
Abstract
Triage is the sorting of patients according to their severity of injury. It evolved during wartime, so that the greatest good could be achieved for the greatest number of patients [1]. Triage has developed in emergency medicine to direct resources to the most seriously ill. The National Triage Scale (NTS; Table 1) was developed by the Australasian College for Emergency Medicine (ACEM) for patients attending emergency departments across Australasia. It has been accepted by emergency departments in Australia and New Zealand, and a number of governments have recommended it, one (New South Wales) of which mandated its use. Criteria used to validate triage include admission rate by triage category, the use of sentinel diagnoses and their triage ‘footprints’, and deaths by triage category. The NTS was validated in a detailed nation-wide study, and is now used as a performance indicator in emergency medicine, and the Australian Council on Healthcare Standards recommends its use [2, 2, 3]].
Triage plays a pivotal role in the emergency department as well as delivering services to patients according to clinical urgency. As triage began in association with injury and illness, the scale has not included patients with mental health problems. Thus, there are no guidelines to assist emergency nurses in their triage of patients with mental health problems. With community-based care of mental health patients and less use of beds, there is pressure on emergency departments to treat more mental health patients of increasing acuity, particularly with disturbed behaviour [4, 4, 5]].
The National Triage Scale for emergency departments in Australasia
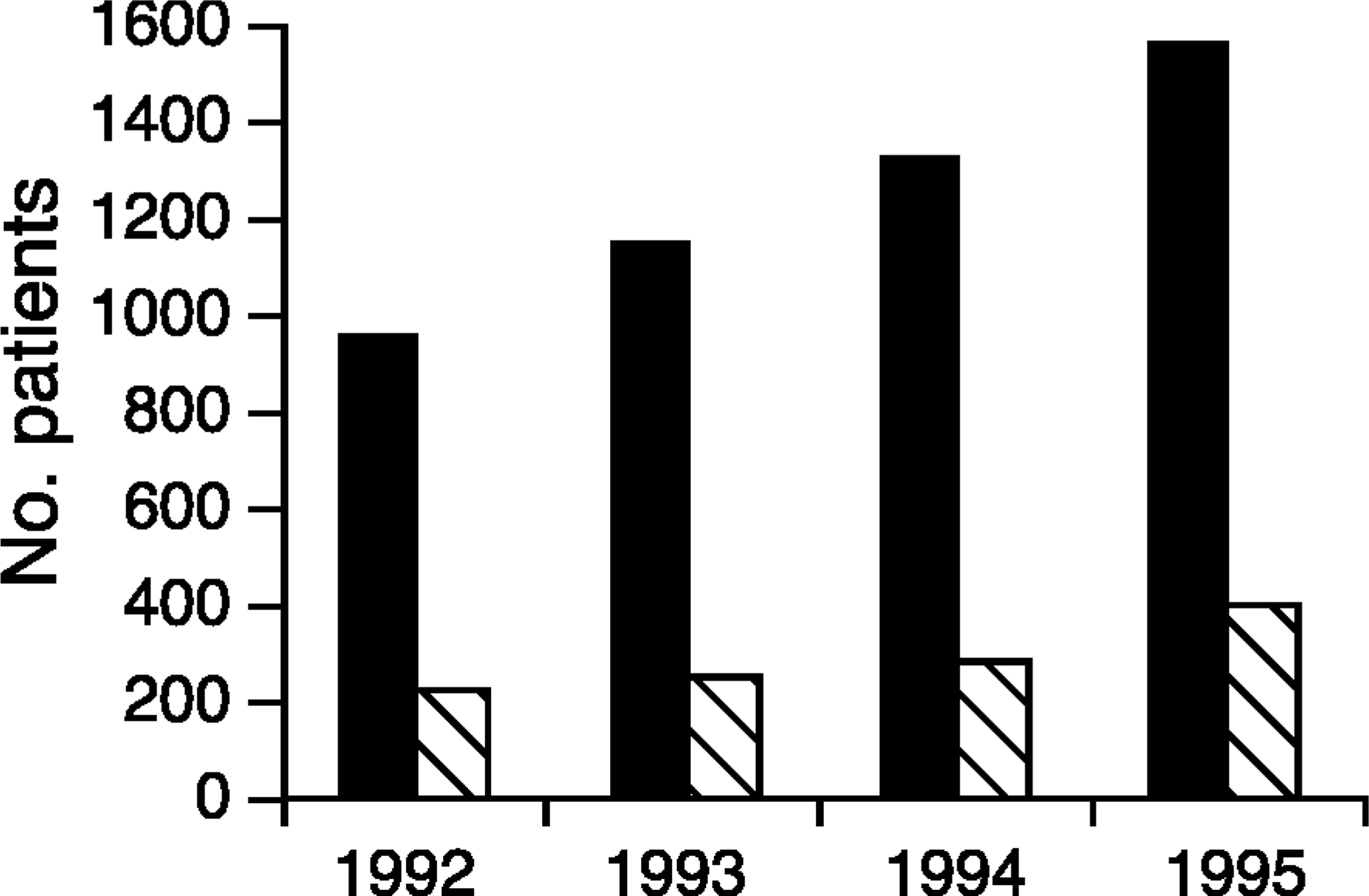
Trends in presentations of patients with mental health problems and deliberate self-harm to Royal Hobart Hospital Department of Emergency Medicine 1992–1995: ▀, mental health presentations; □, deliberate self-harm
The Department of Emergency Medicine (DEM) at the Royal Hobart Hospital (RHH) is the only 24 h service available in southern Tasmania for mental health problems and crises. Figure 1 summarises mental health attendances in DEM at RHH. There has been an increase in mental health presentations since recording commenced in 1991.
Patients with mental health problems have always been integrated into the Royal Hobart Hospital Emergency Department. With the formal implementation of the national triage scale at RHH on 1 January 1994, a need was identified for the development of a scale for triage of mental health disorders. The NTS placed emphasis on physical symptoms and signs and did not cater well for mental health patients and disturbed behaviour. This created difficulty in triaging nearly 5% of the DEM case mix. Motivating