
Abstract

Ladies and gentlemen, good afternoon. It is a great pleasure to be here and to share with you this 10th anniversary of sumatriptan, in the eternal city of Rome. When I started to engage myself in the field of migraine in paediatrics and adolescent patients, I felt similar to Reijo Salonen, like an alien, facing all these really experienced neurologists talking about pathophysiology and epidemiological issues I had never heard before. Over time I learned to manage this feeling but now, and here, standing in front of you, I can tell you it is back.
I have great pleasure in sharing with you some of the data on the paediatric and adolescent use of sumatriptan that we have gathered over the last 10 years. Migraine is a frequent, disabling headache disorder affecting 8–12% of mankind, with a marked female predominance. Based on conservative estimates, the prevalence of paediatric patients 4–16 years of age with migraine is somewhere between 5% and 8%. That means that there live at least 7.8 million children in the European Union who suffer recurrent migraine attacks — a considerable number. Recommended treatment strategies for these patients cover a broad spectrum of pharmacological and non-pharmacological alternatives (Table 1). Pharmacological approaches can be grouped into three categories: anti-emetics (such as metoclopramide or domperidone); analgesics (such as acetaminophen, ibuprofen and acetylsalicylic acid); and ergot preparations. In contrast to the adult recommendations arising from evidence-based medicine, most of the recommendations for children are based on unscientific data.
Potential strategies for the acute treatment of migraine attacks in children

I performed a literature review, searching for the key words migraine, therapy, and children, over the past 28 years. Up to February 2000, there were 10555 publications on migraine, 570 on migraine in children and 189 on migraine therapy in children. A little discrepancy! This might be one of the reasons why approximately one-third of all paediatric migraine patients—that means nearly 2.5 million children and adolescents in Europe—experience at least one migraine attack per year that is refractory to any of the pharmacological recommendations. Too many! This tricky situation has been resolved for adult migraineurs with the introduction of the triptans, shown to be effective in scores of clinical trials and clinical experience.
Over 700 papers attest to the efficacy of sumatriptan in migraine, but only 10 deal with migraine in childhood and adolescence. This discrepancy is surprising, especially if you take into account that between 50% and 90% of all migraineurs start their career as migraineurs in childhood or adolescence.
Looking at the key specifications of the ideal anti-migraine drug for paediatric migraineurs (e.g. easy to use, good social acceptance, rapid onset of action, high efficacy, high response rate, constant reliability, excellent tolerability, high compliance), the question arises, which of the different sumatriptan preparations is the ideal one for children? The answer is clear, it is the 20 mg nasal spray, for a number of reasons. I want to consider three controlled trials using the spray in young migraine patients (Tables 2–4). In the first trial, 14 children participated, six with and eight without aura. Seven were girls. The mean duration of illness was 13.5 months, the median attack duration 12 h (range 6–24 h) and the median attack frequency 3 months (range 2–5). The usual end points were employed. The rate of attacks was identical in placebo and sumatriptan subjects, as was the intensity of attacks at the time of therapy, i.e. 2.6 on a scale of 0–3. Despite the fact that all children participating in the study were rated as refractory (i.e. they had experienced migraine attacks that had not responded to at least three recommended pharmacological strategies), six responded to placebo within 2 h, highlighting one of the problems with studies in paediatric migraine patients.
Symptomatic benefits in children treated for migraine with intranasal sumatriptan: study results (Trial 1)

Symptomatic benefits in children treated for migraine with intranasal sumatriptan: study results (Trial 2)

Adverse events in adolescents treated for migraine with intranasal sumatriptan or placebo: study results (Trial 3)

