
Abstract
Suicide rates in Australia are among the highest in the world [1] and in New South Wales (NSW) alone, more than 700 people die from suicide each year. Even more worrying is that for each person dying from suicide, there are another 30–40 people who attempt suicide [2]. Those who suicide tend to be young men, particularly in rural areas, older men, homeless people, and those with a mental illness such as depression [3]. It is regarded to be a serious health issue not only because of lives lost unnecessarily, but also because of the pain and suffering that affects the lives of bereaved family and friends [4]. Indeed, stigma and rejection can be experienced by the surviving family and friends soon after the incident [5–6].
Research reveals that the incidence of suicide is often associated with complex social issues such as family breakdown, unemployment, bankruptcy, sexual assault, low self-esteem, bereavement, home-lessness, poverty and drug and alcohol abuse [7–10]. Emotive responses to escalating suicide rates generally suggest remedies which concentrate on single issues, like reducing unemployment, poverty, firearms or drug use [11–18]. Yet, as Durkheim argued, both the incidence and responses to this social phenomenon should be mindful of the multiple issues relevant to the context within which suicide occurs [19]. A recent report by the Victorian coroner's working party supports such a view and suggests that a multilayered approach to suicide prevention is needed, including ‘a range of interventions incorporating general educational and promotional campaigns for at-risk groups in the community at large and the development of treatment and research centres’ [11].
This challenge has been accepted nationally in the form of additional government funding for child and adolescent mental health services, increased numbers of Aboriginal mental healthcare workers and family resource kits [2]. The launching of a $1.35 million education package for general medical practitioners and a $450 000 Internet project called ‘Reach Out’ is being used as the latest frontline approach in the fight against youth suicide [3]. The family resource kits are funded out of NSW Health's $14 million allocation to suicide prevention. The kits provide information and advice about suicidal behaviour and stress-reducing behaviours to families [2].
The support for these preventative measures acknowledges research which shows that identifying risk factors does not in itself improve the rate of prediction and prevention of suicide [20–23] and that continuity of care and aftercare of patients who have attempted suicide is a necessary strategy in future suicide prevention [24]. This finding is supported by researchers in different countries who found that the attitudes of healthcare staff towards their role in suicide prevention and support for seriously distressed individuals were important determining factors in reducing the risk of suicide [24–27]. A large body of research reveals that people at risk of suicide perceive a range of healthcare services to be unhelpful [25–27]. Hospital services are often regarded unfavourably because of poor staff attitudes to suicide attempts [26], the way that psychiatric assessments are conducted [26], misdiagnosis [20–27], clinicians' lack of empathy with and ability to deal effectively with the negative behaviours of mentally disturbed patients [28–30], and lack of referral to an appropriate therapist [29]. General medical practitioners' lack of interest and/or experience in dealing with people who present with suicide ideation and depression and their over prescription of medications for suicidal symptoms are also areas of concern [25–26].
The management of suicidal patients is complicated by the emotions expressed and demands made by the patient [28, [30], [31]], the healthcare worker's own responses to patients from different social backgrounds [32] and the influence of family and friends [28]. Positive clinical relationships between patient and clinician depends on a range of factors, such as the ability of the clinician to make a definitive diagnosis [29], the clinician's listening and attending skills, attitude and understanding of the patient's needs [33–34], the degree of patient centredness in management [33] and the expertise and experience of the clinician [29–30].
At the same time, the needs and concerns of others closely associated with the patient must also be addressed [31–35]. Very few studies consider community and consumer perspectives in assessing the effectiveness of existing services, important although they are [31, [35], [36], [37]]. Research indicates that degree of satisfaction with giving and receiving healthcare services is related to the time spent with patients and close others [30], patients being asked if they would consider receiving alternative treatments [30–33] and the degree of illness that is presenting [29, [30], [32]]. In other words, clinicians are more likely to give better care to people presenting with a mental illness or extreme emotional distress when the person's symptoms are easily recognised and severe, and the clinician is familiar with the required treatment schedule.
Twemlow, Bradshaw, Coyne and Lerma suggest that doctors need to involve family and friends in the assessment and treatment of patients presenting with disturbed behaviour, in order to ensure continuity of care and support for the person following discharge [33]. This small study considers the perceptions of close family and friends of a person who did seek healthcare support prior to their suicide, and thus offers some insights into the care received by these people. It provides, more importantly, questions for further research in this area, particularly with regard to evaluating the effectiveness of recent government initiatives in suicide prevention [36–38].