factors for the development of the mental health triage scale included a perceived unfairness in the way mental health presentations were integrated leading to delays in medical assessment and long transit times. Also, delays occurred in psychiatry attendance, which impacted on carers attending with patients, creating violence potential. This was compounded by a lack of mobile services for mental health emergencies in southern Tasmania (population 240 000).
A literature search identified few references pertaining to psychiatry or mental health triage in emergency medicine, and no references where mental health problems were triaged and integrated into a general emergency department. Most literature from North America concentrated on assessment in a dedicated psychiatric emergency service, or primary response by a psychiatry ‘triage team’ who performed a more detailed assessment of patients in the emergency department and then arranged subsequent referral without any involvement of emergency physicians [6, 6, 7]]. The term ‘triaging’ in these studies was used to define the disposition process after the patients have been more fully evaluated. Rosenweig in Minnesota (USA) outlined a similar system that did not include initial assessment by emergency physicians, and the only action performed by emergency nurses was to call the psychiatry team [8]. This is not consistent with Australasian emergency department practice where all patients are initially triaged by nurses, then assessed by emergency physicians, with referral to mental health services.
Other international models have included development of crisis triage rating scales to be applied to patients in the emergency department in an effort to determine whether or not they should be admitted [09, 9, 10]]. These scales were not developed with a view to integrating patients with mental health disorders into a general emergency department. Previous analysis of patient movement through emergency departments has shown that appropriate allocation of urgency at triage has a marked effect on total transit time [11]. Other studies of ‘psychiatric presentations’ to the emergency department have shown that these patients are the least popular with nurses, owing to educational deficiencies [02, 12], 2, 12, 13].
The need for a Mental Health Triage Scale (MHTS) which integrates with the NTS has been identified by the many patients with mental health problems attending Australasian emergency departments and was highlighted by a recent report from New South Wales [14]. The process of mental health triage is not covered in the Australian NTS user manual [15]. Structured approaches to triage of specific patient populations have demonstrated improved reliability [16].
