
Abstract
In Australia, recent changes to Medicare and, in particular, the controversy over Medicare Item 319 have focused attention on the place of psychotherapy within mental health services [1]. This paper describes work commissioned by Birmingham Health Authority (BHA), and carried out by a Psychological Therapies Task Group to balance the provision of pharmacotherapy and psychotherapy for patients in Birmingham. This paper outlines the processes undertaken, highlights the lessons learned and discusses how this might be undertaken in Australia.
Background
In Britain, psychotherapy is largely provided within the National Health Service (NHS) and is therefore paid for through general taxation, rather than Medicare or private health insurance. As with other healthcare services in the UK, there has been growing demand for, and subsequent pressure on, psychotherapy providers, as shown by increasing waiting lists for many kinds of psychological therapies within the NHS.
Birmingham Health Authority is the largest health authority in England and Wales and commissions services for a population of just under one million. The Psychological Therapies Task Group contained representatives of purchasers, providers, voluntary agencies, social services and patients in the city.
This paper only considers the most common conditions for which adults are referred for psychotherapy in the NHS: namely, depression, anxiety and related conditions. It does not include services for psychosis, eating disorders or personality disorders.
Definition
A recent review of psychotherapy services within the NHS in England defined psychotherapy as: ‘all systematic psychotherapeutic interventions, aiming to ameliorate mental health problems, which are delivered in primary, secondary or tertiary care’ [2].
The NHS review of psychotherapy divides interventions into types A, B and C [2].
Type A
This is psychological treatment that is an integral component of mental health care. This describes a wide range of interventions offered within generic mental health services as well as general practice and general hospital settings.
Types B and C
These cover free-standing and complete interventions that are offered in the form of a series of set sessions following an assessment that generates a therapeutic plan. Type B therapy is ‘eclectic’ in that it is informed by more than one therapeutic framework. It includes non-directive counselling and psychotherapeutic work that uses a range of techniques to address patients' problems. Because of the eclectic nature of the interventions, there is little in the way of formal evidence for the efficacy of these treatments other than the fact that non-specific factors account for much of the improvement in patients. Type C therapies represent the formal psychotherapies with well-developed theories and an established scientific literature. In controlled trials, many have been shown to significantly improve outcome.
Although this framework has limitations, it includes a wider range of activities than specialist or individual analytical psychotherapy in tertiary settings. Since it is widely employed in Great Britain, the Task Group adopted this classification. Type B and Type C psychotherapies form the focus of the present paper.
Development process
The aim of the work described in this paper was to develop and implement a strategy for psychotherapy services in Birmingham using the following interrelated methods: (i) establishing the need for psychotherapy in Birmingham and the implications for service delivery; (ii) reviewing the evidence for psychotherapy including summaries of treatment effectiveness and a systematic search of the scientific literature; (iii) developing guidelines using a framework called Getting Research into Practice (GRiP), a technique of implementing research findings from the scientific literature into practice [3]; and (iv) establishing the Integrated Therapeutic Algorithm (ITA) as the model for local implementation.
Establishing the need for psychotherapy services
Anumber of issues were considered when assessing the need for psychological therapies: the potential need; the style of service delivery; and the feasibility and cost effectiveness of options considered. Health Needs Assessment (HNA) involves the comparison of expected need derived from epidemiological data, with actual health service provision and use. Equity of access to services is also included.
1. Estimating prevalence through epidemiological data
Prevalence of psychiatric disorders in the West Midlands, England and Great Britain
For Birmingham's population, this would give a total of 93 214 cases that might potentially benefit from access to psychotherapy. In practice, need is not solely dependent on the prevalence of a specific psychiatric condition, but is also dependent on severity, referral practices, and available resources. Work from America [5] suggests that less than 25% of patients with an appropriate diagnosable psychiatric disorder actually present for psychotherapy (giving a total for Birmingham of 2.4% of the population). In Britain, the estimate of the need for psychotherapy among adults in an inner city area of South London is even lower at 0.6% [5]. This would translate into a figure of 5765 for Birmingham, although it is important to acknowledge that the London estimation is based on an extrapolation from an individual general practice of 7000 [6].
2. Current service provision
Although there are a number of facilities in the voluntary or independent sector that provide psychological therapies, most specialist psychotherapies in Birmingham are provided by two NHS hospitals, as well as counsellors based in primary care. Statistics from the two hospitals were difficult to obtain as different means of recording were used, and the information was available with varying degrees of ease. However, approximately 1500 new patients were seen annually. These figures may reflect a number of factors as well as level of need, including referral practices, availability and geographical proximity of services, and patient demand.