Attacks treated with sumatriptan were relieved significantly more often than those treated with placebo. The sumatriptan nasal spray was also significantly more effective than placebo for associated symptoms such as vomiting or photophobia, although not nausea. All but one of the 14 children preferred sumatriptan. The therapeutic gain for sumatriptan for significant headache relief within 2 h was 43% (95% CI 34–53%). For total headache relief, the therapeutic gain was 50%, for reduction of nausea 36% and for phonophobia 57%.
To study efficacy over multiple attacks, we performed an open study (Trial 2) with the 20 mg nasal spray in 58 children ranging in age from 4.2 to 10.9 years. Twenty-eight were girls. Overall, 376 attacks were evaluated. The overall relief rates are comparable to those found in blinded controlled trials, but efficacy seems higher in younger children than in older ones, for reduction of headache, total headache relief and reduction of nausea, vomiting and photo-phonophobia. The 20 mg nasal spray worked as well in the eighth as in the first attack.
The design used in this multiple-attack efficacy study allowed us to evaluate the behaviour of the patients before, during and after their migraine attacks, using the play performance scale for children. This is a simple measure of children's play behaviour as assessed by their parents every day using special diary cards. During the 3 days preceding a migraine attack, there was increasing impairment of play behaviour, reaching the nadir on the day of the attack. Complete recovery took another 3 days. So, for children, migraines imply a period of incapacity or suffering not only on the day of the attack, but for up to 3 days before and after. Figs 1 and 2 show the typical migraine-related behavioural restrictions of the 58 children participating in Trial 2 using customary anti-migraine therapies (Fig. 1) and sumatriptan 20 mg nasal spray (Fig. 2). Comparing both treatment strategies and their influence on these behavioural problems, the post-attack convalescence period of impairment was significantly shortened by sumatriptan.

Functional capacities over days before, during and after a migraine attack, of children not treated with sumatriptan. Study results (trial 2).
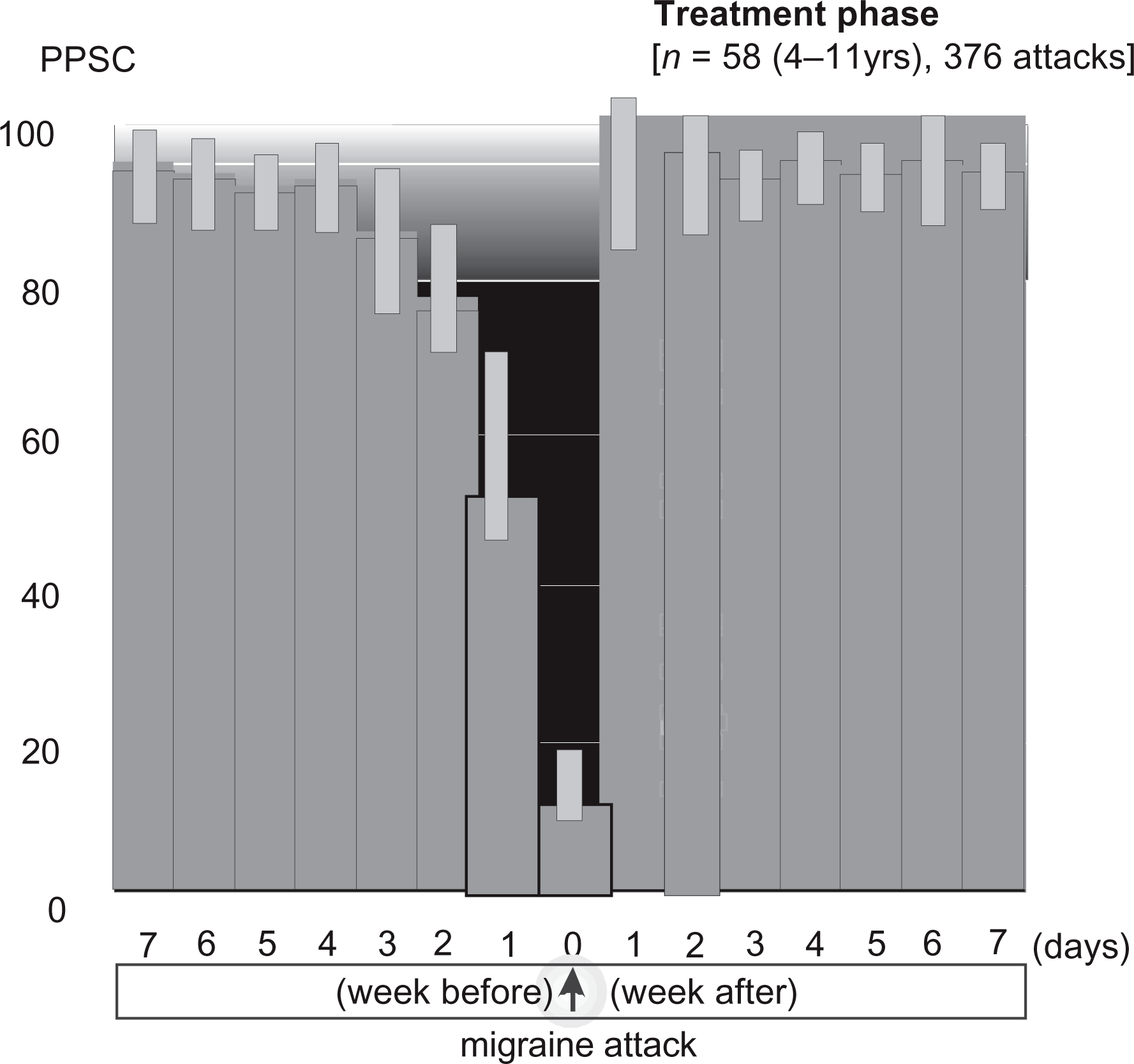
Functional capacities over days before, during and after a migraine attack, of children treated with sumatriptan intranasally. Study results (trial 2).
The Suma 3005 trial was performed in the United States in over 600 migraine patients aged 12–17 years who suffered 510 attacks of any degree of severity. The differences between placebo and the trial drug were less marked (Figs 3 and 4), the sumatriptan relief rates at 1 hour being 56% for the 10 and 20 mg doses compared with 41% for placebo. Two hours post-dose the response rates were 53% for placebo and 64% and 63% for the 10 and 20 mg doses, respectively. The response rates show that at 30 min the 10 and 20 mg doses are already providing better relief than placebo (Fig. 5). The only adverse event occurring significantly more often than with placebo was taste disturbance. Excluding this complaint, the adverse event rates were similar in the placebo- and sumatriptan-treated subjects at all three dosages.

