequently interviewed using the Structured Clinical Interview for Depression (SCID), which is a rating procedure based on the criteria for depression contained in the DSM-III-R criteria [16]. Patients meeting criteria for current major depression (single episode or recurrent) or dysthymia were selected for participation. Persons with a bipolar mood disorder or other major psychiatric disorder (e.g. schizophrenia, personality disorder), an organic brain disorder, substance abuse or problems in reading English were excluded from the study.
The cognitive-behaviour therapy program
Cognitive-behaviour therapy was delivered in a series of identical programs which were conducted between 1992 and 1994. Each program consisted of 12 2-h group format sessions, held once a week. The psychoeducational program was designed by Free [17] and based on the work of McMullin and Giles [18–19] and Lewinsohn and colleagues' ‘Coping With Depression’ course [20]. For further details, refer to earlier paper [17]. Six therapists participated in delivery of the program, all of whom were clinical psychologists experienced in the CBT theory and methods used in the program.
Measures
The following measures were used: Beck Depression Inventory (BDI) [21–22], client's mean weekly mood/activity ratings, therapist rating of patient's depression, Automatic Thoughts Questionnaire (ATQ) [23], Dysfunctional Attitudes Scale (DAS) [24,[25]], Hopelessness Scale (HS) [26], and clients' perception of effectiveness of the program for treating their depression. The mean-weekly mood rating was derived from the client's daily self-ratings of mood level, using a 9-point scale (range: 1=very depressed, 9=happy). The mean-weekly activity rating was derived from the client's daily self-ratings of activity level, using a 9-point scale (range 1=no activity, 9=extremely active). The therapist's weekly rating of patients' depression consists of the therapist's observational rating of each patient's depression on a scale of 0–100%, and was based on the patient's presentation and demeanour in the group at weekly sessions. It was to be expected that this measure would be consistent with the BDI and thus would discriminate between recovered and non-recovered groups during the process of therapy.
The question of what constitutes recovery from depression was an important one for the interpretation of findings in the present study. The use of the BDI for outcome research in depression, with a score of 10 as the cut-off point of the clinical range, has now become widespread [14–27]. Furthermore, in a study which used a therapy program very similar to that used in the present study, Free et al. [17] carefully considered the way in which treatment effect for group CBT of depression could be best assessed, in view of ethical difficulties over random assignment of patients to a control group, and doubts about whether treatment-control group differences could sufficiently show symptom change which might be meaningful to patients. They chose to use normative methods [12,[13],[15]] where post-treatment change in depression can be compared with the distribution of scores for clinically identified but non-distressed persons or for population norms. These procedures resulted in a BDI clinical cut-off point of 9.72 as a norm for non-distressed persons. These findings were regarded as providing support for the use of a BDI level of less than 10 to indicate remission of depression in the present study.