Study aims
The aims of this study were to: (i) develop an MHTS, which integrated with the NTS for use in general emergency departments; (ii) to improve nursing assessment of patients with mental health problems; (iii) improve the effectiveness of triage of mental health presentations; (vi) reduce waiting times for mental health presentations (the time from triage until medical assessment); and (v) reduce transit times for mental health presentations (the time from triage until departure from DEM).
Methods
We undertook a pilot project to develop a scale for the triage of mental health patients. To succeed, this scale needed to be consistent with the NTS so that it could be applied easily by triage nurses. The scale accepted the particular needs of patients with mental health and psychiatric emergencies, including the level of independence of patients, and the needs of carers.
In 1993, a review of mental health services within the Royal Hobart Hospital was undertaken by Kalucy and Crowther [17]. As a result of the review, author CP (dual certificate, general and psychiatric nursing) was appointed as project officer to investigate some of its recommendations. One of CP's major findings was that triage nurses needed direction in defining urgency categories for patients with mental health problems and confirmed an urgent need for training of triage nursing staff in assessment of these patients.
The project officer developed the nursing education program and a reference booklet. She also coordinated submissions from stakeholders to develop the MHTS. This resulted from liaison between staff undertaking emergency mental health assessment: emergency nurses and doctors, liaison psychiatry staff, and nurse management. Consumer input occurred. Patients, community agencies and mental health professionals expressed concerns regarding waiting and transit times for mental health patients in DEM. We used these parameters as outcome measures.
Mental Health Triage Scale
Factors considered in assigning mental health triage categories
The MHTS was developed from ‘first principles’ to integrate patients with mental health disorders into a generalist framework. After consultations outlined above, the MHTS was agreed (Table 2). It had four categories corresponding to triage categories 2–5 on the NTS. Patients with immediately life-threatening, physical illness were triaged according to the NTS as category 1 (Table 1). Patients with deliberate self-harm (e.g. overdose or physical injury) were triaged using both medical and psychiatric information and the most urgent category applied.
Factors for the mental health categories are summarised in Table 3. The first six factors define patients with category 2 or 3 urgency. More severe disturbances led to the patient being assigned to NTS category 2 and significantly distressed patients were allocated to category 3. Triage nurses asked CP for scale validation at the time of triage. They determined if the patient was suicidal, assaultive or confused, and these three states resulted in their allocation to the higher category.
All patients received a mental health assessment by the emergency physician. Athorough physical assessment was deemed to be required for triage categories 2 and 3 (initial presentations, referrals from general practitioners and patients > 64 years), prior to consultation with liaison psychiatry. Triage category 4 and 5 patients were referred to the liaison psychiatry team after emergency mental health assessment and appropriate physical examination where deemed necessary. These also included patients discharged within 5 days from a mental health facility, and those with links to community and inpatient psychiatry. The presence of a carer mandated triaging to category 4 or more urgent because of the assistance the carer could provide. Patients who were assessed at triage but did not wait for treatment were counted as a performance indicator of the MHTS. All ‘did not wait’ patients’ histories were reviewed by the authors. Measurements of outcome for these patients included revisit to DEM within 1 week, mental health admission within 1 month, or death within 6 months (assessed by reviewing DEM and mental health records and death registers).
Once the MHTS and implementation were agreed, the next step was triage nurse education. Supervised by the project officer using the education booklet, triage education commenced. Nurses identified the presenting problem and promptly undertook an analysis categorising urgency by using the guidelines. They created a safe environment and established if life-threatening medical problems including injury, impaired cognition, seizure, overdose and medication side-effects, required immediate attention.
Nurses learned behaviour observation and wide gathering of information. They were taught interview methods, how to ascertain and report on the patient's appearance and behaviour, speech, thought content, mood and affect, perceptions and cognition. Education of DEM nursing staff included assessment of acute psychotic states, acute depression with suicidal ideation, anxiety, intoxication and situational crises.
Data was collected monthly on mental health presentations, tabulating their triage code and mean/median patient waiting times and transit times. A control sample of pre-trial data was collected for the three months prior to the implementation of the triage scale, from 1 December 1993 to 28 February 1994. The MHTS was implemented on 1 March 1994, and was completed on 31 May 1994. Data was collected during implementation and post trial for a further 3 months to 31 August 1994, measuring nursing attitudes, waiting times and transit times, admission rates for mental health presentations, numbers who did not wait for care after triage assessment, and impact on waiting and transit times for other DEM patients.