Study aims
The study had two aims. The first was to explore the kind of experiences that suicidees had when seeking support from healthcare services in the period leading up to their death, as perceived by close family and friends. The second aim was to find out what type of support was considered helpful to those at risk of suicide, from the point of view of family and close friends.
Method
This was a descriptive, interpretative study using a qualitative research approach with a small study sample. Focused in-depth interviews were conducted with the family and close friends of people who had suicided, in order to gain a clearer understanding of the circumstances surrounding the suicides and to investigate what family and friends believed were helpful and unhelpful health service supports.
Study sample
The research participants were family and close friends of young people who had suicided in Sydney, NSW, between 1990 and 1995. Fifteen people associated with 15 people who had suicided included nine mothers, one father, one sister, one girlfriend, two male friends and one female friend. All participants spoke English; however, two of the participants were of Lebanese background. None of the participants were financially disadvantaged and all lived north of the city.
The sample was selected using the following criteria: they self-selected to participate in the study; they were close family or friends of persons who had committed suicide; were willing to be interviewed and were able to give written, informed consent to participate in the study; the person who committed suicide had lived in Sydney for the last 6 months of his/her life; the suicide occurred between 1990 and 1995.
The original intention of the research was to interview people who made a suicide attempt as well as their family and close friends, but it became clear that these people were not interested in participating in the study.
To recruit participants, advertisements were placed in metropolitan newspapers, community healthcare bulletins and on local radio stations, asking for families and friends associated with suicide to participate in a personal interview with the researchers. As well, mental healthcare workers attached to hospitals were asked to refer patients to the researchers, two of whom were very experienced mental healthcare staff. However, no referrals were forthcoming and it was decided to advertise for recruits. Both purposive and snowball (nominated) sampling methods were eventually used, as only one person responded to the advertisements. The majority of the 15 participants eventually recruited were drawn from non-government organisations such as Speranza and the Compassionate Friends, which are support groups for people affected by suicide.
This limitation to sample size and composition restricted findings to the group itself, because of the difficulties associated with gaining translators for people unable to speak and understand English well enough to discuss such sensitive issues. Because of the sensitive and potentially distressing nature of being interviewed about their loved one's experiences up to their death, the researchers felt it important to recruit only those people who were quite comfortable with discussing such issues.
The reason for selecting relatives or friends of people who had suicided after 1990 was related to changes in resource allocations and health policies associated with suicide that occurred after this date. Another factor was to limit the potential for poor recall of events surrounding the suicide before this date. As this study was designed to gain an in-depth understanding of the perceptions of the study participants, rather than to gain data from which to generalise to the larger population, it was not important to recruit large numbers. As it turned out, a sample of 15 participants was found to be sufficient, as the similarities in their responses to the questions asked indicated that saturation of data responses had occurred.
Research tool
The research utilised in-depth focused interviews, which were based on the areas of most concern to participants. A semi-structured questionnaire was developed and piloted prior to the study to elicit the most important topics for interview. The questionnaire covered broad topic areas including: basic demography and employment status of the suicidee; memory of participating events leading to their suicide; history of a previous mental illness in the person committing suicide; the perceived role of general medical practitioners in suicide prevention; and the suicidees' and participants' experiences with health services prior to the suicidee's death. The data arising from the questionnaire helped to refine the interview questions, which were extended to gain information about suggestions for improving support services for people at risk of suicide.
Data collection procedures
The approval of the South-Eastern Sydney Area Health Service Research Ethics Committee was gained prior to conducting the interviews. The researchers intended to recruit participants in such a way that service users and/or a particular gender would not be over-represented; however, this proved to be difficult and ethical reasons precluded a direct approach using coronial files. Following initial telephone contact with the researchers, volunteer participants were informed fully of the nature and purpose of the study and convenient times were arranged for giving informed consent and participating in the interviews.
Interviews were conducted privately in a place chosen by the participants. Due to the sensitivity of the topic being discussed, participants were given as much time as they required. However, the approximate length of the interviews was 1.5 h. Each participant was interviewed only once. While an interview schedule was used, based on questions arising out of the results of the piloted questionnaire, the discussion with participants tended to be directed to issues of most concern to them at the time. These issues were shared by all participants and provided a measure for the researchers in knowing when saturation of data had occurred.