Percentages of children obtaining headache relief at 1 h after treatment for a migraine attack with sumatriptan intranasally or with placebo. Study results (trial 3).

Percentages of children obtaining complete headache relief at 2 h after treatment for a migraine attack with sumatriptan intranasally or with placebo.

Probability of response in children obtaining headache relief at points up to 2 h after treatment of a migraine attack with sumatriptan intranasally or with placebo. Study results (trial 3). P < 0.05 for 5 mg, 10 mg and 20 mg sumatriptan vs. placebo (based on log-rank-test).
In summary, sumatriptan is the only 5-HT1B,D agonist to prove effective for the treatment of children and adolescents from 4–17 years of age. The sumatriptan 20 mg nasal spray gave better symptom relief than placebo, with a comparable adverse event profile, and it thus offers to younger children the unique opportunity to treat their migraine attacks by themselves, a basic requirement for the development of effective anti-migraine coping strategies in paediatric patients.
One critical word at the end concerns approval status. The perspective of adult migraineurs changed dramatically 10 years ago with the introduction of sumatriptan, now approved for use in adults in 97 countries for the tablets, 88 for the subcutaneous injection, 32 for the nasal spray and 13 for suppositories. Only 5% of the data on sumatriptan have been derived from studies in children, but the results are still compelling, to clinical scientists at least. Regrettably, they seem less compelling to regulators, for sumatriptan is not yet licensed for use in children in a single country in Europe or North America, in any one of its four formulations. I ask you to work in your own country to speed the approval of sumatriptan for children. They deserve it too.
Thank you very much for your attention.