
Abstract
Objective:
The purpose of the study was to implement a comprehensive adverse childhood experiences (ACEs) screening protocol in a rural Integrated Primary Care Clinic serving Latino Children utilizing implementation science as a framework.
Methods:
The Exploration, Preparation, Implementation, Sustainment (EPIS) framework was utilized to guide and evaluate the implementation. There were 2,347 children who were screened with the developed protocol which included screening for ACEs, psychosocial problems, adolescent depression, and parental depression. Several implementation outcomes were collected and are reported, including a list of screening barriers and adaptations, a list of developed staff training, a clinician stakeholder survey and focus group, and a patient stakeholder survey.
Results:
Clinicians reported being satisfied with the protocol and indicated that screenings provided new clinical information, changed their clinical care and helped to inform the medical needs of patients. Barriers included inadequate time to complete screenings and over-screening for prevalent stressors in the community.
Conclusions:
Implementation science provides a reliable framework for the implementation of a comprehensive ACE screening process by identifying the necessary conditions for high-quality implementation. With the appropriate resources in place, screenings are possible and enhance patient care. More attention is needed to identify primary care interventions for ACEs.
Implications for Impact Statement
Implementation science provides models for implementation that can improve the uptake of ACE screenings in Pediatric Primary Care settings. Integrated Care presents a comprehensive interdisciplinary approach that aids in providing appropriate responses to positive screenings.
Adverse childhood experiences (ACEs) are an important public health issue. ACEs are potentially traumatic events occurring between 0 and 17 years of age and include experiences like abuse, neglect, and household dysfunction. The seminal ACE study found a correlation between 10 specific childhood experiences and physical health outcomes related to high morbidity and mortality in adulthood (Felitti et al., 1998). Subsequent studies have expanded research to consider other adverse experiences like bullying, community violence, neighborhood safety, and racism (Cronholm et al., 2015). Adults who have experienced one or more ACEs are more likely to engage in behaviors such as smoking, substance use, physical inactivity, and suicide attempts and have a higher likelihood of being diagnosed with chronic diseases (Felitti et al., 1998; Hughes et al., 2017). These diseases include cancer, obesity, chronic bronchitis, liver, and cardiovascular diseases (Felitti et al., 1998; Hughes et al., 2017). Adults with ACE exposure are also at risk for depression, anxiety, and intimate partner violence (Hughes et al., 2017).
ACEs and Childhood Development
Adult health problems associated with ACEs are tied to disruptions in child development. Persistent adversity can consistently activate the stress response system and increase cortisol levels during childhood (Miller et al., 2011). This chronic activation affects future health through pathways of disrupted neurodevelopment leading to social and cognitive impairment and the adoption of health risk behaviors (US Centers for Disease Control and Prevention, 2021). Several studies have demonstrated that specific types of ACEs have distinctive impact on neurodevelopment. For instance, parental verbal abuse seems to significantly impact the arcuate fasciculus, a region of the brain that interconnects Broca and Wernicke's area and is involved in producing and understanding language (Choi et al., 2009). Another study highlighted that maltreatment at 10–11 years of age was associated with sensitivity in the right amygdala, a part of the brain that has a strong link with negative emotions such as fear and sadness (Pechtel et al., 2014).