Most of the open-ended questions were repeated to ensure that the responses given were consistent with the intention of the questions posed. Where the participants raised issues of concern to them that were not directly relevant to the questions asked, their responses were noted and put aside for analysis at a later date. Due to the sensitivity of the issues being discussed, it was decided to take detailed, verbatim notes during interview, rather than to tape record them. It became clear during the early interviews that participants felt far too distressed to speak openly about their experiences in front of a tape recorder. The researchers felt that it was important to gain trust and rapport with participants in order to gain a clear picture of their experiences and to encourage openness with their responses to the questions. The handwritten transcripts were filed away in a locked filing cabinet at the conclusion of each interview.
Participants were made quite aware that they were at liberty to end the interview at any time and that they were able to pull out of the study or refuse to answer any question that they felt was too sensitive. This did not occur with any of the participants, although one person became quite upset when answering some of the questions. A back-up team of mental health professionals was available to support any participant who the researchers identified was in need of further help, or who asked for assistance when this was offered by the researchers. None of the participants indicated that they would like to take up this offer and the majority of them stated that being able to talk with the researchers about their experiences was in itself therapeutic. Participants were contacted following the interviews to assess whether there had been a negative effect from the interview on their emotional state. None of the participants were found to have suffered adversely from the interview.
Data analysis
This small, in-depth study provided a rich source of data about peoples' experiences of a tragic event and in the process of collecting this data, the researchers became a vital part of the research process. On the whole, data were analysed to explore and describe patterns, themes and qualities in the responses given by participants. The purpose of analysing the small degree of numerical data, demographic data and interview content was to identify patterns distributed in the data.
To assist in this process, SPSS (Statistical Package for the Social Sciences) was used initially to enter and analyse the demographic, numeric and codable data from hand-written interview notes. Due to the small sample size and the nature of the study, descriptive statistics were used to identify the frequency and distribution of variables such as participants' ages, ethnicity, gender, geography of abode and demographic variables of the suicidees.
The purpose of analysing the content of the interview transcripts was to gain a detailed understanding of what the participants believed were important for them in the experiences they conveyed to the researchers. The data from each transcript were first read through fully by both researchers, so that they could become intimately familiar with them. To begin the process of inductive analysis, the researchers independently re-read each transcript to identify meaningful entities in the data, line by line. These entities were noted, underlined and written in coded form in the text margins. The codes emerging directly out of the participant's own words were noted in one colour and the concepts given to the ideas expressed by the researchers were written in a different colour. After independently coding several of the same transcripts in this way, the researchers made a list of all substantive codes identified and compared their interpretations of the ideas expressed by participants. This process assisted in ensuring that both researchers were achieving consistency in initial data coding. Once all transcripts were independently coded and compared for consistent interpretation, the researchers worked together to cluster similar codes and categorised them.
Codes that sat outside similarly grouped codes were analysed independently, while the substantive codes were analysed to see if they matched more than one category of response to the questions posed. In this process of constant comparison of data codes with the actual verbatim interview transcripts, it is important to ensure that the codes fit the data rather than forcing the data to fit into the codes named. Not only did the rigour of this process ensure that the intended meanings of the participant's words were interpreted as accurately as possible, it also ensured that the labelling of meanings was refined until a satisfactory system was established between the researchers. Where more than one researcher is involved in data collection and analysis in a study, it is important to ensure that consistent processes are upheld. The process of qualitative data collection and inductive analysis described is considered to be a rigorous approach in gaining meaning from the content of interviews [39–40].
While the process of constant comparison of codes and coding clusters usually extends to validating the findings with the study participants throughout the analysing process, this was not possible in the study described. However, the researchers were able to verify the participants' general meanings to the questions posed in follow-up telephone conversations. According to Strauss and Corbin, this assists the researcher in advancing the analysis [41]. In this type of research, data analysis moves away from factual reporting to conceptual understanding of the issue itself.