Percentage of assessed referrals in each ICD-10 category [7]
Within primary care, there were counsellors with varying levels of expertise and training, as well as clinical psychologists undertaking Type B therapy [8]. A survey by the Primary Care Development Team of the Health Authority in 1995 indicated that at least 60 practices in Birmingham wished greater access to counselling in primary care. Actual service provision was more difficult to quantify, as the majority of counsellors were not directly funded by Health Authority contracts, and therefore no information about any of these categories was held at district level.
Although these figures do not include psychotherapy undertaken within mainstream psychiatric services, or in primary care by psychiatrists and other health care professionals, it was unlikely that potential need (estimated n == 5765) could be met simply by increasing the number of face-to-face consultations (n == 1500 new cases per year as far as it could be determined from the available data).
In addition, the NHS Strategic Review of Psychotherapy highlighted that access should not depend on factors such as place of residence, socioeconomic status, ethnicity or age [2]. Balarjan and Raleigh have extensively reviewed the specific needs of individuals from black and minority ethnic communities in relation to mental health [9]. In particular, there appeared to be over-representation in patients admitted for psychiatric disorder under the Mental Health Act, among those of African–Caribbean origin, and under-representation among those attending general practitioners (GPs) for anxiety and depression, as well as patients of specialist psychotherapy services [9].
What should be provided in Birmingham?
In considering the type of service provision for Birmingham, the Task Group adopted a set of principles derived from national and local reports on the provision of psychotherapy services such as the NHS Strategic Review [2], and the Medical Audit Advisory Group of Camden and Islington [10]. These principles are outlined below.
In terms of commissioning, the Task Group determined that priorities should be set on the basis of research evidence supplemented, where appropriate, by expert opinion. In addition, the most cost-effective treatment should be used where appropriate, and where evidence for efficacy was equal. As most medical treatments are much less time-consuming than psychotherapy and have equal efficacy, these should be considered first while allowing for the possibility of the psychotherapeutic approach concurrently or at a later date [11].
Interventions should be targeted on the basis of objective criteria to ensure that patients are referred for the appropriate level and intensity of psychological intervention using the full range of available services. Accordingly, there should be clearly understood and explicit tiers of service with locally agreed guidelines for referral between levels. Equally, psychotherapy services in Birmingham should be comprehensive and offer a range of alternative interventions for patients when a first-line therapy may not be suitable.
Finally, services should be coordinated with collaborative working between specialist psychotherapy services, and health professionals in primary and secondary care. This would include supervision, and consultation–liaison work to ensure greater access to psychotherapy for all residents of Birmingham.
Which sort of therapy is appropriate?
Anumber of sources were reviewed. These included summaries of treatment effectiveness such as the NHS Review and retrieved articles, identified as examining determinants of treatment outcome, from a search of the literature on psychotherapy from 1972 onwards using Medline, Index Medicus and other bibliographic databases. Although there have been a large number of systemic reviews, particular attention was paid to studies which had standardised inclusion criteria, well described interventions, random allocation to treatment and control groups, and excluded the effect of concomitant interventions [12, [13], [14], [15]].
Six factors in the choice of therapy were identified from the literature, a summary of which now follows:
1. Characteristics of the therapy
There has been a greater emphasis on brief and focused forms of therapy, and the development of integrative techniques that incorporate methods from a variety of psychotherapeutic schools. Integrative techniques are underpinned by evidence that brief interventions are at least as effective as long-term psychotherapy, and the development of detailed treatment packages for specific psychiatric conditions (termed ‘manualisation’). The findings are discussed later in this paper. These therapies include brief dynamic psychotherapy (BDP) [16], interpersonal therapy (IPT) [17], dialectical behavioural therapy (DBT) [18] and cognitive–analytical therapy (CAT) [19]
Approximately 66% of therapeutic gain occurs in the first 25 sessions [20], and more recent work suggests that in all but the most severe cases of anxiety or depression, 16 sessions of cognitive behavioural therapy showed no advantage over half that number [21, [22]].
2. Therapist skill and adherence to treatment guidelines specific to a school of psychotherapy including the issue of ‘manualisation’
As important as the school of psychotherapy, appears to be the skill of a therapist in the particular method chosen. A good outcome appears to depend on a complex mixture of adherence to treatment guidelines, therapist integrity, level of therapeutic experience, and skill and delivery of that particular therapy [23].