Patients were included in the study if they presented with a mental health disorder or disturbed behaviour, acute situational crises or evidence of psychiatric disturbance. National triage scale category 1 medical illness or injury was excluded. Patients with coexistent drug or alcohol intoxication were included unless they required resuscitation and were otherwise unassessable by liaison psychiatry (overdose affecting airway patency or consciousness). To assess reliability of the MHTS, the liaison psychiatry team completed a questionnaire for a sample of patients during implementation of the scale. The questionnaire included demographic information about the patient and asked the psychiatry team to retrospectively apply a triage rating and evaluate the appropriateness of the triage nurses’ assessments.
A survey at 2 years assessed utilisation of the mental health triage scale, assessing awareness of the scale, frequency of use and nurse confidence with triaging patients with mental health problems. Triage ‘footprints’ (the relative percentage of patients in each of the triage categories) for mental health presentations were also analysed as an indicator of continued use of the MHTS, comparing these with the global DEM census.
Initial sample size estimates indicated that to detect a 20% difference in waiting times at the 5% significance level, with a power of 80%, a sample size of 270 per group would be required: 3 months of mental health presentations at RHH. Data were collected directly and also by retrieval of waiting times and transit times from McDonnell-DouglasTM ‘Emerg module’ (CSC Healthcare, Sydney, Australia) and entered onto MicrosoftTM Excel Spreadsheets, and stored in MicrosoftTM Access database (Microsoft Corporation, Redmond, WA, USA). Statistical comparisons used the Mann-Whitney U-test for ranked variables, Student's t-test and Chi-squared tests, rejecting the null hypothesis at p < 0.05; defining statistical significance at this level. The kappa statistic was used to assess inter-rater reliability.
Waiting times (min) for mental health presentations for each triage category for the three phases of the study
Transit times (minutes) for mental health presentations by triage category for the three phases of the study
Results
The nurse's response to the education package and booklet was positive. Triage staff felt well equipped to deal with patients with mental health problems, and more confident in applying these triage categories, in line with the NTS.
Table 4 summarises mean and median waiting times for each triage category, for patients with mental health problems during the three phases of this study. Table 5 summarises mean and median transit times for each triage category, for patients with mental health problems during the three phases of this study. Table 6 summarises the population mean waiting and transit times, for each phase of this study, and Table 7 summarises the triage footprints for patients with mental health problems compared with the total emergency department census. Table 8 summarises outcomes for the ‘did not wait’ population.
The control sample confirmed some difficulties with service delivery to mental health patients. In the three months that the control sample was collected, there were 261 mental health presentations. The mean waiting time was 34.3 min (SD = 33.6). This compared with a mean of 26.4 min (SD = 44.2) for the whole of DEM census during the control period (t = 3.68, p = 0.0002). The median waiting times for mental health presentations ranged from 10 min to 39 min. The mean transit time was 149.2 min (SD = 101.0).
Mental health patient whole of population waiting times and transit times during the three phases of the study for all triage categories
Triage footprints for mental health presentations compared with the global emergency census (category 1 excluded)
Outcomes of the ‘did not wait’ (DNW) populations
The median transit times pretrial ranged from 83 min to 161 min. Prior to implementation of the MHTS, patients with mental heath problems had longer waiting times than other DEM patients, and were more likely to receive a lower triage category (Table 7). In addition, mental health patients had a significantly higher chance of leaving DEM without being seen by an emergency physician (did not wait). In the control sample, 7.3% (19) patients did not wait out of a total of 261. This compared with 3.7% (865) for the DEM census (9 months) of 23 121 patient attendances (χ2 = 8.90, df = 1, p = 0.003).
During implementation of the MHTS, there were a total of 306 mental health presentations. During this period the mean waiting time was reduced to 29.1 min (SD = 26.1); a statistically significant improvement (t = − 2.03, p = 0.043). Mean waiting times were reduced in all triage categories except for category 3. Median waiting times were reduced in all triage categories (see Table 4). Mean transit time was reduced to 131.8 min (SD = 77.3). This represented an improvement of 17.4 min per patient (t = − 2.28, p = 0.023); over the 306 patients, a reduction of 88.9 patient hours in the emergency department for the 3-month period. ‘Did not waits’ declined from 19/261 (7.3%) to 12/306 (3.9%).