Methods
Sociodemographic background of people committing suicide
A total of 15 people bereaved by suicide were interviewed, 12 females and three males. Those who had committed suicide included 14 males and one female. Thirteen of the suicide victims were under 30 years of age (mean age=25 years) and lived with their parents, flatmates or de facto partners at the time of the suicide. Only two people were living alone at the time of suicide. Of the 15 suicide victims, four were students, five were unemployed and six were employed. A high proportion of the males had never married and the remainders were either married, separated or living in a de facto relationship.
Risk factors and causes of suicide
The most common method of suicide was carbon monoxide poisoning, followed by gun shot wounds and hanging. Overdose was the most common method used for previous suicide attempts. There was, however, no consistency in the method used to suicide, as only three of eight people used the same method as tried previously. The suicide was precipitated by a disturbing event in the majority of cases [11], including a relationship problem, work/study related stress and a general inability to communicate meaningfully with family and friends. Eight people had a history of self-harm, mostly within 18 months prior to the suicide. A history of mental illness, such as schizophrenia and attention deficit disorder, was reported in eight cases. Among those who did not have a history of mental illness, four had a family history of suicide, drug and alcohol problems and/or violence. Seven people who committed suicide had a past or present history of drug and/or alcohol dependency, or substance misuse, and the majority had used cannabis over a long period of time. Six victims were on prescribed medication at the time of suicide. Two of these were taking antidepressant drugs, two were taking antipsychotic drugs, one was taking sedatives and one a stimulant. Common to all suicide victims was a period of elation (lasting days or weeks) prior to the actual suicide.
Perceptions of the role of the general medical practitioner in suicide prevention and support for people associated with suicide
The majority of those who had suicided were patients of a general medical practitioner and five out of the 15 had visited their general medical practitioner during the last month of their life. According to family and friends, three people had seen their general medical practitioner for minor problems, one for a major problem and one to obtain a prescription medication in order to overdose. It was perceived by family and friends that the majority of those who had suicided did not feel comfortable talking with their doctor about their emotional problems, either due to their own reluctance to do so or to a perceived lack of interest on the part of the general medical practitioner in helping them deal with suicidal thoughts. Statements such as ‘My brother saw his GP shortly before he suicided but he would not discuss his feelings with the doctor’ or ‘My husband went to see our family GP for his sleeping problems… he did not talk to his GP but told him about his work problems…’ were recorded.
Another issue surrounding general practitioners' quality of service provision was related to short consultation periods: ‘… he always gave short consultations…in and out in a short time’.
General practitioners' lack of knowledge or interest in providing patients with information of existing counselling and support services was expressed by many participants. Responses varied from anger: ‘After my brother's suicide I went to visit my GP…. He didn't have any information…. He gave me the wrong phone number…. I had to find out about counselling services from the director’, to disappointment: ‘…next time I went to see him, he did not even mention my depression or my brother…. I lost faith in him’. Some expressed feelings of disbelief toward their general practitioners' lack of interest in supporting them after their tragedy: ‘After he suicided I went to see our GP and he just gave me sedatives… no mention of any counselling or support services that I could use’.
Awareness and effectiveness of support services
According to study participants, they and the majority of those completing suicide, had some knowledge of the availability of support services, but four of the victims did not use support services. In these cases, their relatives perceived the suicide to have been impulsive. This information was unknown in two cases. Government/public counselling services, such as hospital counselling and community mental health services, were utilised by five suicide victims. Non-government services were used by one, two others used both government and non-government organisations (NGO) and six people did not use any counselling or hospital services (Figure 1). When asked about the effectiveness of service provision, seven out of eight participants who reported the use of any services before or at the time of suicide, believed that they were inadequate and that follow-up services were lacking. In general, issues related to assessment, management, follow-up, community education and quality of counselling services were raised.