During weeks 4, 8 and 12 sessions of the program, patients were also asked to rate a range of therapy variables. Two measures were used, the first assessing the client's belief that the therapy would help his/her depression (rated on a 5-point scale), and the second assessing the client's perception of the usefulness of information provided in therapy (also rated on a 5-point scale). These measures were taken to investigate whether therapy variables such as credibility and perceived usefulness of skills and information taught in this CBT program differentiated the recovered and non-recovered groups.
Methods
Analysis was conducted using the Statistical Package for Social Sciences (Windows version). Chi-squared tests showed that the recovered and non-recovered groups did not differ on demographic variables such as gender, age, education level, or marital status. Separate two-way mixed model ANOVAS with between-groups factor recovery (recovered vs non-recovered) and within-groups factor time (measured at intervals across the 12 weeks of therapy) were performed on each dependent variable. A significance level of 0.05 was applied in all statistical tests, except where mean substitutions were necessary to enable analyses (due to scattered missing cases across some of the frequently repeated measures). In such a situation, the significance level was raised to 0.01 in order to reduce Type 1 error.
Beck Depression Inventory scores
Mean BDI scores for recovered and non-recovered patients at each assessment point during the CBT program are presented in Figure 1 The results of an ANOVA performed on these data reveal a main effect for recovery (F1,63=31.84, p<0.001), and time (F5,315=38.08, p<0.001), modified by a significant recovery by time interaction (F5,315=7.92, p<0.001). Figure 1 shows that the interaction occurs because mean BDI scores for both groups decreased over the duration of the CBT program, but the rate of change was faster for the recovered group than the non-recovered group. As expected, the recovered group showed faster improvement (i.e. sharper decline in BDI scores) than the non-recovered group.
Mean Beck Depression Inventory (BDI) scores: _ _ _ _ _, recovered; _____, non-recovered.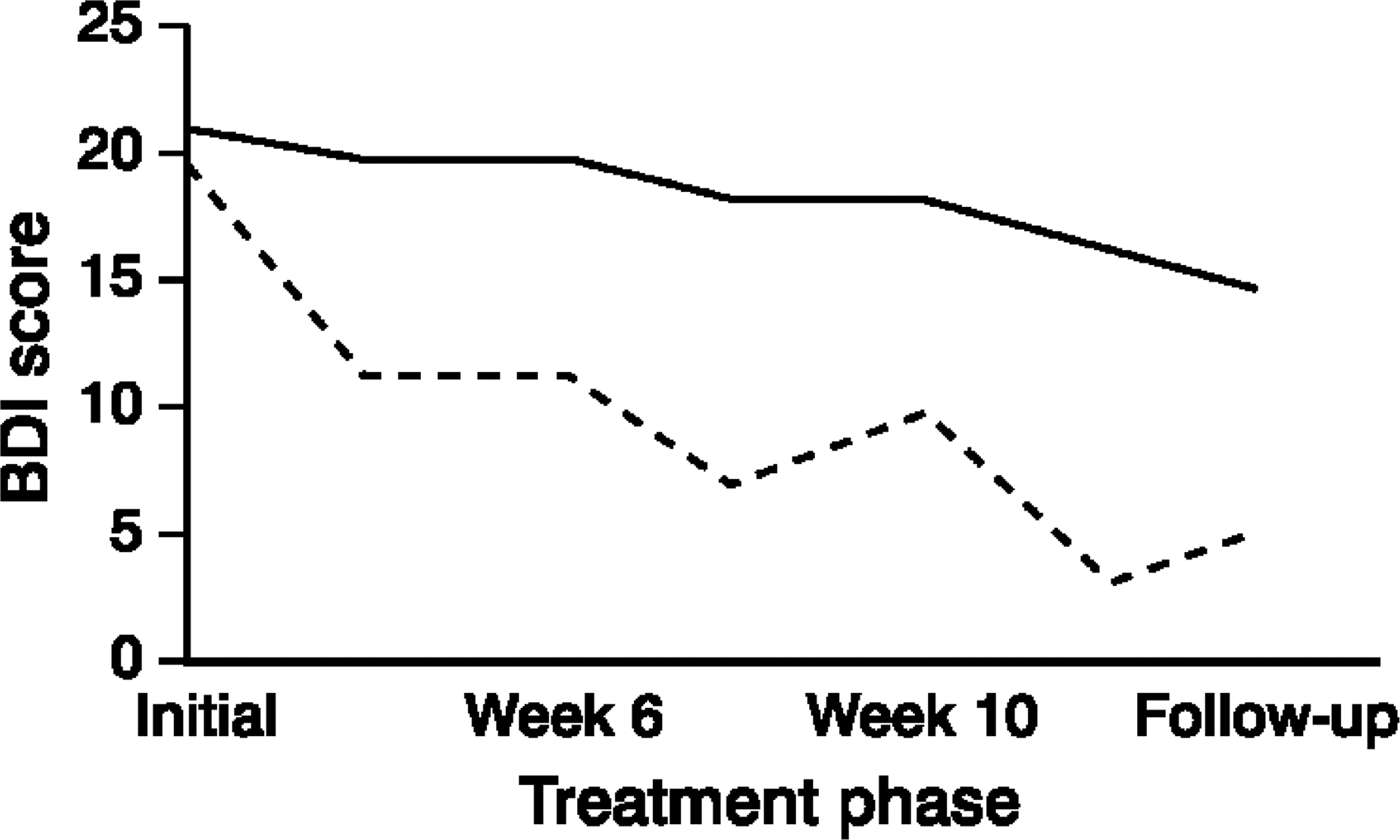
Mean-weekly mood self-rating
Figure 2 presents the mean-weekly mood self-ratings for the recovered and non-recovered groups over time. Mean substitution was used because of scattered missing scores at some measurement points. The ANOVA revealed main effects for recovery (F1,65=9.15, p<0.01) and time (F11,715=20.21, p<0.001). However, no significant interaction was found. This result suggests that mean-weekly mood self-rating levels for the recovered group were consistently higher than those of the non-recovered group.
Mean weekly mood self-rating: _____, recovered; _____, non-recovered.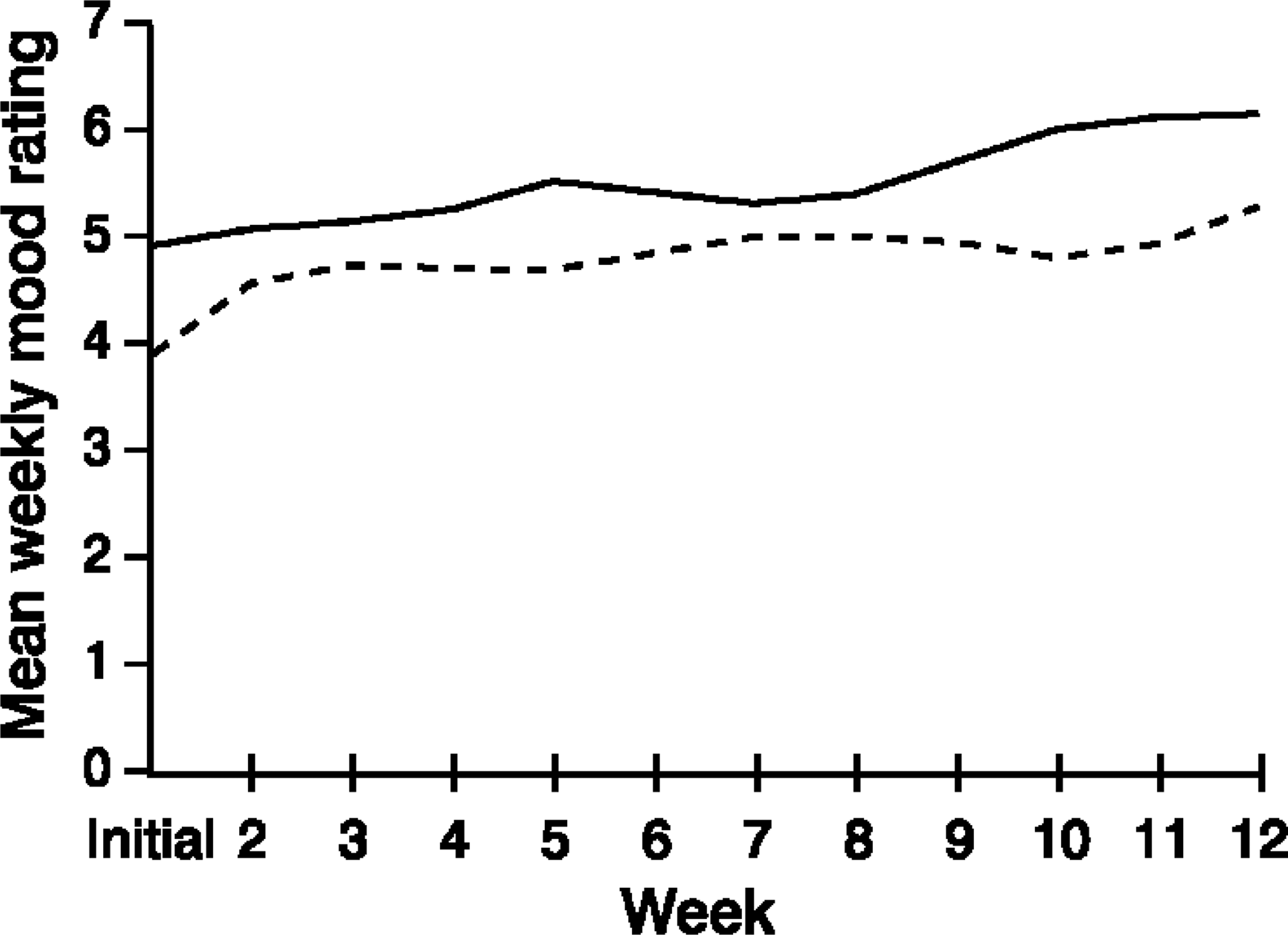
Mean-weekly activity self-rating
Figure 3 shows the mean-weekly self-ratings of activity level for the recovered and non-recovered groups. A two-way ANOVA for repeated measures using a mean substitution was performed. Significant main effects were found for recovery (F1,65=7.62, p<0.01), and for time (F11,715=8.19, p<0.001). The recovery by time interaction was not significant. This result suggests that the recovered group had significantly higher self-rated activity levels than the non-recovered group, but that rate of change in self-rated activity did not differentiate the recovered and non-recovered groups.