Screening for ACEs
While the impact of high ACEs on child development and later adult health is well documented, ACE screenings have not been widely incorporated into routine Pediatric Primary Care (Rariden et al., 2021). Barriers to screening implementation initially centered around concerns of patient discomfort; however, research has mainly shown that families are receptive to screenings (Rariden et al., 2021). A greater concern has been the feasibility of incorporating ACE screenings in health care settings. Pediatricians often express concerns about the amount of time it would take to complete and respond to screenings, discomfort around how to discuss ACEs with families and overall low levels of confidence on the topic (Gillespie & Folger, 2017). Health care settings may be unprepared to screen particularly if they lack access to resources like multidisciplinary behavioral health support to help respond to positive screening reports (Flanagan et al., 2018; Rariden et al., 2021). There are several approaches that may help advance the identification of ACEs in Pediatric Primary Care settings. The first is utilizing an Integrated Care model where a practice team of primary care and mental health clinicians work together with patients and families to address mental health, health behaviors (and their contribution to chronic illness), and life stressors (Peek, 2013). Integrated health care teams include a myriad of interprofessional health care professionals including but not limited to social workers, mental health consultants, care managers, nurses, primary care physicians (PCPs), psychiatric mental health nurse practitioners, psychologists, and psychiatrists (Brown et al., 2021). Such a multidisciplinary team could help the concern about managing positive ACE reports. A second approach that may help advance the identification of ACEs is the utilization of implementation models in the development and application of screenings to ensure feasibility, acceptability, and sustainability (Silver et al., 2017). While there is a significant research base to addressing ACEs in Pediatric Primary Care, there is less empirical data about which strategies lead to successful implementation in this setting. Implementation of such efforts should not be spontaneous. Implementation science provides a reliable framework for integrating practices into routine care by identifying the necessary conditions for high-quality implementation (Silver et al., 2017). This is particularly important when developing processes with considerations for diverse populations. The current study describes the development and implementation of a comprehensive ACE screening protocol (ACEsPlus+) for children ages 6–16 in a rural Pediatric Primary Care setting. The specific aims of the study were to (a) utilize implementation science and the Exploration, Preparation, Implementation, Sustainment (EPIS) model (Moullin et al., 2019) as a guiding framework for high-quality implementation of a screening protocol, (b) to develop a screening process with adaptations to maximize the contextual fit within a Federally Qualified Health Center (FQHC) setting serving Latino families from an agricultural community, and (c) to use the Standards for Quality Improvement Reporting Excellence guidelines (SQUIRE 2.0; Ogrinc et al., 2016) to report findings from the implementation process.
Method
Implementation Strategy
The implementation strategy was to initiate the development and adoption of a comprehensive ACE screening protocol, ACEsPlus+, in a Pediatric Primary Care setting with Integrated Behavioral Health. The implementation process was informed by the EPIS framework, a framework commonly used in health service systems to guide implementation practices for evidence-based programs (Moullin et al., 2019). The methods for each of the EPIS phases are described below and outcomes for each of the phases will be reported in the Results section.
Exploration Phase
The primary goal of this initial phase was for stakeholders to consider the prevalence of ACEs in the patient population to later identify the best measures and methods for screening. There were three core activities that took place during this phase. First, an Implementation Resource Team (IRT; Moullin et al., 2019) was formed to guide the implementation, the result of a public–academic collaborative partnership between a FQHC and a public medical school. Members included administrators and physicians from the health center and clinical psychology faculty from the medical school who met regularly to guide the implementation efforts throughout each of the EPIS phases.
Next, a needs assessment was completed which focused on the prevalence of ACEs in the target population (Rosado et al., 2021). Finally, the IRT held meetings with clinical staff from the health center's Pediatrics department to introduce the concept of comprehensive ACE screening and to elicit their receptiveness as well as any foreseeable barriers. This included introductory meetings with all levels of staff to ensure that the unique perspectives of each position within the pediatric department were given consideration. Both nonclinical (operations director, office manager, receptionists, schedulers, billing staff) and clinical staff (nurses, medical providers, behavioral health providers) participated. Important components of this step were to (a) give staff a voice in the implementation process and (b) consider nonclinical factors that could influence the screening process (i.e., staff buy-in to follow through with implementation, scheduling, and operations factors).