Suicide victims' use of existing services before or at the time of crisis according to their family and friends (n=15). NGO, non-government organisations.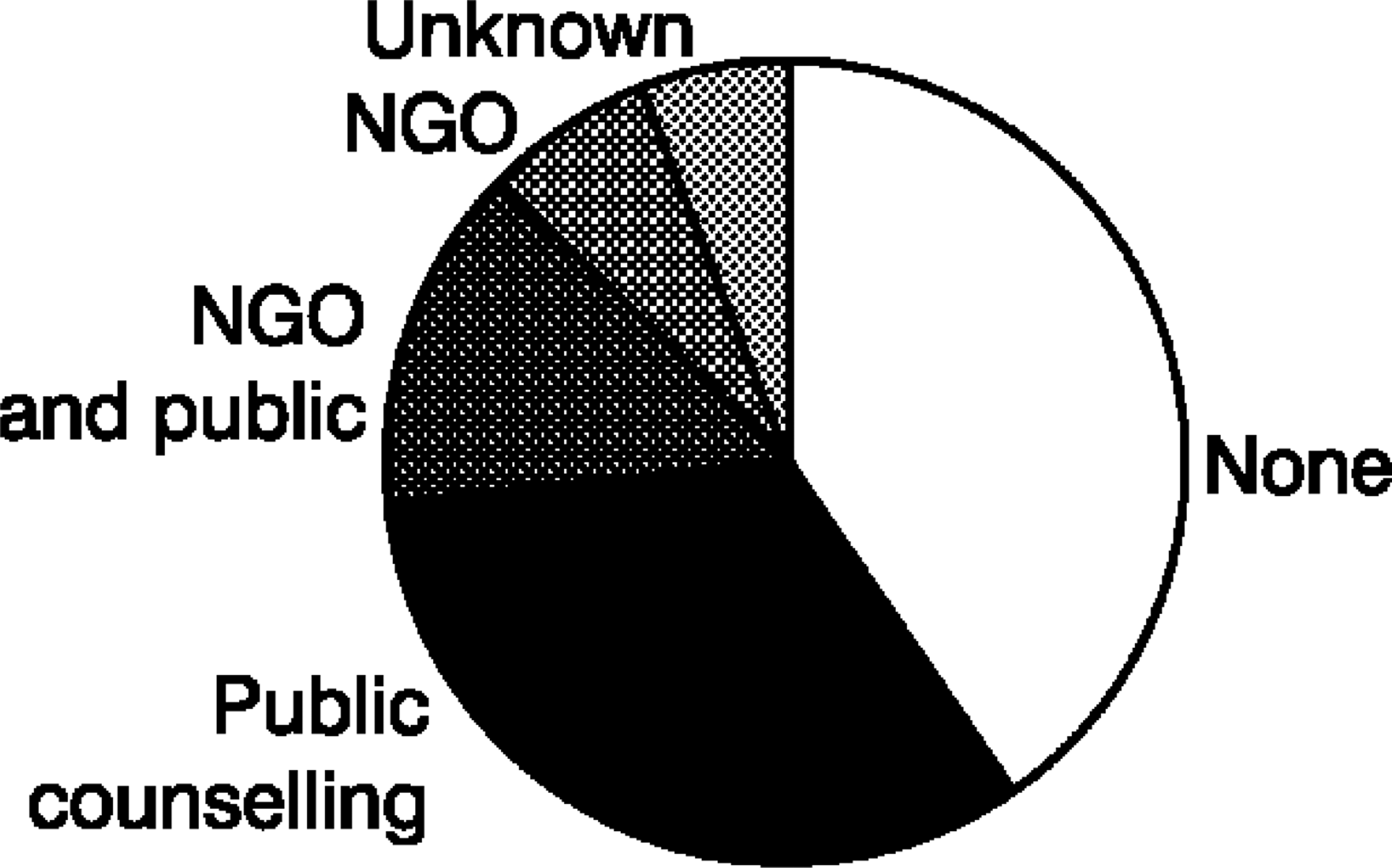
Lack of appropriate hospital management of people with suicidal behaviour was raised by most participants. One young girl was outraged by the lack of proper assessment and management of her suicidal boyfriend. She explained:
My boyfriend took 70 tablets (his second attempt) and was admitted to a major teaching hospital. The hospital psychiatrist spent only half an hour with him. He told the psychiatrist that he did it because of pain… he lied to the hospital. The psychiatrist said that he should go to the pain clinic. The psychiatrist did not diagnose that he was schizophrenic… no follow-up, no nothing… he was admitted to this hospital for overdose and he escaped…. They were more worried about me than him…. They put me down.
The mother of a young boy who was addicted to drugs and eventually committed suicide suggested: ‘He should have been admitted when he felt suicidal a few months ago, instead he was given medications…he was not followed up’. The majority of participants expressed great concern about inadequate follow-up after discharge from hospital.
