
Abstract
Objective:
Text messaging is a promising weight loss intervention modality for emerging adults who are overweight, but few studies exist to guide intervention development. Furthermore, sleep is emerging as a salient intervention target for weight management. This study examines feasibility and acceptability of two text messaging interventions for weight control in emerging adults, one of which includes sleep intervention content.
Methods:
Forty-three emerging adults who were overweight (BMI ≥ 25 < 30; ages 18–21) were randomized to receive either a text messaging intervention focused on diet and physical activity change, or a text messaging intervention designed to modify sleep behavior plus diet and physical activity. The interventions included motivational interviewing, education around health behaviors, physical activity, and dietary goal setting, as well as sleep goals for those in the sleep condition. All participants self-monitored diet, physical activity, and weight via text message for 3 months; those in the sleep intervention monitored nightly sleep duration.
Results:
Intervention acceptability and engagement were high for both conditions. In exploratory analyses, we observed that body mass index remained stable across assessments, regardless of condition. Participants in the sleep modification condition showed significantly greater sleep duration from pre- to post-intervention than those in the standard intervention.
Conclusions:
This study demonstrates that a weight loss intervention delivered by text messaging, including components designed to improve sleep, is acceptable and feasible for emerging adults who are overweight, and that extended sleep duration may be a benefit of the sleep modification intervention.
Implications for Impact Statement
This study provides support for the feasibility and acceptability of a text messaging intervention combining traditional behavioral weight loss strategies with sleep intervention in emerging adults. Results also suggest that a weight loss intervention targeting sleep improvements may increase sleep duration.
Emerging adulthood, a developmental window including individuals ages 18–25, represents a sensitive period for establishing life-long health behavior patterns which influence risk for weight gain and development of obesity (Barbour-Tuck et al., 2018). However, behavioral weight loss interventions for emerging adults have received limited research attention despite the fact that this period represents an optimal time for prevention and intervention given that emerging adults are developing weight-related habits that they generally maintain over the life course (Nelson et al., 2008). Preliminary studies suggest that weight management interventions delivered via text messaging are feasible and effective in reducing body mass index among emerging adults (Laska et al., 2009). Moreover, text messaging interventions utilizing automatically generated individualized feedback as a part of a weight management program enhance weight loss outcomes above and beyond standard of care interventions and waitlist control (Jensen et al., 2019; Napolitano et al., 2013), though this novel intervention approach is just beginning to be examined in emerging adults (Shoneye et al., 2019). College campuses are an ideal environment for providing health promotion interventions to this population given that nearly 40% of United States emerging adults are enrolled in post-secondary education (National Center for Educational Statistics, 2022) and risk for weight gain is elevated during college enrollment (Vadeboncoeur et al., 2015)
A separate literature highlights the association between sleep behaviors and weight outcomes. Specifically, poorer sleep has been consistently associated with obesity risk among adolescents and adults (Miller et al., 2018; Wu et al., 2014). Emerging adults who sleep less than 7 hr per night are at increased risk for obesity (Hart et al., 2013), while those who obtain adequate sleep are less likely to gain weight during the first-semester at a university (Ludy et al., 2018; Roane et al., 2015). This is salient, as up to 60% of college students report poor sleep quality (Lund et al., 2010), with two-thirds of the college population sleeping less than 8 hr per night (Whipps et al., 2018). No published studies have examined the efficacy of a mobile health sleep intervention for weight loss in an emerging adult population.
This present study is the first to evaluate two text-message weight loss interventions in emerging adults at high risk for development of obesity. Because the study was conceptualized as an obesity prevention feasibility/acceptability trial, we designed the interventions for emerging adults with overweight rather than for those with obesity. The two intervention conditions included (a) a standard weight loss text message intervention consisting of standard diet and physical activity behavior change components (STANDARD) and (b) a weight loss text message intervention addressing all content presented in the STANDARD intervention plus additional intervention addressing sleep behavior (SLEEP). The primary aim of the current study was to evaluate the feasibility and acceptability of each intervention modality using both quantitative measures and qualitative interviews. Based on findings from a similar text-message intervention study conducted with adolescents (Jensen et al., 2019), we hypothesized that emerging adults would find the text-messaging intervention feasible and highly acceptable. Additional exploratory analyses determined whether each intervention modality was associated with reductions in BMI and/or changes in objective and self-reported measures of sleep duration and quality.