Preparation Phase
The primary objective of this phase was to identify potential barriers to implementing screenings and corresponding needed adaptations, or innovation factors, that would maximize the contextual fit of the screening measures and methods to be implemented, including their fit within the service setting and patient characteristics (Moullin et al., 2019). The IRT utilized information gathered during the Exploration phase to generate a list of potential barriers and recommended adaptations to improve uptake of the screenings. Additionally, there were two key innovations completed during this phase. The first was to adapt the original ACE Questionnaire used in the CDC-Kaiser ACE Study (Felitti et al., 1998) to meet the literacy needs of the target patient population. The questionnaire is designed to screen for 10 ACEs, including physical, emotional, and sexual abuse, physical and emotional neglect, mental illness in the household, witnessing intimate partner violence, separation from parents, having an incarcerated relative and substance abuse in the household. The original questionnaire, which was designed for an adult to self-report childhood ACEs, was adapted to include a parent version used by caregivers to endorse any ACEs experienced by their child, and a youth self-report version used by youth ages ≥12. Additionally, adaptations included changes to simplify the text, such as substituting complex words (e.g., replacing “A parent often or very often humiliates me” with “…makes me feel very badly about myself”). Items were also broken down for clarity by asking about one adversity at a time. For example, separating multiple items like “Does a parent often or very often swear at you, insult you, put you down, or humiliate you?” into several sub-questions asking about each behavior individually (i.e., “Does a parent … swear at you?” Does a parent … insult you?” “Does a parent … put you down?” etc.).
The second innovation completed during the Preparation Phase was the development of an electronic tool, the Multilingual Automated Screening System (MASS; Rosado et al., 2018). MASS utilizes an electronic platform to administer the ACE questionnaire and other measures included in the screening protocol. MASS runs on touchscreen devices and is programmed to administer screening questions in a choice of languages (English, Spanish, and Creole). The software utilizes a graphical user interface that allows users to independently interact with the touchscreen device (without staff assistance) through graphical icons and audio indicators. This interface was designed to address screening barriers associated with the linguistic needs and reading/literacy levels of the patient population. MASS provides automated scoring of responses to screening items and generates a report that can be imported into an electronic medical record (EMR). This feature was designed to address implementation barriers associated with workflow limitations including challenges in scoring screening results during an office visit.
Additional measures were included given guidelines emphasizing the need for comprehensive ACE screenings that not only assess for experiences of adversity but also behaviors and associated symptoms (NCTSN, 2021). The Pediatric Symptom Checklist (PSC; Jellinek et al., 1988) was used as a measure of child psychosocial functioning. Two versions of the PSC were included in the screening protocol: the original parent-completed version and the Youth Self-Report (Y-PSC) completed by adolescents (ages >12). Additionally, the Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002) was completed by children ages 12 and older as a measure of adolescent depressive symptoms and by parents of younger children (ages 6–11) to screen for parental depression. The final step of the Preparation Phase was to develop staff training and formulate an implementation plan.
Implementation Phase
There were three notable components of the implementation plan. First, a caseworker position was added to the Primary Care team to help respond to positive screenings. If ACE screenings resulted in the identification of social service needs (i.e., food, housing, financial assistance, etc.) or patient navigation needs (i.e., access to specialty mental health services) the caseworker was available to work directly with families. The second component of the implementation plan was the development of a comprehensive protocol (ACEsPlus+) so that a team of providers could share the responsibility of responding to positive screenings according to the risk level identified. Third, training was provided to staff (including nurses, receptionists, etc.) on how to include the ACEsPlus+ screening into the regular workflow. Patient stakeholder surveys and a clinician survey were also administered with the goal of assessing experience with the protocol. Additionally, a focus group with pediatricians was conducted to measure their experience with the screening process.
Sustainment Phase
The sustainment phase had three main components with the goal to ensure the screening process became routine care and sustainable. First, leadership at the clinic adopted the established workflow into the operating procedures. Second, an effort was made to bill for services provided as a result of the positive screenings. Finally, the collaboration between the FQHC and the academic clinicians was ongoing and facilitated continuous data collection and analysis providing opportunities for updates and dissemination.