The following quote is also one example of an extreme situation where there was a perceived lack of concern and appropriate healthcare support, including assessment, management and follow-up, for the person with suicidal behaviour:
My 16-year-old son took pills to overdose 9 months before this and we took him to a hospital. They kept him for a couple of hours and sent him home and never contacted him. They did not even let his general practitioner know about this.
A mother angrily expressed her experience with the hospital's lack of follow-up: ‘After my son went to this hospital casualty for overdose, they did not bother sending a letter to his GP… nothing….no follow-up’.
Some participants noted that the length of counselling provided was inadequate: ‘She was disappointed with her counsellor so she did not go to see him…the services are not effective…they do not give you enough time…when you are in crisis you should be given as long as you may need’.
Other issues raised by some participants included health services' lack of communication with family members: ‘He had an attempt a year before his death. He was admitted to a hospital. Nobody contacted us… !’.
Other issues raised were to do with the lack of community education about risks associated with suicide, how to manage or help people at risk and where to go for help were raised: ‘How come I have never heard about suicide before… is it because it was not a problem before?’.
Major concerns were also raised about the type of information provided to survivors of suicide and the level of education about the contributing factors of suicide.
Based on one mother's description of her son's behaviour, it appeared that he was schizophrenic (his father was also schizophrenic and there was a family history of suicidal behaviour). However, there was no definitive diagnosis of a mental health problem for the boy. The mother was given no information about her son's possible causes of suicide and she was left feeling confused and extremely guilty, thinking that she had caused her son to end his life:
Maybe I caused him to suicide because I insisted he continue school, and finish high school…. Do you think he had a mental illness?!…. Maybe he was gay?
When asked about non-government organisations and their efficiency in delivering quality services, some responses were positive:, ‘… there are some support groups that are good…but let people know about them’. Others were negative. For example, telephone counselling services were perceived as inadequate in providing prompt services to suicidal people in need: ‘I needed help for me and so I contacted Life Line and was put on hold for 20 minutes’.
Clearly, the memory of government and some nongovernment services available to suicide victims, their family and friends was largely negative.
Preventative support strategies suggested by participants
Although some of the participants stressed the importance of striving to uphold family values and family cohesion as major factors in altering the current trend in suicide, the majority of people believed that a more proactive education program for the community was needed. Use of posters in doctors' surgeries and other public places, as well as upgraded media campaigns, were suggested as ways of educating people about risk factors related to suicide: ‘I think we need more advertising about services… maybe through TV… poster in GP's surgery, telling people where to get help’.
Moreover, it was emphasised by the participants to utilise all existing avenues in providing information to those who are at a higher risk of suicide, such as survivors of suicide: ‘It would be good for funeral directors to give information to family and friends of survivors’. Raising awareness of the public in relation to risks involved in substance misuse and suicide was another message conveyed by the group.
There were some suggestions to involve community members in youth suicide prevention initiatives: ‘I think we should have volunteer groups… maybe older people to talk to these kids and bond with them’.
It was also imperative, from the participants' point of view, that health professionals should communicate with family members: ‘they should involve family… contact us… tell us… we may be able to help’.
Other strong views related to enhancing the support for people presenting at or admitted to hospitals and clinics with self-harm behaviour. The following quotes illustrate some of the thoughts of the study participants about the current situation and the preventative support strategies needed.
Not effective, not enough time given to people… more personalised approach is needed!
It would have been good if the GP could have referred him to counselling services or something.
Discussion
The main purpose of this study was to consider the experiences of people seeking healthcare support prior to suicide, from the perspective of their families and close friends. Very little research of this sort has been conducted, therefore the findings from this study offer healthcare workers a different view on the needs of people at risk of suicide. Although the findings are limited by the characteristics of the sample, the lack of data about the clinicians visited and healthcare services used by the suicidees and the sample selection process, the stories of these people move us closer to a clearer understanding of what is going on in the minds of people at risk of suicide and the sort of healthcare support they need. Again, even though the researchers were unable to gain first-hand information about the interactions between the suicidees and healthcare workers, the perceptions of family and close friends about the effect that these encounters had on the suicidees are important to consider.