During the post trial phase, the mental health population mean waiting time was 26.6 min (SD = 28.3), a statistically significant reduction (t = − 2.92, p = 0.004). Mean waiting times for all triage categories were lower in the post-trial sample compared with the control period. Median waiting times were also lower than the control, except for triage category 3.
Mean transit times post trial remained lower than the control period (131.7 min, SD = 86.8, t = − 2.21, p = 0.027), and were not statistically different from the implementation period (t = − 0.09, p = 0.93). Transit time reductions were most apparent in triage categories 2 and 4. Median transit times were reduced in all MHTS categories except category 5. The post-trial period had a further reduction in the number of ‘did not waits’ to 11/322 (3.4%) (χ2 = 4.41, df = 1, p = 0.036). This result was a statistically significant improvement compared with the pretrial sample, and lower than the total DEM census ‘did not waits’. There were no deaths in the ‘did not wait’ population for the three phases of the trial (Table 8). Emergency reattendances were reduced, and later admissions to mental health facilities were unchanged in the ‘did not wait’ population after implementing MHTS.
The triage footprints for mental health patients are summarized in Table 7. During implementation of the MHTS, a significant ‘up-triaging’ occurred. Mental health patients were allocated to higher urgency categories than occurred in the pretrial period. This effect persisted during the third phase of the study.
Admission rates by triage category for mental health presentations are compared with the DEM census in Fig. 2. The control sample prior to implementation of the MHTS demonstrates an inconsistent relationship between assigned triage category and the need for inpatient admission of mental health patients. Once implemented, the MHTS led to consistent relationships between assigned urgency and admission rates with greater urgency, leading to a corresponding higher chance of admission. This was also consistent with the DEM census triage code/admission relationship.
For the three phases of the study, mental health admission rates were relatively constant (53.6%, 59.4% and 53.7%), indicating that the MHTS did not influence this parameter. However, overall admission rates for mental health patients were significantly higher than other emergency patients (505/889 [56.8%] versus 6806/23121 [29.4%], p < 0.00001, test for difference between two proportions).