Data Collection
This study was approved by the Florida State University Institutional Review Board. Researchers approached pediatricians and invited them to participate in the study (i.e., clinician stakeholder survey and focus group). Written informed consent was obtained. A subset of patients was invited to complete a patient stakeholder survey by a bilingual research assistant following the Well-Child visit. Those who agreed completed a written informed consent form. There were six pediatricians (four female, two male) and three psychologists at the FQHC who participated in the implementation. There were a total of 2,347 children who were screened during the implementation process. Approximately 51% of the children were male with a mean age of 11 years old (SD = 3.1). Most children were Hispanic/Latino (87%) from Spanish-speaking households (63%). Approximately 88% of participants were covered by Medicaid.
Measures
Implementation Measures
Clinician Stakeholder Survey
Items from a screening feasibility survey were modified to measure pediatricians' experience with the ACEsPlus+ protocol (Glowa et al., 2016). The survey included 12 items on a 4-point Likert-type scale across two domains which assessed the clinician's attitudes and satisfaction with the protocol and evaluated the clinician's perception of the added value of screening for ACEs.
Clinician Focus Group
A 90-min focus group was facilitated with the six pediatricians participating in the implementation practice. An independent evaluator facilitated the group using an open-ended interview protocol. Interview questions were developed by the IRT and covered two general domains related to the ACE screening implementation. First, clinicians were asked to recall their practice pre-implementation and reflect on how/if they obtained information related to a child's history of adversity during a clinical encounter. They were asked to compare that practice to information obtained from the newly implemented screening practice. Second, clinicians were asked to discuss any added value they saw in incorporating screenings into Well-Child visits. Finally, they were questioned about any implementation barriers and concerns. Audio recordings from the focus groups were transcribed and then analyzed using a multistep, successive approximation coding process (Neuman, 2013).
Patient Stakeholder Survey
This survey included 13 questions adapted from a Parent Exit Survey (Fothergill et al., 2013) designed to measure patient comfort with screening questions included in the protocol. Parents and adolescents (ages >12) were randomly selected and asked to complete the survey at the end of an office visit.
Results
Implementation Outcomes (by EPIS Phase)
Preparation Phase Outcomes
Barriers and Solutions
Screening Implementation Barriers and Solutions
Staff Training
Staff Training by EPIS Phase
Implementation Phase Outcomes
Screening Protocol
A primary outcome of the Implementation Phase was the development of a comprehensive ACE screening protocol, ACEsPlus+ (Figure 1). The protocol included a team of Primary Care Providers (pediatricians), Primary Care Behavioral Health Providers (psychologists), and the caseworker that shared the responsibility of responding to positive screenings. Reception staff asked families to use the MASS software to complete the screening at check-in. An automated electronic report with results was imported into the EMR for review at intake/vitals by a nurse. The nurse reviewed the results to determine the level of risk as indicated by the screening protocol (Figure 1). Levels of risk were defined by the IRT during the Implementation Phase and were informed in part by recommended cutoff scores from developers of the PHQ-9 (Kroenke & Spitzer, 2002) and the PSC (Jellinek et al., 1988), clinical guidance around assessing adolescent suicide risk (Substance Abuse and Mental Health Services Administration, 2020) and child abuse and neglect (Flaherty et al., 2019) and recommendations for the interpretation of ACE screening data (NCTSN, 2021). Low Risk (Level 1) screenings were those with ACE scores of zero, depression PHQ-9 scores below the moderate range (≤9), and scores below the cutoff for psychosocial impairment on the PSC (<28) and Y-PSC (<30). Moderate to Significant Risk (Level 2) screenings were those with an ACE score >0, and/or depression PHQ-9 scores at or above the moderate range (≥10), and/or scores above the cutoff for psychosocial impairment on the PSC (≥28) or Y-PSC (≥30). Severe Risk (Level 3) screenings were those with ACE endorsement of abuse or neglect and/or domestic violence and/or substance abuse as well as any suicidal ideation reported on the PHQ-9. Note. See the online article for the color version of this figure.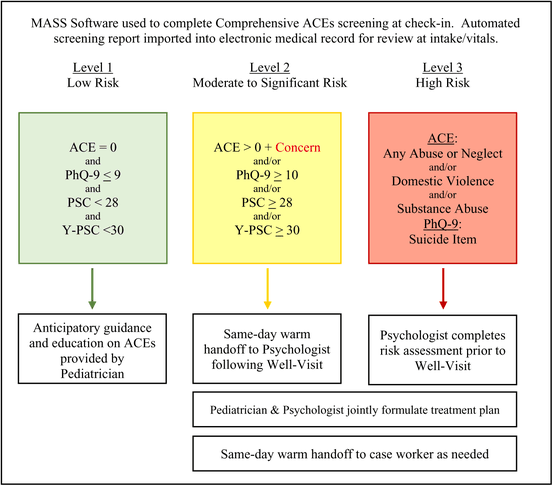