Mean weekly activity self-rating: _____, recovered; _____, non-recovered.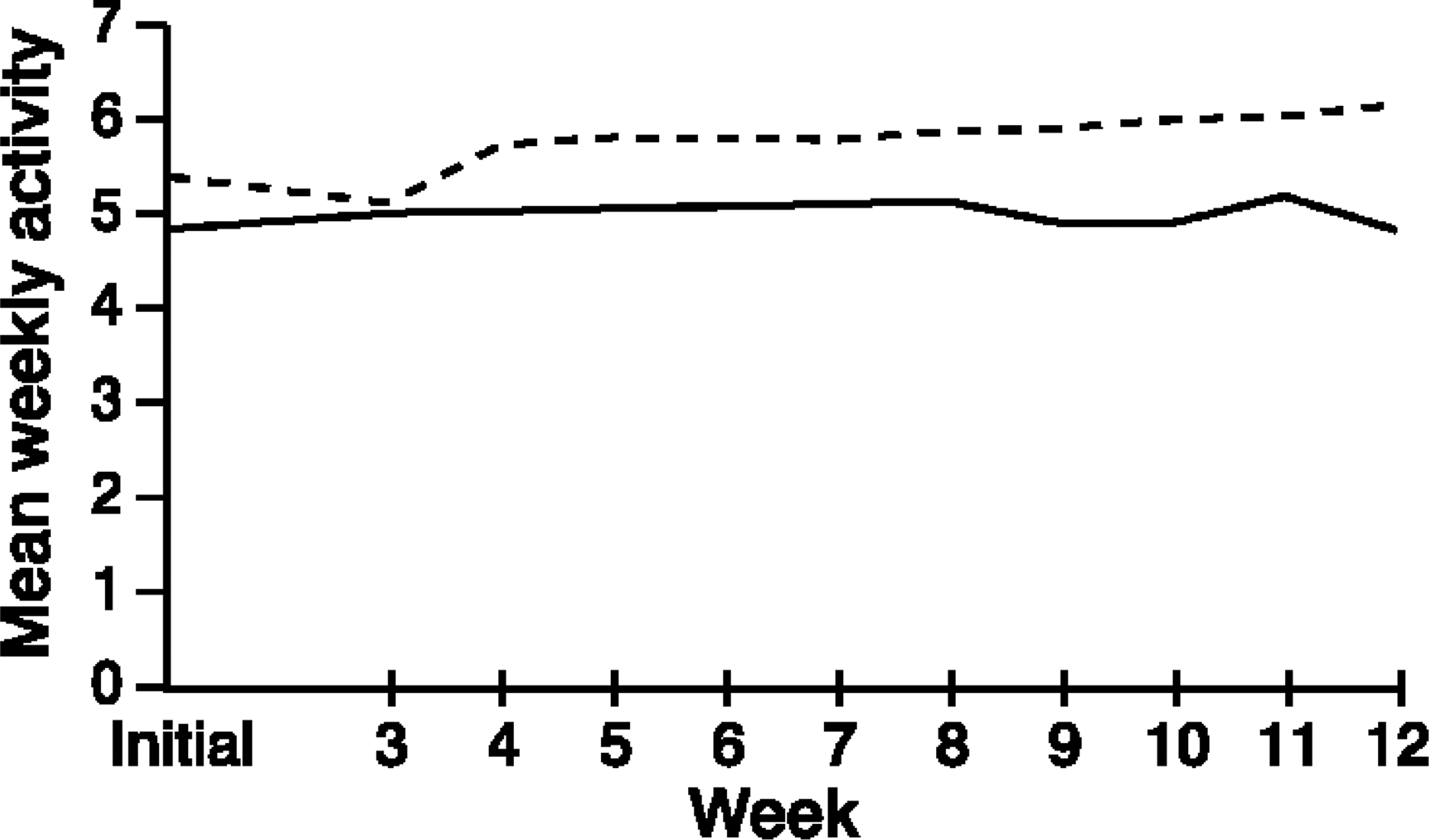
Therapist's weekly rating of patient's depression
Therapist's weekly rating of overall depression of recovered and non-recovered groups are presented in Figure 4 Therapist-rated depression is similar for both the recovered and non-recovered groups over the course of the program, with an exceptional rise for the non-recovered group at week 10. A repeated measures ANOVA with mean substitution revealed a significant main effect for time (F11,715=55.53, p<0.001), but no significant interaction effect. This result suggests that both groups were perceived by the therapists to have similar levels of depression, with both groups showing improvement over time, but that rate of change did not differentiate between the recovered and non-recovered groups.