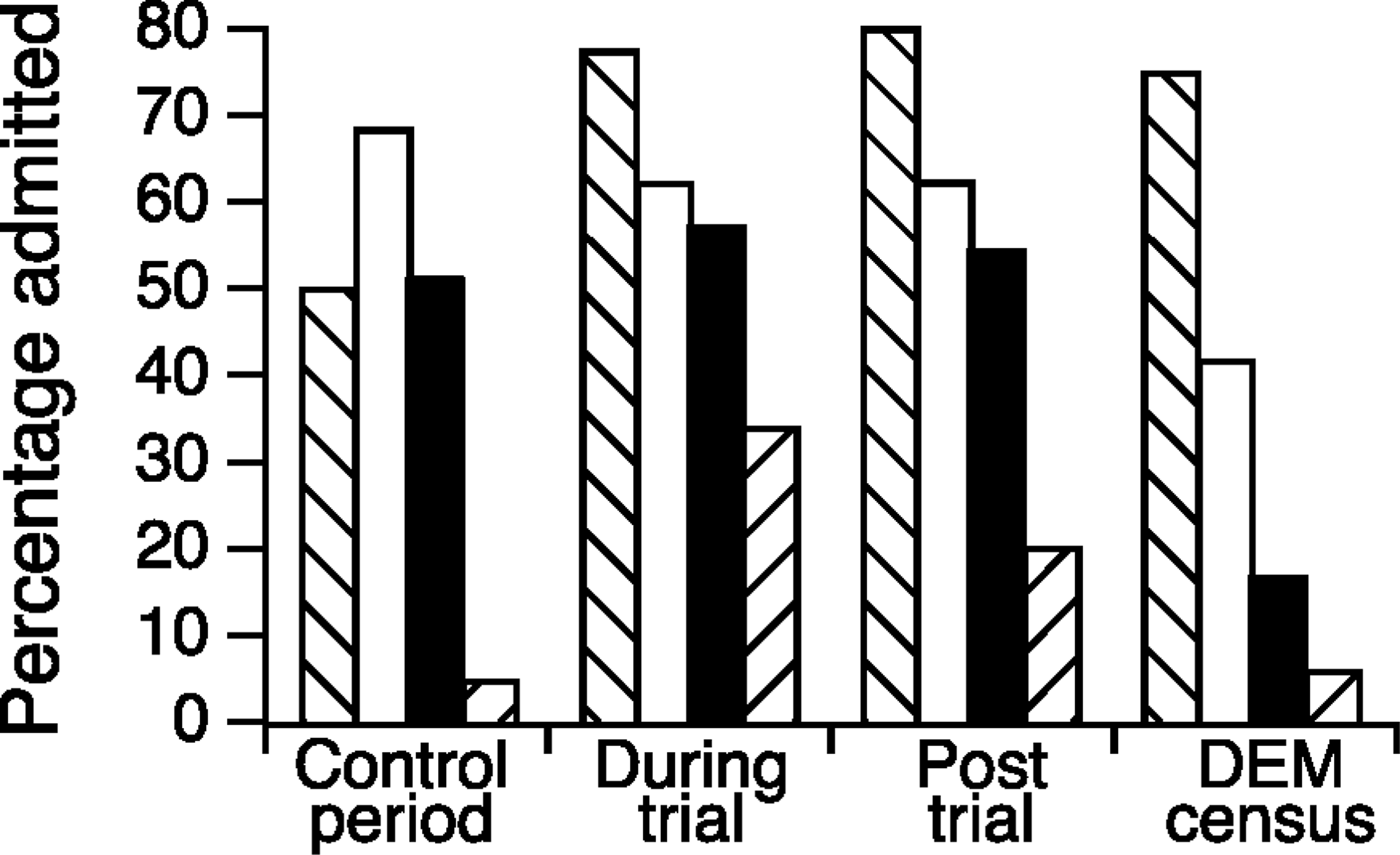
Admission rates by triage category for the three phases of the study, compared with emergency census. Triage category: □, 2; ▪, 3; ▀, 4; □, 5
The MHTS had minimal effect on service delivery to other DEM patients: waiting times and transit times for the whole DEM census were not significantly changed (p-values not significant, all triage categories, using t-test).
Liaison psychiatry staff completed 81 evaluations in a parallel retrospective review of nursing triage (Table 9). Sixty-six (81.5%) agreed with the nurses’ triage coding, five disagreed (rating the urgency one point lower), and 10 had no rating due mainly to changes in patient status. There was a high level of agreement between the triage nurse urgency ratings and those assigned by the psychiatry medical staff in this small study of inter-rater reliabilities (K = 0.89, 95% confidence intervals 0.79–0.98).
The follow up survey of nurse utilisation and attitudes to the MHTS demonstrated a high level of acceptance. Thirty-one nurses were surveyed, and 21 completed the questionnaire. Six of the non-responders were on leave. Seventeen nurses (81%) were still using the process to allocate triage categories for patients with mental health problems. Fifteen of the 17 found the scale was extremely useful. All expressed confidence in its use. At 2 years follow-up, the triage footprints for mental health patients were not significantly different from the post trial sample, (z = 0.72, p = 0.45, Mann-Whitney test). This also provided evidence of the continued use and validity of the MHTS.
Discussion
The MHTS is consistent with the national triage scale and has been validated in this study using a number of criteria: acceptance by emergency nursing staff; reduced waiting and transit times; service delivery, less patients did not wait; support for the urgency categories by liaison psychiatry medical staff; continued use of the scale at 2 years follow-up; minimal impact on other emergency patients.
A recent national analysis of the triage process demonstrated broad agreement with the MHTS guidelines outlined in Tables 2 and 3, and this provides further support for our methodology [2].