Method
Participants
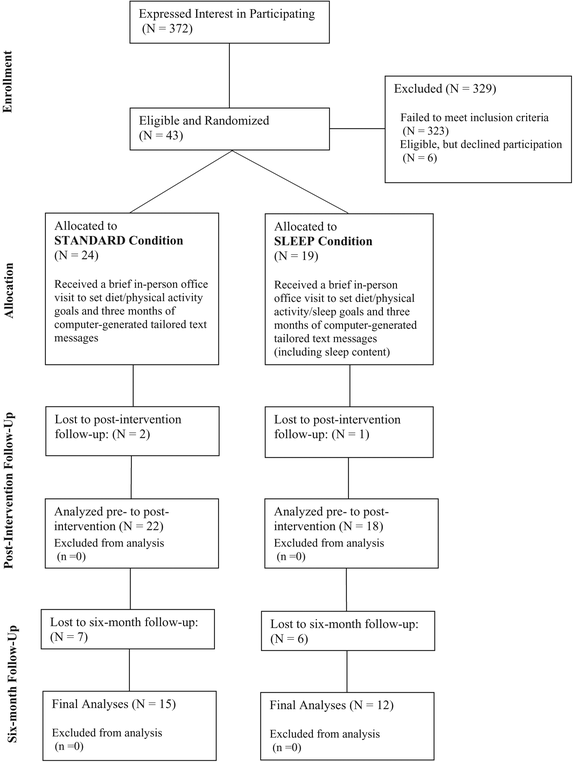
Consort Diagram
Sample Demographic and Anthropometric Characteristics (at Baseline)
Note. M = mean; SD = standard deviation; PSQI = Pittsburgh Sleep Quality Index.
aBetween group differences observed for BMI (p = .01).
Procedures
The institutional review board at the first author's institution approved all study procedures and participants provided informed consent (IRB#: X15030). Participants were randomly assigned to one of two treatment conditions using a simple randomization sequence generated by a researcher unaffiliated with the research. No blinding of treatment condition occurred for either interventionists or participants. All interventions were provided on a university campus in the Western United States across a 2-year period. All participants completed a pre-treatment assessment including completing all study questionnaires and measuring height and weight. Following this assessment, participants were fitted with an accelerometer (Actigraph GT3x+) and asked to wear the monitor on their non-dominant hip for 5 days, both day and night (only removing the device when swimming or bathing). Data gathered from accelerometers were used to assess baseline sleep parameters. All study procedures occurred during the academic year, not during summer months.
At the end of the 5-day baseline assessment period, participants attended a single in-person visit with a clinical psychology doctoral student lasting 50–70 min. The visit consisted of a brief motivational interview and a weight control behavior skills development intervention. The motivational interviewing techniques included in the intervention comprised eliciting client motivation for change, assessing potential barriers to behavior change, and amplifying ambivalence about behavior change. The skills building content for weight control behavior change included self-monitoring, stimulus control, reinforcement, and social support. Furthermore, participants received instruction regarding, and were asked to adhere to, Epstein's Stoplight Eating Plan (Epstein & Squires, 1988). Additionally, participants were instructed to increase their moderate physical activity to a minimum of 60 min per day. Participants monitored these behaviors via text messaging by reporting four key health behaviors daily: (a) number of servings of Red foods consumed, (b) number of servings of Green foods consumed, (c) minutes of physical activity engagement, and (d) current weight. Research assistants confirmed that the study participants had access to a scale. To provide an incentive to text daily, participants were reimbursed $1.00 for each nightly text they sent.