A related topic is the issue of ‘manualisation’. This refers to the development of detailed treatment packages for specific conditions, and is related to the integrative therapies described previously. Adherence to a treatment manual and the ability to deviate from or modify standard techniques when required are probably associated with good outcomes, as compared to poor adherence and rigidity in practice [23].
3. Characteristics of the problem
There has been a growing emphasis on matching specific techniques to individual diagnoses (‘specificity’). This is because meta-analytic studies consistently show that although psychotherapeutic treatments produce overall effects that are equivalent to antidepressant medication, there is variation between different forms of psychotherapy [24, [25], [26], [27], [28]].
These studies have suggested that structured behavioural and cognitive therapies have greater efficacy than dynamic and humanistic approaches. However, the advantages do not always reach statistical significance and many studies are of short-term therapy, where focused and structured approaches might be expected to show an advantage [11].
More recently, research has laid greater emphasis on matching specific techniques to individual diagnosis, rather than measuring the effect of one school of psychotherapy versus another. The development of ‘manualisation’ has meant that psychotherapy treatment packages have now been designed for a variety of psychiatric illnesses [23]. Many of these are explicitly integrative in the sense of combining drug treatment with psychotherapy, or mixing cognitive behavioural techniques with psychodynamic approaches for longer-term difficulties.
In the case of depression, several large well-conducted research trials support the efficacy of the structured ‘manualised’ therapies for depression, in particular interpersonal psychotherapy and cognitive– behavioural therapy (CBT) [29], The most recent meta-analysis, incorporating studies which used an ‘intention to treat’ and pill-placebo controls, found response rates of just over 50% for cognitive therapy, behavioural therapy and treatment with anti-depressants [15, [20]]. Brief dynamic psychotherapy was less effective with a response rate of 35% [15, [20]].
The additional health gain in offering psychotherapy in addition to antidepressants has still not been definitively established, and economic factors in choosing between antidepressants and psychotherapy may be of relevance. Combined pharmacotherapy and CBT has been associated with faster recovery, and improved outcome in terms of concomitant anxiety and somatic symptoms [13]. Blackburn et al. also reported lower rates of relapse than either treatment alone [30]. Although most patients maintained improvement at 6 months' follow-up, 30% of subjects relapsed in the medication-only group compared to 6% in the CBT group and none in the combined treatment group. However, the response to medication in this study was less than would be expected from placebo [13].
Cognitive–behavioural therapy has also been found to be effective in a number of anxiety disorders such as generalised anxiety disorders, panic disorder, phobias, obsessive–compulsive disorder and post-traumatic stress disorder [2, [23], [28], [31]]. Marks and O'Sullivan highlighted the need for including exposure to the feared situation in interventions for agoraphobia and obsessive–compulsive disorder [32]. There is also evidence for the benefit of treatments combining the use of antidepressants and psychological interventions [2, [28], [33]].
The severity, chronicity and complexity of the presenting problem have also been identified as determining outcome [10, [15], [34], [35]]. More severely disturbed patients with multiple problems of greater than 1 year in duration need longer and more intensive psychological interventions [15, [34], [35]].
4. Characteristics of the patient
There is evidence that matching patients to their preferred treatment results in greater compliance and better outcomes [36, [37], [38]]. Other patient characteristics linked with improved outcome included an interest in self-exploration and a capacity to tolerate frustration and psychic pain [39, [40], [41]]. Patients with poor self-control may find psychodynamic psychotherapy difficult to tolerate and benefit from the more structured approach of CBT [42].
5. Choice of the appropriate tier
Tiers of psychotherapy
6. The therapy–patient match
Assessing the patient-therapy match (adapted from [11])
The development of an integrated treatment algorithm for pharmacotherapy and psychotherapy
Studies indicate that the process of changing clinician behaviour is an interaction between the characteristics of source, message and channel of information [43, [44], [45], [46]]. Publication of results without consideration of these other factors, is a weak form of dissemination. Additional methods include feedback, participation by clinicians in bringing about change, guidelines and contractual agreements between planners and provider units. This information underpins the approach of GRiPwhich is an iterative process of literature review, consultation, audit, guideline design and contracting [3].