For Severe Risk screenings, the nurse alerted the psychologist who would begin an evaluation in the examination room prior to the pediatrician entering the visit. The psychologist's evaluation focused on a risk assessment to identify any imminent safety concerns. Initial findings were shared with the pediatrician prior to initiating the Well-Visit. Both providers worked together to formulate a treatment plan based on the family's needed level of care (i.e., Behavioral Health services in integrated Primary Care setting vs. referral to specialty mental health). Moderate to Significant Risk screenings were reviewed by the pediatrician during the Well-Visit. If a history of ACEs was endorsed but no psychosocial impairment or depression symptoms were identified, the pediatrician would review ACE responses with the family to determine if there were any concerns or unaddressed effects of the adversity. Families with ACE concerns and/or symptoms of depression and/or psychosocial impairment received a same-day warm hand off from the pediatrician to the psychologist following the Well-Visit. The psychologist initiated an evaluation, then shared preliminary findings with the pediatrician and both providers worked together to formulate a treatment plan based on the family's needed level of care. Low Risk screenings received anticipatory guidance and education on ACEs by the pediatrician. Anytime a social service need was identified based on positive screening results, families would receive a same-day warm hand off to the caseworker who would respond to identified needs. The caseworker would also help navigate patients referred for specialty mental health services. In their review of ACE reports, providers would discuss any discrepancies between parent-report of child ACEs and adolescent self-report. Providers would often follow up on any sensitive discrepancies (i.e., parental substance use, physical abuse, domestic violence, etc.) during portions of the office visit when they were alone with the adolescent.
Implementation Training
The Implementation Phase yielded additional training for staff (Table 2). This included technical training around the use of the MASS software and an implementation training module around the ACEsPlus+ protocol and workflow.
Clinician Stakeholder Survey
Clinician Stakeholder Survey Responses
Clinician Focus Group
Clinician Focus Group Domains and Themes
For Domain 2, pediatricians were asked to discuss any added value they found and implementation barriers and concerns. Table 4 describes three themes that emerged for “added value” and five themes for barriers and concerns. In general, the added value was to inform and support the medical needs of patients and increased team-based care. Pediatricians noted that screening results were an unexpected source of information for informing a patient's medical treatment and at times the screenings were a life-saving procedure for high-risk patients with chronic adversity and associated symptoms like suicidal ideation. Pediatricians' concerns included the length of the screening, amount of false-positive screening results, and how to best integrate the psychologist into the established workflow. The IRT utilized this information, along with Clinician Stakeholder Survey results, to work with the FQHC to modify provider schedules to address some of the challenges around integrating psychologists into the workflow. Psychologists' schedules were modified so that they had blocks of time without scheduled follow-up appointments so that they had more availability to collaborate with pediatricians.