Data analysis suggests that for the participants there was a perception of dissonance between support service delivery and service need. The themes which emerge include the participants' frustration and anger with different health services, disillusionment in encounters with different healthcare workers, suggestions for improving service delivery and increasing public awareness of different approaches available to them in suicide prevention. It became clear throughout the data collection and analysis stages that the participants believed their own needs had been ignored by healthcare staff at a time that they and the suicidal person were desperate for advice and support. This finding is supported by the literature reviewed, which explains these poor encounters in terms of the difficulty in making a clear diagnosis and, therefore, treatment for the presenting symptoms, the degree of confidence and experience of the attending clinician and the severity of presenting symptoms [29, [30], [33], [34]].
Further, participants believed that their own experiences and insights into the needs of the suicidee were not accepted by healthcare staff when offered. In view of recent strategies by government to improve family access to information support, these findings need to be considered in improving service delivery. The results acknowledge the observations by Durkheim, that social problems like suicide need to be analysed within the social circumstances in which they occur and not simply as an end product [19]. In this case, the whole dynamics surrounding the suicide and the time leading up to it, need to be considered within the construct of family and friendship networks.
As stressed in the literature, this study identifies the links between suicide, social stress, vulnerability and support for this group [1]. [4], [5], [6], [7], [8], [9]]. This was found to be combined with an emphasis on the significance of social support in the lives of those associated with suicide. The level of adversity, the presence of stressful events, social vulnerability, mental illness and individual management of stress, including drug abuse, all contribute to explaining the incidence of suicide in this study. Where social networks and healthcare interventions were considered negative, inadequate or absent, there was no effective buffer against the threatening life events which pushed the individual toward some form of mental disorder, emotional distress and eventually suicide. Research in England and Wales on suicide supports this finding for people of all ages and social situations [7]. Many people who go on to commit suicide feel their situation is hopeless and that if any social support systems do exist for them, they are of a transitory nature.
Analysis of the perceived poor quality of healthcare supports for those contemplating suicide, as well as for their family and close friends, reveals two main areas or concern. The first focuses on the way in which the participants interpreted their own position in this situation. For participants, their association with a loved one contemplating or committing suicide placed them in a tenuous position of not knowing how to give help or how to secure help. The sometimes negative and unhelpful service given to family, friends and those contemplating suicide acknowledges this sense of powerlessness, evidenced by descriptions of not being able to find anyone who would take suicidal behaviours seriously and lack of referral or follow-up support when the person was discharged from hospital prematurely. The literature supports this finding [28–30, 33, 34] and recommends that family and friends need to be included in aspects of assessment and treatment, in order to facilitate better continuity of follow-up care [34].
The second area of concern is associated with this, in the form of discrimination and deprivation. Clearly, the experiences of participants in this study tend to support Rutz et al. and Swedner's theses, that social problems like suicide exist when people do not have access to the right kind, or degree, of social support systems and this includes appropriate health and follow-up services [20–21]. In the minds of study participants, the suicidees did not receive the kinds of services that they believed would help prevent the suicide. The literature supports this reality and explains, in particular, the poor attention received by those at risk of suicide who had a history of mental illness and/or drug abuse [10, [13], [25], [26], [33], [34]]. A high proportion of the suicidees took cannabis and/or other drugs, therefore it is possible that this behaviour may have influenced healthcare workers' responses to the suicidees, a finding supported by Rutz et al. [20]. The literature suggests that aggressive, anxious or depressive behaviours displayed by at-risk patients, as well as poor compliance with prescribed treatment regimes, tend to distance clinicians from the patient, particularly where the clinician is less experienced or confidant in dealing with psychiatric symptoms [30, [32], [33], [35]].
In the opinion of study participants, cries for help were ignored and individuals at risk of suicide were marginalised by healthcare staff because they displayed negative and often self-destructive behaviours. These actions by healthcare staff effectively separated the patient and people close to them from health support systems and their primary social community. The outcome of this, as demonstrated in the study's findings, is an exclusion from society's positive symbols of self-worth and belonging. This finding supports the work of Birtchnell, who found that negative attitudes of healthcare workers towards suicide ideation and their inability to correct these tendencies, prevented them from developing an effective therapeutic relationship with the person [28–35]. In turn, perceptions of healthcare services tended to be negative for the patient and their family when the healthcare worker held such views. Durkheim's important work on suicide across all social strata also needs to be heeded: that marginalisation by healthcare workers of the kind found in this study produces a variety of emotional and mental disorders for the person at risk and in some cases, leads to suicide or self-harm [19].