Weekly therapist-rated depression: _____, recovered; _____, non-recovered.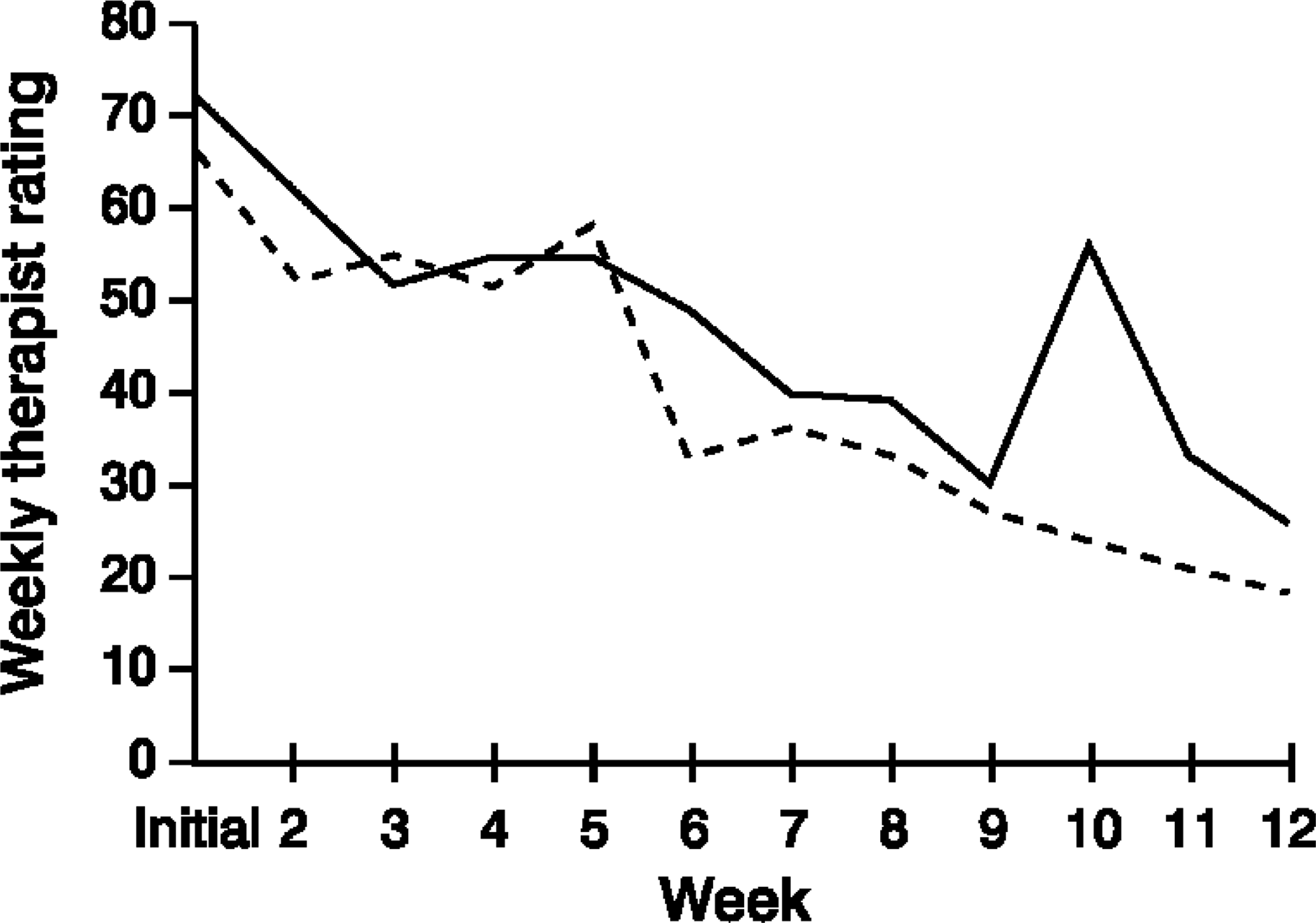
Automatic Thoughts Questionnaire scores
Figure 5 presents the mean ATQ scores for recovered and non-recovered patients over the course of the CBT program. An ANOVA performed with the ATQ scores revealed significant main effects for recovery (F1,63=6.70, p<0.05), and time (F5,315=26.11, p<0.001), and a significant interaction of recovery with time (F5,315=3.18, p<0.01). Figure 5 shows that the interaction occurs because ATQ scores were lower in the recovered group than the non-recovered group, and this difference increases over the course of treatment. Consistent with the cognitive theory of depression, this measure of cognition significantly differentiates the recovered from the non-recovered group in terms of both absolute level of scores and change during the process of therapy. Automatic Thoughts Questionnaire scores for the recovered group increasingly diverged from those of the non-recovered group, with the difference being most pronounced at the end of program.
Mean Automatic Thoughts Questionnaire (ATQ) scores: _____, recovered; _____, non-recovered.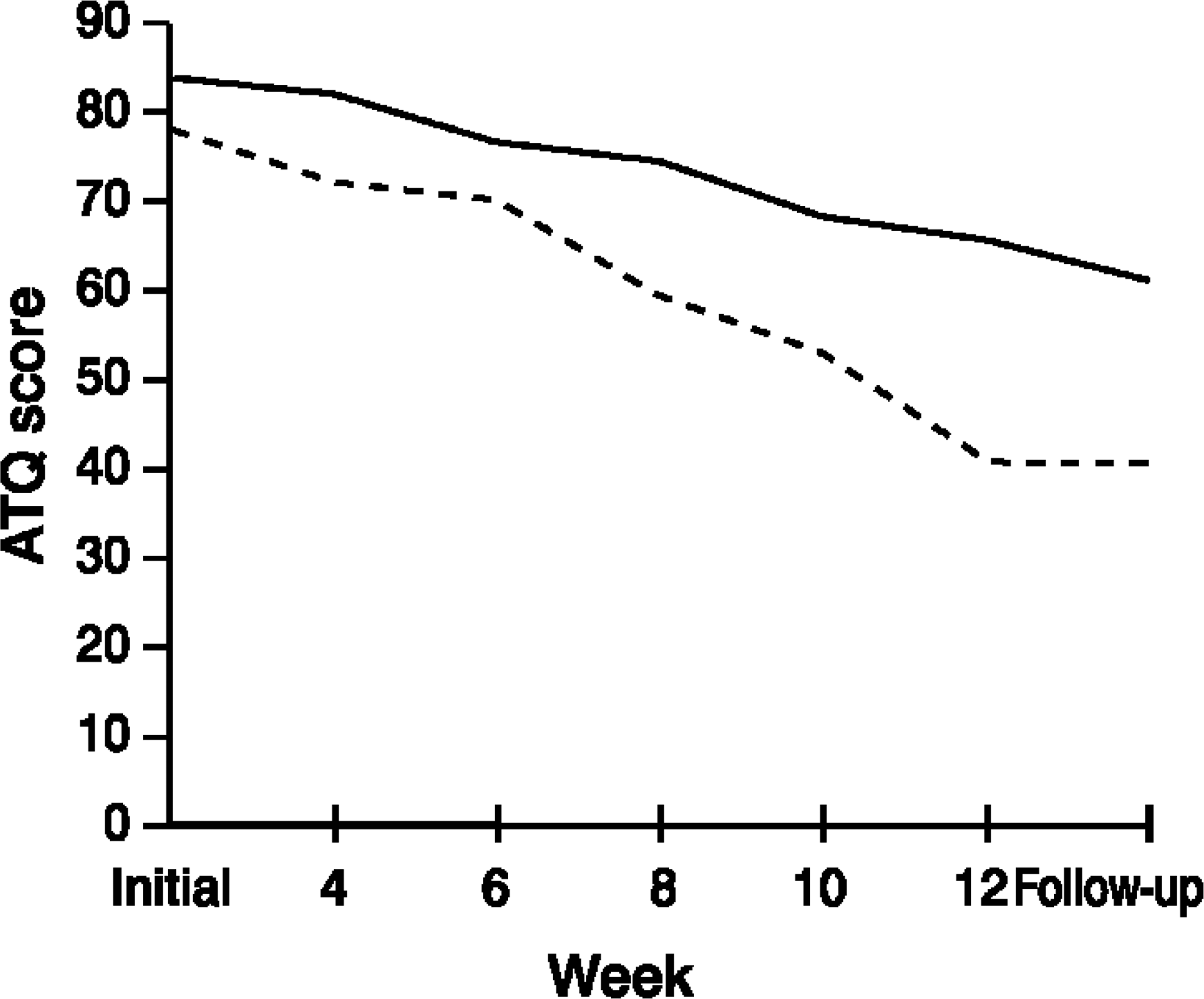
Dysfunctional Attitudes Scale scores
Figure 6 shows the mean DAS scores for recovered and non-recovered patients over the course of the CBT program. ANOVA analyses found a significant main effect for time (F5,315=12.54, p<0.001), but not for recovery. The recovery by time interaction was signficant (F5,315=5.92, p=0.001), indicating that while the overall level of DAS scores did not differentiate between the recovered and non-recovered groups, there was a divergence of pattern of scores for the two groups over the course of CBT. Scores for the recovered group increased more than those for the non-recovered group during the second half of the program.