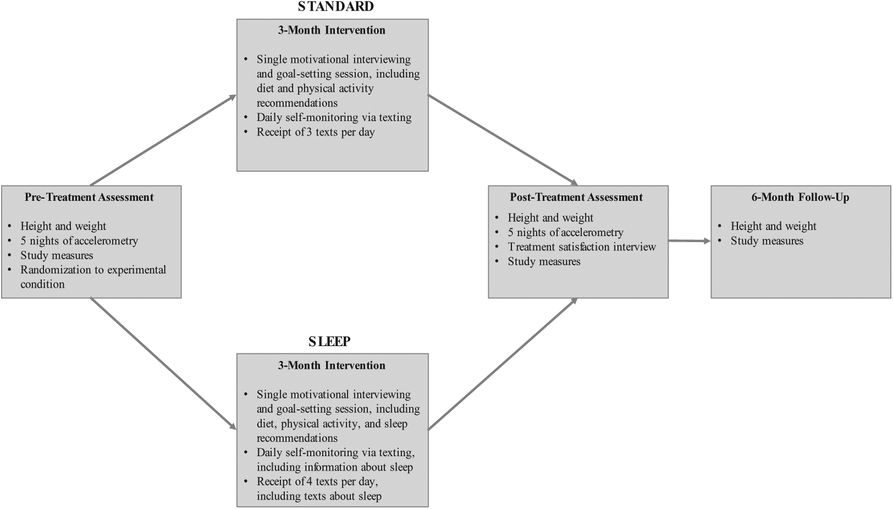
Standard Weight-Related Behavior Change Condition (STANDARD)
Participants randomly assigned to STANDARD intervention received the behavioral intervention outlined above, with the intervention lasting ∼50 min. Additionally, they received three automated text messages per day, corresponding to mealtimes (i.e., 8 a.m., 12 p.m., 5 p.m.), over the course of 3 months. Text messages addressed eating (e.g., “Eat your vegetables!” All parents say it. We hate when they’re right, but it's true. Fruits and vegetables help fight disease and help you lose weight) and physical activity (e.g., It's much easier to exercise when someone does it with you. Could you ask your mom to exercise with you a few days each week?) behaviors and were selected from a text message library developed by Woolford et al. (2010) containing 90 unique messages with evidence-based intervention content that utilize motivational interviewing principles. The automated computer text-messaging system, created by our research team to aggregate self-report data and deliver text messages to participants, used the information that participants texted to determine which of the 90 messages to send to the participant. Using a priori thresholding, we increased the ratio of messages targeting individually identified problem behaviors (e.g., participants who reported low green food consumption received more messages encouraging eating green foods). Text messages were spaced in such a way to avoid immediate repetition.
Standard Weight-Related Behavior Change Plus Sleep Behavior Modification Condition (SLEEP)
Participants randomly assigned to SLEEP condition received the same intervention as the STANDARD condition, plus an additional 20 min with the clinician to specifically target sleep behavior change. Specifically, this intervention addressed adhering to sleep hygiene behaviors, establishing consistent sleep and wake times, and creating healthy sleep associations. Participants in the SLEEP condition set the goal to obtain 8 hr of sleep per night. Participants were also instructed to include the number of hours of sleep they obtained the previous night in their daily text message (in addition to the four key health behaviors described above). In addition to the three automated text messages sent per day (corresponding with mealtimes), participants in the SLEEP condition also received one text message each evening including information relevant to sleep behavior change. These text messages were selected automatically from a library of 83 messages developed by study staff using evidence-based sleep improvement strategies but were not tailored based on participant sleep self-reports (see
Assessment Procedures
The pre- and post-treatment assessment included anthropometric measurements, questionnaire data, and actigraphy data. The post-treatment assessment also included a treatment satisfaction questionnaire and a qualitative interview about their experience with the intervention. During the 6-month follow-up visit, anthropometric measurements and questionnaire data were collected (see Figure 2 for study procedure overview).Randomized Pilot Trial Design
Measures
Body Mass Index
Participant weight and height were measured using a digital scale (Seca 869) and a portable stadiometer (Seca 217) with participants wearing light clothing and no shoes. BMI was calculated for each participant, using a standardized formula, BMI = weight (kg)/height (m2); Keys et al., 1972. BMI has been shown to reliably estimate body fat percentage (Mei et al., 2002).
Accelerometry
Data collected from Actigraph GT3X+ accelerometers were used as an objective measurement of sleep at the pre-intervention assessment and post-intervention assessment. Devices were worn for five consecutive nights, including three weekdays and two weekend nights. Waist-worn accelerometers (as compared to wrist-worn accelerometers) can approximate total sleep time but are less sensitive to sleep disturbances and have been shown to overestimate total sleep time (Hjorth et al., 2012; Slater et al., 2015; Takeshima et al., 2014). As such, we only analyzed total sleep duration from available accelerometry indices at the pre- and post-intervention.
Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) is a 19-item self-report questionnaire that assesses sleep quality. The PSQI demonstrates good evidence for its utility in research (89.6% sensitivity and 86.5% specificity) when distinguishing “good” versus “poor” sleepers (Buysse et al., 1989). The PSQI has good internal consistency across a variety of populations (α = .80; Buysse et al., 1989); within our sample, the PSQI showed adequate internal consistency (α = .74). We examined PSQI total score as a means for assessing sleep quality at all time points.