A suggested flow diagram for referral for psychotherapy. IPT, interpersonal therapy; CBT, cognitive–behavioural therapy; BDP, brief dynamic psychotherapy.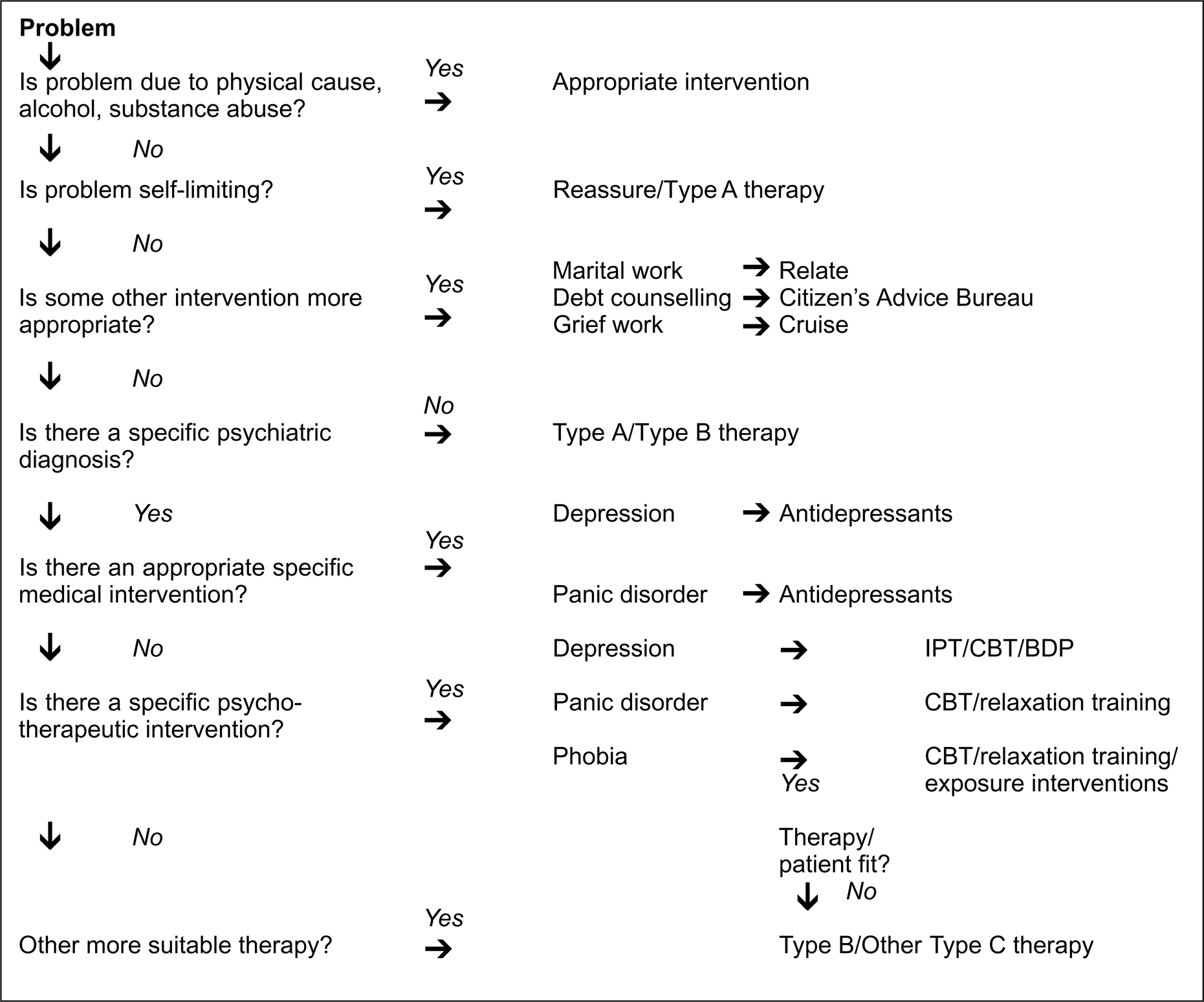
The systematic literature review, health needs assessment and audit have been covered in previous sections. The development of an integrated treatment algorithm for pharmacotherapy and psychotherapy formed the next stage of the GRiP project, using Tillet's framework [11] and the tiers of psychotherapy described in Table 3 (Fig. 1). The algorithm was designed to help GPs, clinicians and other health care professionals in primary and secondary care identify the most appropriate balance between psychotherapy and pharmacotherapy.
Additional recommendations
Additional recommendations included the development of a comprehensive guide to the full range of psychotherapy services available in Birmingham within the NHS, independent sector and voluntary agencies to include the numbers, training, qualifications, theoretical framework and supervision of counsellors and psychotherapists in primary and secondary care.
The Health Authority is also encouraging the growth of collaborative working between specialist psychotherapy services, and health professionals in primary and secondary care. Specialist psychotherapy services in one hospital trust are currently developing consultation–liaison services in primary care, and have integrated with general psychiatric services through a move to the main hospital site.