Analysis of the experiences of the study participants shows without a doubt, that on many occasions the healthcare system failed to deliver the support and advice that they believed they and the suicidee needed. It appears at the time of this research that family and friends perceived very few resources had been invested in the prevention of suicide and that much of the support that was given was inadequate. The practice of giving medication without thorough assessment of the social, emotional and physical health of the individual can, therefore, be considered problematic and is supported by previous research [30]. At the time that this research took place, there was no concerted and unified approach by governments to give information and support to individuals or families, which needs to be considered when comparing the results of this study with future research. Participants also perceived at this time that mass media techniques had a far greater impact on informing the public about the factors associated with suicide than did clinical encounters between health-care staff and those at risk of suicide. The information that suicidees and families received from health services was generally inadequate and often absent.
This lack of information was one example that participants felt illustrated a lack of genuine concern or commitment to the person at risk of suicide and also to them. It appears that there was very little discussion between suicidees, families, close friends and healthcare staff about suicide ideation and prevention strategies. While it might be considered that the introduction of the family resource kit and other preventative strategies may improve communication between the public and health service providers, it is important that evaluation of recent initiatives include the experiences of potential suicidees, their family and close friends with seeking information and support.
The final question arising from analysis of the study results is whether healthcare workers regard themselves as agents of social sanction, in terms of their responses to those seeking help who are drug users and/or do not comply with prescribed treatment regimes, or whether they act as the protectors of these vulnerable and socially isolated individuals. This question was raised by Vassilos and Morgan in Britain, who came no closer to resolving this dilemma than we in Australia [31], as the attitude adopted by staff depended very much upon their own personal ethical beliefs and experiences with people at risk of suicide.
In the present social environment, where traditional supports of family and community are in a stage of decline, there appears to be dissonance in beliefs about what healthcare supports are available, who has access to services and what forms these will take. This dissonance is characterised in the study by the discourse of participants' complaints about the services they utilised and by a dynamic of exclusion that they experienced from health care staff. The fact that these negative memories remained in their experiences for some time following the death of their loved one, is a powerful testimony to their feelings of helplessness and vulnerability at a time of crisis. Clearly, families and close friends are also in need of much more support in a situation like this.
Analysing their discourse of complaints about the lack of support they and their loved one received and identifying the ways in which they were denied information and advice from healthcare staff, provides researchers with issues for further work in the area of suicide. The acknowledgement by Government that suicide is a multifactorial phenomena, demanding multilevel approaches, is evidenced by the recent launching of the variety of self-help and information packages aimed at individuals, families and healthcare staff in a broad range of healthcare contexts [2, [28], [7], [38]].
Conclusion
In conclusion, on the basis of this small qualitative study, the suggestions offered by participants include the following strategies to help prevent negative experiences for people at risk of suicide, their family and close friends: ensure that all cases of self-inflicted injuries are assessed by a mental health care professional before discharge; follow up all cases of self-harm behaviour presenting to hospital emergency departments and refer patients to appropriate clinicians for further assessment and treatment; improve assessment procedures, healthcare supports and management strategies for people presenting with suicidal behaviour; improve follow-up arrangements for people with suicidal behaviour who present to the hospitals; refer the family/caregivers of the suicidal person to relevant services for follow-up support; educate parents and the community generally about the risk factors associated with suicide and ways to address them; educate general medical practitioners and other healthcare staff working in a variety of settings about identifying the risk factors associated with suicide; and encourage their participation and interest in supporting people affected by suicide.
Essentially, the social problem of suicide is not simply a matter of treating the individual's symptoms of distress prior to the event, without a commitment to providing adequate referral and support for the person, for suicide affects all others closely associated with it. It can no longer be treated in a reductionist way.
Footnotes
Acknowledgements
We thank Mr Tony Humphrey of SPERANZA and staff of Compassionate Friends who assisted us in recruiting participants. Staff of Triple J Radio were also helpful in broadcasting the message, advertising the study and asking for participation of those affected by suicide. We thank Lorraine Young and Sandra Gifford for their valuable comments, and the staff of the Prince of Wales Medical Library for their help in obtaining literature. We are also grateful to Patrizia Fiorillo for her help in designing the questionnaire and Associate Professor Ferson for his encouragement.