Mean Dysfunctional Attitude Scale (DAS) scores: _____, recovered;_____, non-recovered.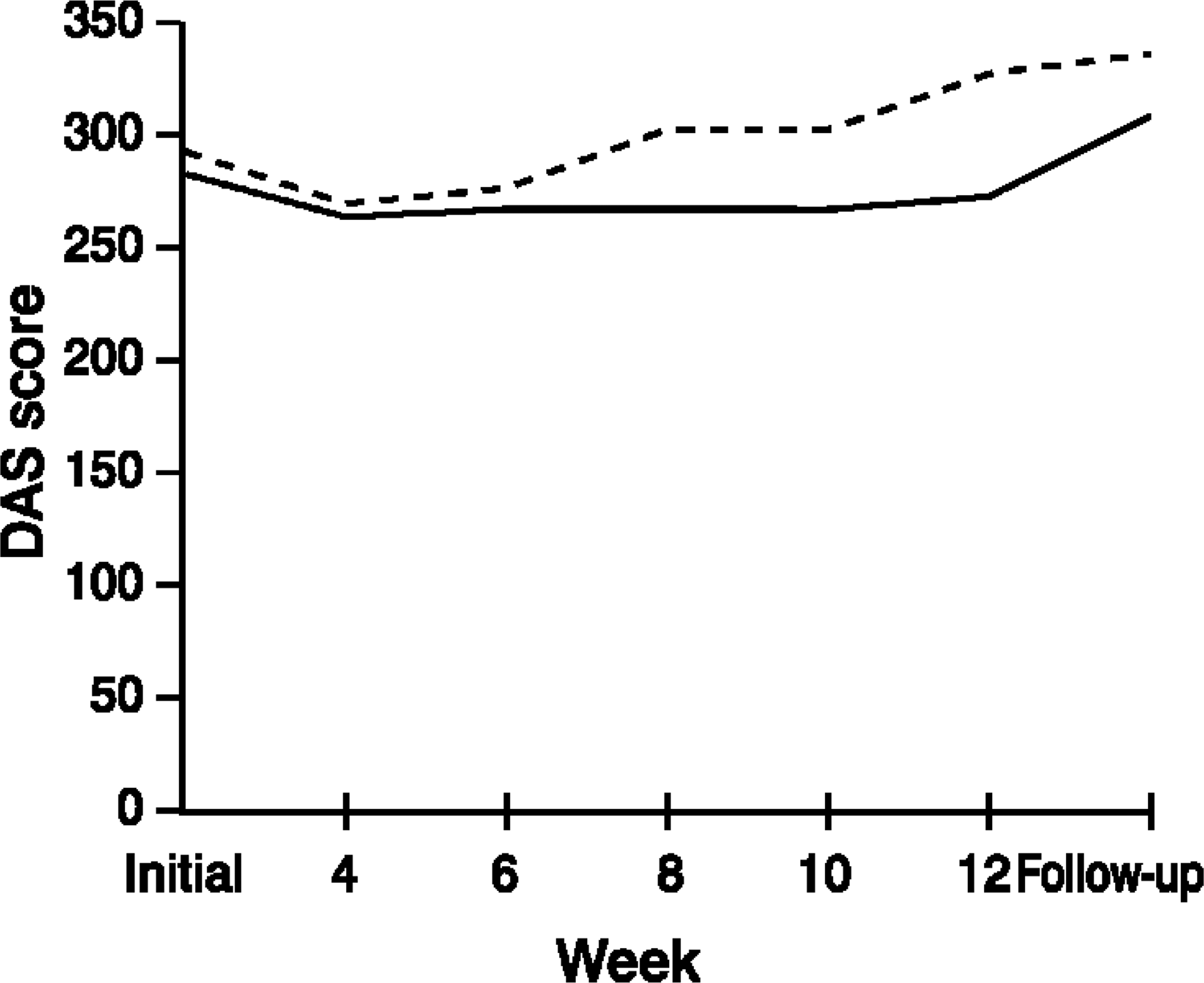
Hopelessness scores
Mean hopelessness scores for recovered and non-recovered patients over the course of the CBT program are shown in Figure 7 Results of ANOVA analyses indicated that the main effect for treatment was significant, (F1,63=5.92, p<0.05), as was the main effect for time (F5,315=8.37, p<0.001). However, the interaction effect of treatment with time was not significant. This result suggests that while the two groups were significantly different on this measure, and that each group showed lower scores over the duration of the therapy program, there was no significant difference in the rate of change between the two groups.
