
Abstract

Cluster headache is the most severe pain that can be experienced, beside trigeminal neuralgia. The pathogenesis is poorly understood but there is a relationship with circadian rhythms. Arne May, together with Peter Goadsby, has shown that functional and structural changes in the hypothalamus can be seen in patients with cluster headache (1). There are two types, episodic and chronic, as well as chronic paroxysmal hemicrania, a condition that also responds to sumatriptan and which is probably a variant of cluster headache. The usual treatments include inhalation of oxygen, ergotamine also by inhalation, DHE subcutaneously, intranasal Lidocaine (which is not very effective) and sumatriptan injections. Prophylactic medications for episodic cluster include corticosteroids, verapamil, lithium and topiramate, which is also effective for chronic cluster headache (2).
The effect of sumatriptan injections has been investigated in two placebo-controlled multicentre clinical trials (3, 4). As the 12 mg dose was no better than 6 mg, I will only talk about the latter. In migraine we consider a time axis of 1–2 h but in cluster headache 15 min is a more appropriate figure. Sumatriptan can provide relief in 10 min for a condition that does not respond well to any other treatment. The figure may be even better because the placebo effect in cluster headache is not truly a placebo effect; it is just that some attacks are very short. Using a 60-min time-scale, the ability to function improves with sumatriptan uniquely, and the associated symptoms are also diminished (Figs 1 and 2). In a second, cross-over study, pain relief was seen even at 5 min and after 15 min there was 75% improvement with sumatriptan compared with 35% from placebo (Figs 3 and 4).

Rates and times of pain relief in cluster headache in patients treated with sc. sumatriptan or placebo (Studies 1 and 2). ∗P < 0.05.
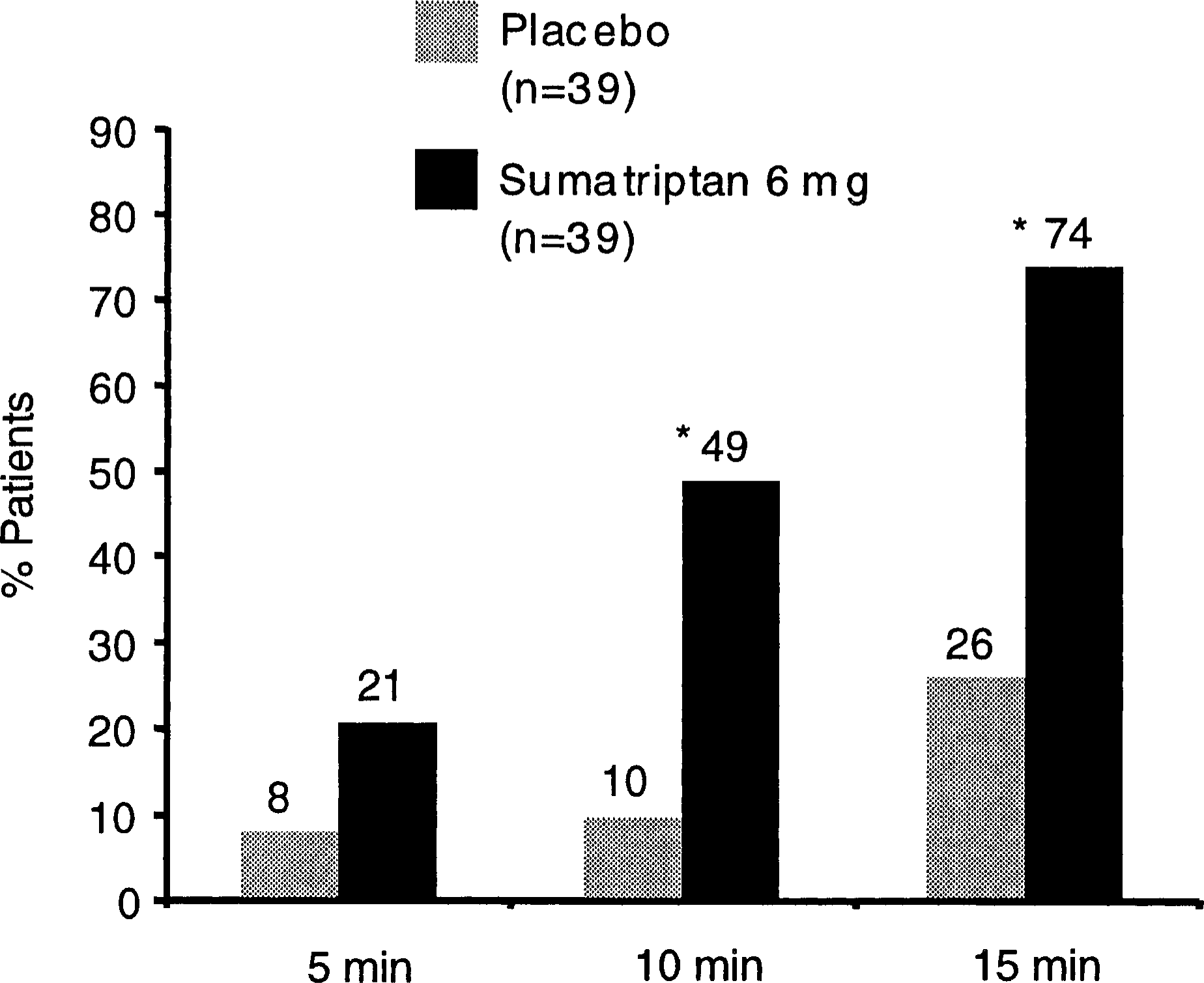
Rates of early pain relief in cluster headache treated with sc. sumatriptan and placebo (Study 1). Pain relief was defined as reduction of moderate, severe or very severe headache pain (grade 2, 3 or 4) to mild or no headache pain (grade 1 or 0). ∗P < 0.01. From Ekbom (3).

Migraine-related disability rated on a 4-point scale from able to function normally (grade 0) to severely functionally disabled (grade 3). Study 1. ∗P = 0.001; 1 P < 0.01. From Ekbom (3).

Long-term efficacy trials have shown that the effect on pain relief and pain freedom persists (5). There is no tachyphylaxis, the incidence of side-effects is lower than in migraine patients, and cluster patients do not develop drug-induced headache with sumatriptan, even if they use it three times a day for 3 years.
To conclude, the 6 mg sumatriptan injection rapidly relieves cluster headache and represents a real breakthrough in the treatment of this horrible, painful condition. It is highly effective in the acute stage with an onset of effect within 10 min and it does not interact with the prophylactic medications usually given.