Patient Stakeholder Survey
Over the first several months of the Implementation Phase, parents of screened patients were randomly selected and asked to complete the Patient Stakeholder Survey at the end of the office visit. Overall, parents reported feeling comfortable with questions across the different screening domains (see
Discussion
Summary
The current study used implementation science and the EPIS model to develop and implement a comprehensive ACE screening protocol in a rural Pediatric Primary Care (FQHC) clinic serving a predominantly Latino population. There are four key findings of the present research. First, implementation science and models like EPIS, offer useful strategies that can lead to the successful implementation of ACE screening efforts in Pediatric Primary Care settings. The implementation strategies applied in this study led to the successful screening of 2,347 children during the implementation process and to the adoption of the screening protocol into the operating procedures at the FQHC. Second, commonly cited ACE screening barriers, such as insufficient time to administer and score screening measures, can be addressed with electronic assessment tools like the MASS software utilized in this study. This type of technology automated screening and scoring and adjusted for literacy levels to maximize contextual fit. Third, staff training in the implementation setting promotes an implementation climate consistent with national recommendations. Fourth, Integrated Care teams can significantly facilitate the screening process and help ensure patient access to needed resources in response to positive screening results.
Interpretation
While there is a strong research base to addressing ACEs in Pediatric Primary Care there have been concerns about the feasibility of incorporating screenings to the extent that they have not been widely incorporated into routine care (Rariden et al., 2021). Bringing evidence to routine clinical care is often challenging and is a well-recognized gap across multiple key healthcare areas (Li et al., 2018). Results from this study support previous findings that have focused on implementation models as effective strategies to promote the successful uptake and sustainability of evidence-based practices (Tucker & Gallagher-Ford, 2019). The use of implementation models to bring evidence-based practices into community-based healthcare settings can have a significant positive impact on both the system and the people who are served. At a system level, the implementation in this study led to changes in workflow, introduced training to address workforce competencies, and changed service delivery through team-based care and billing. Pediatricians noted that screening results became a source of information for informing a patient's medical treatment (and not just their mental health treatment) and at times were a life-saving procedure for high-risk patients that presented with chronic adversity and associated symptoms.
The implementation phase in this study centered on the creation of a comprehensive ACE screening protocol that relied on an interprofessional team who responded to screening results. This team approach helped to address known implementation barriers related to providers feeling that they alone would not be able to manage screenings either due to lack of time, knowledge, or access to referral resources (Emerson, 2019). Integrating mental health professionals into the pediatric care team can help identify treatment needs, and create unified treatment plans (Hagan, 2017). Practice settings must be mindful that while Integrated Care teams can be very effective, it is important to establish procedures that facilitate their collaboration.
Limitations
A key component of this study in the early stages of implementation was the development of the IRT, which was the result of a partnership between the FQHC and a medical school. Without a similar partnership to bring together resources, it may be difficult to replicate the implementation process followed in this study. This could limit current inferences about feasibility within the Primary Care system. However, this underscores the need to develop sustainable community–academic partnerships has been cited as an essential factor for the successful implementation of interventions aimed at addressing important public health issues (Noel et al., 2019).
Conclusions
Clinician and patient stakeholder data from this study highlight the usefulness and value of implementation models when developing the practice of screening for ACEs. Clinicians found clinical utility in screening data to address ACEs. The model helped verify the feasibility of parents' using technology and recognizing its value. Data collected using this model contributed to sustainability as it informed FQHC stakeholders of the prevalence of the problem and highlighted the need for Integrated Care. Furthermore, it motivated FQHC stakeholders to work through identified barriers to ensure sustainability. Using the implementation model, staff connections with program developers (i.e., MASS software developers, medical school faculty) were formed. Staff were invested in the efforts that had gone into implementation and wanted to see those efforts continue long-term.
ACE screenings can be particularly useful given that they allow for rapid assessment of cumulative adversity (Bucci et al., 2016). However, ACE screenings need to be comprehensive and assess not just exposure to adversity but also associated symptoms and more importantly should result in linking children with needed interventions. Implementation research is a powerful tool to use for this end.