The benefits of a structured approach to mental health triage became apparent soon after implementation. Triage nurses had greater understanding of mental health presentations as a result of the education package delivered in DEM, assisted by the education booklet. They were able to systematically prioritise mental health presentations rather than relying on their previous experience. Medical staff had greater confidence in caring for mental health patients concurrent with others who were ill or injured because they were triaged consistently. The relationship between emergency department staff and liaison psychiatry staff was enhanced.
Inter-rater reliability sample. Triage categories assigned by nurses compared with psychiatry staff
The effect of the MHTS in ‘up triaging’ mental health patients relative to the whole of DEM census was expected, because admission rates for mental health patients at Royal Hobart Hospital have always been higher (57% overall) than patients with other illnesses (31%). This is consistent with data from USA [5] and reflects the relative severity of mental health problems presenting to an inner city tertiary hospital. Waiting and transit times for mental health presentations were thus reduced, and there was a more consistent relationship between allocated urgency categories and the need for inpatient admission. These parameters support the validity of the MHTS. The relationship between urgency of presentation and the need for inpatient treatment has been well established for patients with illness and injury [02, 2, 15]].
We have performed only a limited study of the reliability of the MHTS. There were several reasons for this. Liaison psychiatry staff already had input to the development of MHTS and were not applying it in a blinded manner. They retrospectively evaluated the nurses’ assigned urgency. Undertaking this activity retrospectively has limitations as illustrated by the 10 cases to which liaison psychiatry did not assign a triage category, mainly due to altered status after their arrival in DEM. There had been significant discussion between Liaison Psychiatry and DEM staff regarding assigning urgency to various case scenarios. The high level of agreement for the sample of 71 cases during MHTS implementation was expected. To perform a detailed inter-rater reliability study would require the psychiatrist to spend many hours at triage in order to witness emergency presentations of mental health patients, and assign urgency concurrent with the triage nurse. Further study of the reliability of the MHTS is required and this may be achieved by simulated scenarios as used by other authors [18].
Mental Health Triage Scale use remained high, when reviewed in November 1996, which was testimony to its effectiveness and ease of implementation. The reference book is a valuable resource and remains in use by the nursing staff. A revised booklet has been released in 1998, and is available from the authors.
There are limitations to this study. Our sample size consists of only nine months data, covering control, implementation and post trial periods. We believe the data to be representative. We have attempted to improve validity of the study by the 2-year follow-up sample. Triage footprints for mental health patients remained consistent with the post trial sample, as did admission rates by triage category.
Our only measure of patient satisfaction has been the reduction in the number of patients who ‘did not wait’. We did not undertake a direct survey of mental health patient satisfaction with the emergency department as a forum for evaluation of their health problems; however, feedback has been generally positive. Further study is needed regarding specific needs of patients with mental health problems who present to emergency departments.
Conclusions
Outcomes of this study are two-fold. First, patients with mental health problems are now addressed in a generalist framework. Mental health problems are successfully integrated with a teaching hospital emergency department. Conditions are evaluated, prioritised and patients referred to psychiatry in the same way as occurs for medicine, surgery, gynaecology and paediatrics. Second, DEM staff felt safe with acute mental health patients, once they have been appropriately triaged. Patients and their carers know their classification, know the time frame in which they are to be seen, and much of the ambiguity surrounding their presentation to the emergency department has disappeared. Nursing education led to greater professionalism, more understanding between patients and staff as to early care outcomes and better care. Psychiatry staff have developed an understanding of the perspectives and goals of emergency medicine, and know it is important to respond within the allocated time frame.
Community attitudes towards the emergency management of mental health problems have also improved, so that patients, their families and carers feel more confident about their care. This has been borne out by the progressive increase in mental health attendances to DEM at Royal Hobart Hospital over the subsequent 3 years on a background of a static DEM census. All staff felt that the development of the Mental Health Triage Scale had been a thoroughly worthwhile exercise, resulting in improved care for mental health patients, allowing us to comfortably mainstream mental health patients to the benefit of all.
Footnotes
Acknowledgements
We are grateful for the support provided with data collection by Pam McGrath (Clerical Manager, Department of Emergency Medicine, Royal Hobart Hospital) and her staff, and Mark Gaukroger (CNC DEM RHH) for advice and support.