Mean Hopelessness Scale score: _____, recovered; _____, non-recovered.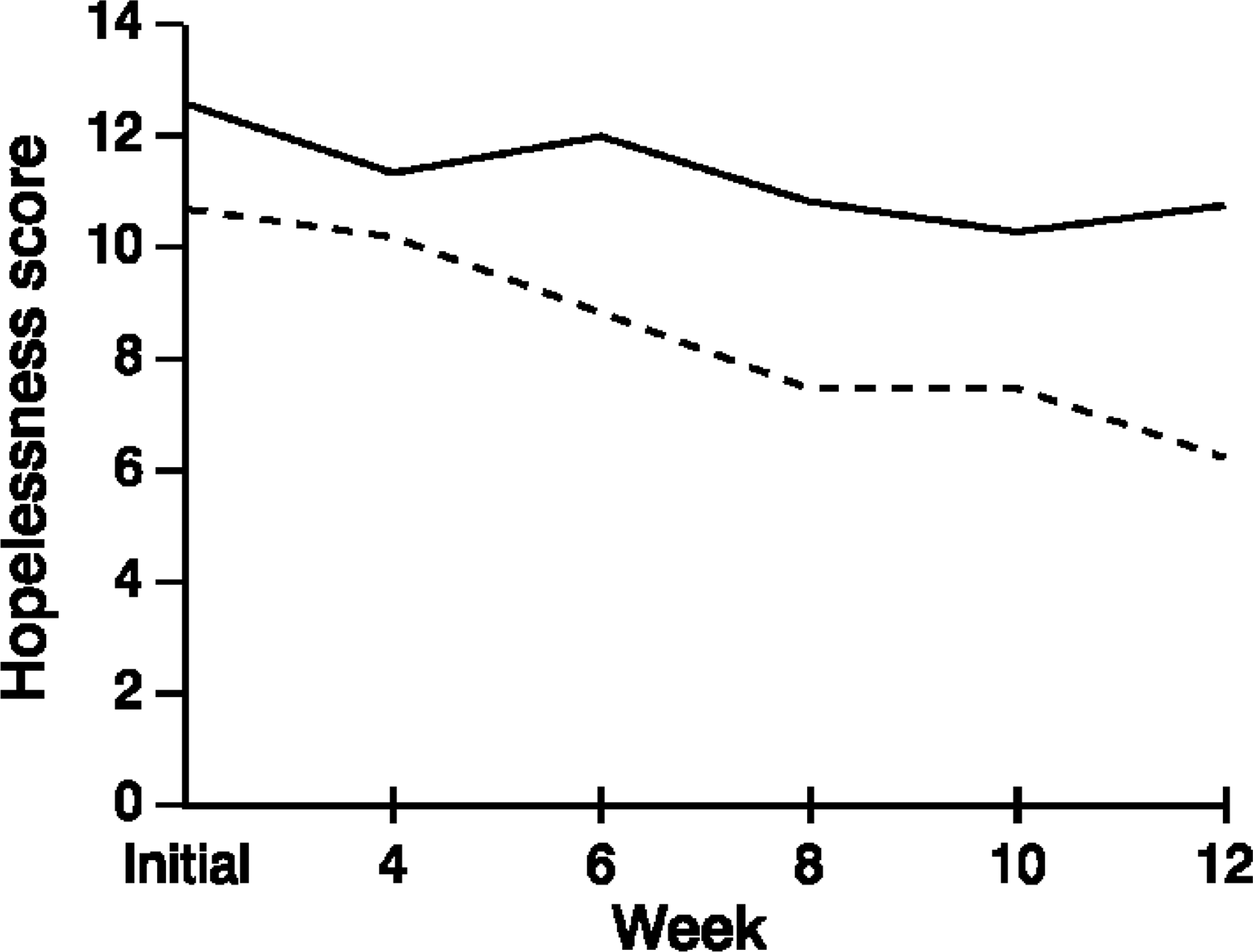
Clients' ratings of the therapy program
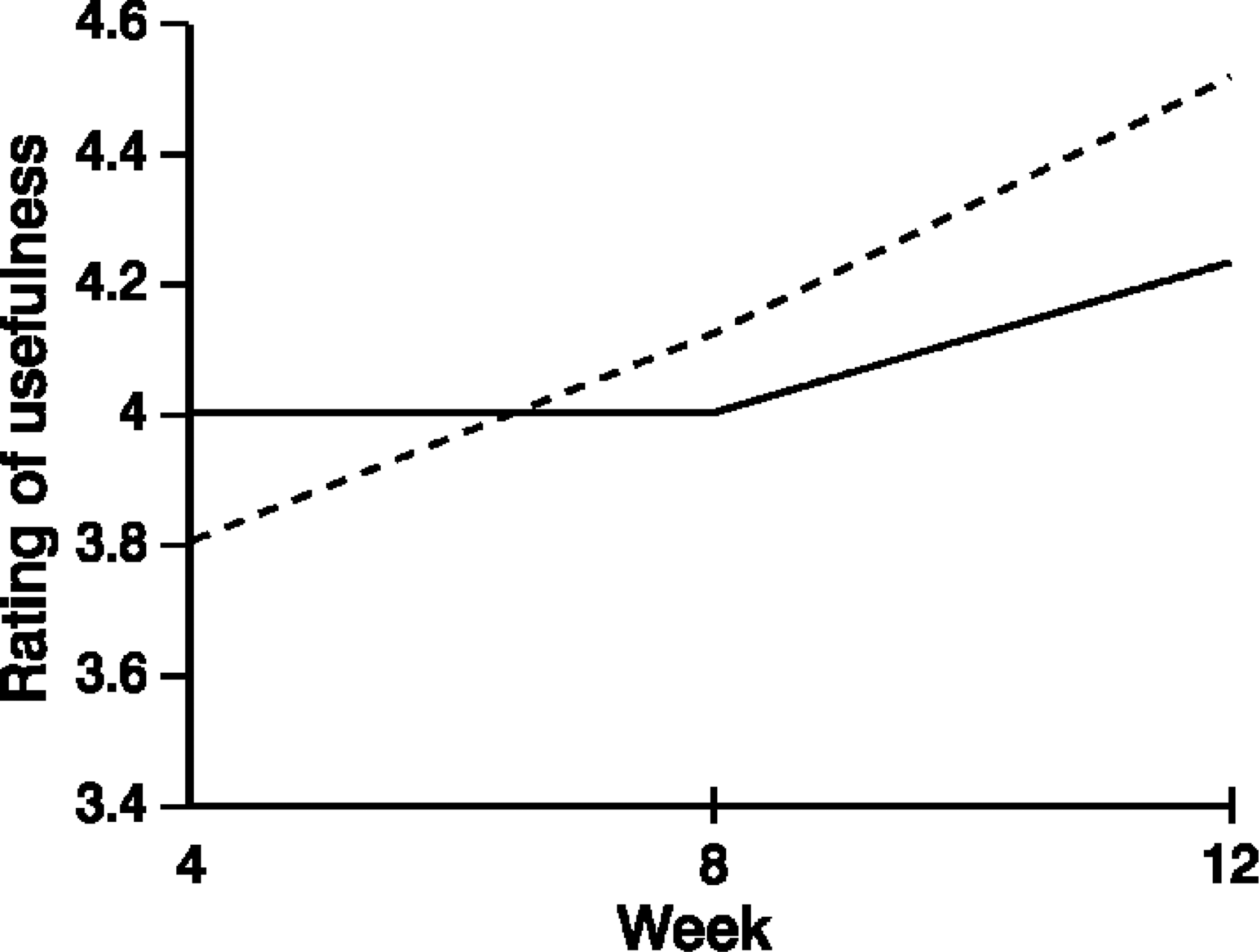
Figure 8 shows ratings of clients' belief that therapy will help depression for the two groups over the course of the program. An ANOVA on these data found no significant main effect for recovery, but there was a significant main effect for time (F2,130=18.61, p<0.001). The interaction was not significant. The main effect is due to higher ratings of belief that therapy will be beneficial over the course of CBT in both groups. Figure 9 shows ratings by the recovered and non-recovered groups of the extent to which information provided in therapy was useful. Again, the ANOVA analyses revealed a significant main effect for time, (F2,130=19.96, p<0.001), but no main effect for recovery and no significant interaction effect, F2,130=1.70, p=0.19. This result suggests that the perceived usefulness of information increased for both groups over the course of therapy.