Discussion
Context of the work
This review highlighted how the existing services or workforce could not meet the demand for psychotherapy services. Ta rgeting was therefore required, so that patients were referred for the appropriate level and intensity of psychological interventions using the full range of available services, through locally agreed guidelines for referral between clearly understood and explicit tiers of service (Table 3). In addition, the Health Authority established priorities on the basis of scientific literature and expert opinion. A general principle was the use of the most cost-effective pharmacological or psychological treatment where appropriate, and where evidence for efficacy was equal. However, as another predictor of outcome was the orientation of the patient to the therapy, a range of alternative interventions was also required when a first-line therapy was not suitable.
The development of the ITA described in this paper combined research evidence, needs assessment, issues of equity, service availability and treatment effectiveness, and involved health care commissioners, providers and other interested parties in developing psychotherapy services for the residents of Birmingham. The aim was not to reduce costs, but to deploy resources in the most effective way, so as to widen access to appropriate interventions.
There are limitations to the approach described in this paper. Accurate and detailed data about the need for psychotherapy, and the services available to meet that need were incomplete. Extrapolation from general epidemiological data can be useful to quantify the presence of common problems but does not take into account other factors such as complexity, severity, chronicity and patient choice. The present work did not cover psychological treatments for schizophrenia, eating disorders and personality disorders which make important demands on psychotherapy services. There have been a number of criticisms of the application of qualitative techniques to psychotherapy. Meta-analytic studies that have shown the poorest results for psychotherapy have included a wide variety of different techniques including hypnotherapy and transactional analysis [24, [25]]. It has been argued that psychological processes in some forms of psychotherapy are too complex and individual in character to be represented by numerical variables. Psychodynamically orientated research often uses empirical, naturalistic, single case studies that do not meet the criteria for inclusion in quantitatively orientated reviews or meta-analyses such as the NHS Strategic Review of psychotherapy [2]. Finally, the efficacy of treatments conducted under highly structured conditions in specialist centres exceeds their clinical effectiveness as applied in ordinary settings [46], and few studies have evaluated the cost-effectiveness of interventions [46]. Such evidence that exists suggests that savings are only apparent in the most severe disorders through the avoidance of subsequent readmissions [46].
However, there is also a risk that some methods of treatment will be immune from public scrutiny if quantitative methodologies are not applied to psychotherapy. In addition, the ITA that was developed recognised that a preferred treatment cannot always be selected on the presenting problem alone, and that longer-term psychological therapy should be offered by specialist secondary and tertiary centres for those with severe, chronic and complex problems.
Applicability to Australia
Funding for psychotherapy services has been a controversial issue in Europe, Australia and North America. The introduction of managed care packages by health insurance or health maintenance organisations has restricted access to many forms of psychotherapy on the grounds of cost. In Britain, the situation is different, in that psychotherapy is largely paid for through general taxation within the NHS. Nevertheless, it is possible that some of the techniques described in this paper could be useful outside Britain.
As in Great Britain, there is a discrepancy between service need and provision in Australia. Although not expressly investigating the need for psychotherapy, Andrews has estimated that 25–30% of the Australian population met the criteria for a mental disorder, of whom one-third are in treatment [47].
A first step would be to gather information on all services offering psychological interventions, whether funded privately, or publicly by the States or Commonwealth. Information concerning the proportion of the population in need of psychiatric treatment is available from epidemiological studies in Canberra and Sydney [48]. Estimates of the prevalence of disorders for which psychotherapy may be appropriate are similar to those reported in Great Britain. Andrews has also demonstrated how resources for mental health services in Australia could be distributed according to illness prevalence, burden and treatment efficacy [49].
Subsequent consultation would require the participation of commissioners, hospital clinicians, private psychiatrists, and possibly health insurance organisations, including the Health Insurance Commission and the private sector. This would probably be most appropriately carried out at State level, recognising that the needs of metropolitan districts are very different from those of rural areas. Once agreed, an ITA could lead to greater integration of access to, and funding of, services. Such an ITA could also be adapted in collaboration with Divisions of General Practice to assist general practitioners in their management and referral decisions.
Unlike managed care, the development of an ITA involves consultation with all interested parties and an emphasis on broadening rather than restricting access. The present funding arrangements may not remain, and unless practitioners are willing to participate in addressing broader issues of cost-effectiveness and equity, these decisions will be taken by others and imposed on the profession. A defence of the status quo, and a refusal to engage in dialogue is unlikely to be in the best interest of patients, practitioners or the wider community.