Belief that therapy will help depression: _____, recovered; _____, non-recovered. Information provided in therapy found useful: _____, recovered; _____, non-recovered.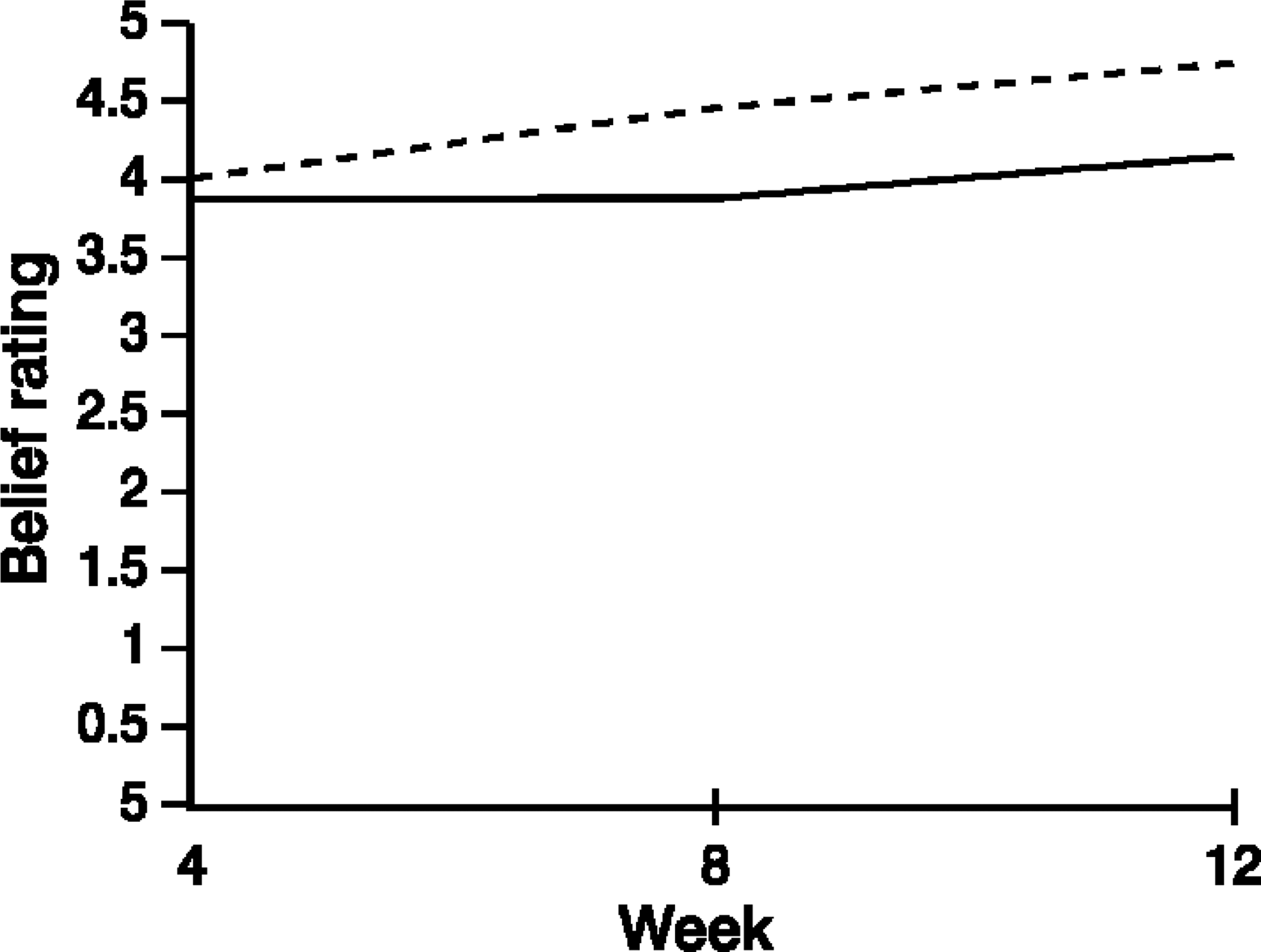
Discussion
The present study sought to make a contribution to the understanding of cognitive influences in recovery from depression. The results supported the two main hypotheses. First, recovered participants exhibited significantly lower scores on measures of negative cognitions by the end of the CBT program. Second, the difference between recovered and non-recovered participants on cognitive measures increased over the duration of therapy.
The present findings confirmed the differential response to the program of recovered and non-recovered groups on a variety of measures of depression. Mean mood self-rating rose significantly for all patients over the duration of CBT, although it was found to be significantly higher (i.e. more positive) for the recovered group as compared to the non-recovered group. Mean self-rating for activity level also rose significantly for all patients over the course of the program, but the level was significantly higher for recovered patients. Therapist-rated depression showed a significant decrease for all patients over the program, but did not differentiate between groups. These findings are consistent with the results for the BDI, which in turn were generally consistent with findings concerning the efficacy of cognitive forms of therapy [9].
The analysis of ATQ scores confirmed the expected differences in automatic thoughts of recovered and non-recovered patients. Automatic Thoughts Questionnaire scores were significantly lower for the recovered group, indicating fewer negative thoughts in the recovered than the non-recovered patients. Furthermore, there was a greater rate of decrease in scores for the recovered group on this measure of negative automatic thinking. Of special interest also, the recovered group changed from a clinical to a non-clinical level on the ATQ over the course of the group CBT program. The findings for the measure of dysfunctional attitudes, the DAS, were slightly more complex than those for the ATQ. While no significant group differences were found, there were significant main effects for time and for interaction of recovery status with time. These findings were interpreted as confirming a hypothesised significant difference between recovered and non-recovered groups on this measure of underlying dysfunctional cognition. As a further point of interest, the graph of mean DAS scores for the two groups showed a faster rate of improvement for the recovered group after the middle phase of the program (week 6). This ‘lag’ before any change in dysfunctional attitudes occurs is consistent with the theoretical characterisation of dysfunctional attitudes as ‘deeper’, more generalised and pervasive, and thus harder to shift.
Findings of the present study may be compared with the conclusions drawn by Oei and Free [9] in their meta-analysis of 21 studies examining the relationship between change in depression and change in cognitions. The studies included both individual and group formats and covered cognitive therapy, drugs, other psychological therapies and waiting-list control conditions. In common with the present study, the most frequently used measures of negative cognition were the ATQ and the DAS. The meta-analysis revealed significant cognitive changes over the course of treatment for all types of therapy, and thus did not show a superiority of cognitive approaches over drug or other psychological therapies. A regression analysis of the relationship between depression change and cognitive change did, however, show a clear positive relationship in the case of cognitive and other psychological therapies, but not for drug therapy. While the focus of the present study was the difference in depression and cognition scores between recovered and non-recovered patients, rather than on differences among a variety of therapies, results for cognitive change are clearly consistent with those obtained for the studies of cognitive and other forms of therapies examined by Oei and Free [9].
On the Hopelessness Scale, which measures negative expectations about the future, scores for the recovered group were significantly lower than those for the non-recovered group during the course of the program. This is again consistent with the hypothesised differences in negative cognition between the two groups at the end of the group CBT. Again of interest was the drop of scores from a clinical level to a non-clinical level for the recovered group, while the non-recovered group remained at the clinical level on this measure of pessimistic expectations.
The present findings on the main measures for both depression symptoms and negative cognition were consistent with the central proposition of cognitive theory, that remediation of negative cognition plays a significant role in recovery from depression during CBT. These findings are also consistent with those reported in the relevant literature for remediation of depression symptoms and change in negative cognition. Until recently, CBT has usually been provided on an individual basis. The finding of positive therapeutic results in a group format adds support to the finding of Oei and Free [9] that group-administered CBT is of comparable efficacy with individual therapy. This in turn suggests that the mechanisms of CBT are independent of variations in format and delivery, and are thus a robust means of effecting cognitive change. These findings help to resolve the issue of group versus individual treatment for depression raised by Wilson [28].
No significant group differences between the recovered and non-recovered groups were found for therapist rating of depression, patient belief that therapy would help depression, and patient rating of the usefulness of the information provided in therapy. This finding is interesting in view of the comment by Robinson et al. [29] that factors such as client expectations of improvement and acceptance of the therapeutic rationale are possible mediators of therapeutic change.
The absence of a statistically significant group difference for therapist-rated global depression during CBT is the most unexpected of the findings. It stands in contrast to the findings for group differences on the BDI. Apart from possible psychometric weaknesses of the therapist-rated depression measure (compared to the well-established psychometric properties of the BDI), other reasons for the non-significant findings may be considered. For example, global ratings of depression may have lacked sensitivity. Alternatively, the absence of a significant group difference in therapist-rated depression may reflect the similar absence of significant group differences on perceived helpfulness of therapy and usefulness of the information provided: that is, both recovered and non-recovered patients may have appeared similar in behaviour and mood on the basis of their apparently equally positive approach to the CBT program.
Precise specification of the way in which CBT is imputed to remedy depression has remained somewhat unclear, with the issue of causality being especially ambiguous. Various speculations have been made about possible mechanisms of effecting change in CBT. Some researchers have commented, at a general level, that cognitive and biochemical aspects of depression are closely interwoven through interactive or circular processes, and CBT may be one way of breaking an otherwise self-maintaining cycle of depression [3–30]. Other theorists have suggested more detailed mechanisms through which cognitive variables may relate to the development of symptoms of depression. For example, Kwon and Oei [7] postulated that depression is due to the outcome of both the distal, moderating influences of dysfunctional attitudes and the proximal, mediating effects of automatic thoughts. This account binds together more tightly some of the concepts of cognitive theory, which Haaga et al. [4] have characterised as a mixture of descriptive and causal elements.
Although there is a need for a comprehensive theoretical explication of a cognitive account of depression, at a more basic level, the doubts raised about whether specific treatment factors might operate at all [8] require that a cognitive theory of depression demonstrate the validity of its most fundamental tenets. In this context, the present study sought to contribute to clarification of one of the core ideas in the cognitive theory of depression: that is, change of negative cognition is intrinsic to change in depression symptoms [31]. The focus of the present study on differences between recovered and non-recovered patients provides a new means of demonstrating support for such an intrinsic association. The pattern of findings confirmed the hypothesised differences between recovered and non-recovered patients, and thus provided an additional and different avenue of support for the central role of cognition in the remediation of depression. Potentially confounding factors such as differences between recovered and non-recovered groups on demographic characteristics or expectations of therapy did not appear to play a significant role in the present study. This strengthens the likelihood that cognitive factors truly distinguish the recovered from the non-recovered patients.
The issue of measurement of recovery in the present study is itself an interesting one. A distinction needs to be made between technical ‘non-recovery’, in terms of a BDI score of 10 or more at the end of the CBT program, and absence of improvement. Even for the non-recovered group, improvement was evident on most of the symptom and cognitive measures, although the recovered group showed greater gains. This suggests that group CBT may be accessible in varying degrees to different people, but that critical levels of cognitive change may be needed before therapeutic gains reach statistical and clinical levels. This in turn raises challenges for improvements in methods of explanation and skill-teaching to expand program effectiveness.
To conclude, the findings of the present study support the assertion of cognitive theory, that negative cognition is intrinsic to depression, and change in negative cognition is intrinsic in recovery to the nonclinical status. The results also reinforce previous findings [17], that CBT delivered in a group format is as effective as individually administered CBT.
Footnotes
Acknowledgements
This project was supported by a grant from the Australian Research Council. We would like to thank the patients and Ms Anna Lamberton and Dr Michael Free for their help.