Client Satisfaction
Participants’ satisfaction with the intervention was measured at the post-intervention assessment using the eight-item Consumer Satisfaction Questionnaire (CSQ; Attkisson & Greenfield, 1999). This scale has satisfaction ratings that range from 0 to 32, and higher scores indicate greater satisfaction with the treatment. The CSQ has demonstrated adequate reliability (α = .83–.93) in previous studies (Attkisson & Greenfield, 2004) and excellent reliability in the current sample (α = .94).
Qualitative Treatment Satisfaction Interview
At the post-intervention assessment, all participants were invited to complete a semi-structured interview to provide feedback about their experience which asked several questions surrounding their overall impressions of the study, what aspects were most/least helpful, and thoughts surrounding the texts that they received. Consistent with the interview questions asked following an adolescent text-messaging weight control study conducted by our team (Jensen et al., 2019), the following questions were asked to all participants at the post-treatment assessment: (a) “What were your overall impressions of the weight control study?” (b) “What aspects of this program were helpful in managing your weight?” (c) “What could the study staff have done differently?” (d) “If you were to design a treatment program for managing weight, what else would you include?” (e) “How did you feel about receiving text messages from the researchers?” (f) “Is there anything you would have changed about the text messages if you were running the program?” and (g) “How could this intervention be changed to better serve college aged-young adults?” Participants in the SWBC + S condition were also asked, “Did you find the texts about sleep helpful?” Based on answers provided by participants, additional questions were asked to clarify responses or to better understand feedback.
Adherence/Engagement
We quantified adherence and participant engagement with the interventions by examining the number of text messages sent to the automated messaging system by participants. We calculated engagement with the text messaging intervention in three ways: (a) percentage of intervention days in which participants sent texts over the intervention period; (b) percentage of days during the first week in which participants sent text messages; and (c) percentage of days during the final week in which participants sent text messages.
Data Analytic Procedure
Sleep Accelerometry Cleaning and Scoring
Waist-worn actigraphy data was initialized and downloaded in 60-s epoch intervals within ActiLife5. Two research staff members coded bedtime as when physical activity demonstrated a downward decline in the evening and wake time as when the participant engaged in a noticeable amount of physical activity in the morning (Fekedulegn et al., 2020). Any discrepancies in coding that were greater than 60 min between coders were re-coded by a third coder and then averaged with the in-bed and out-of-bed times that were closest with the third coder. Discrepancies smaller than 60 min were resolved by averaging the in-bed and out-of-bed times between the two initial coders. Data were excluded if no movement was noted throughout the night. Using the Sadeh sleep algorithm, (Sadeh et al., 1994) we generated sleep duration estimates.
Data Analysis
Statistical analyses were conducted using SPSS Statistics 25 (IBM Corp). Although the intent of this pilot trial was to obtain estimates of feasibility and acceptability, an a priori power analysis conducted using G*Power 3.1.9.7 indicated that to have at least 80% power to detect a medium effect size (0.5) for a reduction of sleep problems (as indicated by PSQI total score), we would need 24 total participants (12 per group). Quantitative study outcomes were relatively normally distributed, and no significant outliers were noted. Missing data were handled with list-wise deletion. For the qualitative analyses, NVivo 12 (Melbourne, Australia) was used. Transcribed interviews were examined by two research assistants for similarities across response types using an open coding system; if several instances of similar response patterns were noted, the responses were then coded within a central theme. We used a grounded theory approach (Walker & Myrick, 20067) to allow for participant responses to guide the coding process, rather than use a predetermined coding system. Responses were allowed to be coded under multiple themes. Intercoder reliability was high (Cohen's κ = 0.96). When there were discrepancies between the two coders on a response, the two coders met together to discuss the discrepancy until a mutually agreed upon code was established. In instances where a mutual agreement could not be met, a third coder was used to resolve discrepancies.
Results
Demographics
Of the 43 participants randomized to a treatment condition, 40 completed the post-intervention follow-up. Of these 40 individuals, 27 completed the 6-month follow-up assessment questionnaires and 26 provided anthropometric measurements at the 6-month follow-up assessment. There were no significant differences noted in any key demographic variables or primary outcome variables by treatment condition at baseline assessment (p's > .05), except for baseline BMI (which showed a large difference between treatment conditions). Specifically, those in the STANDARD condition had significantly lower BMI (M = 26.84, SD = 1.43) than those in the SLEEP condition, M = 28.11, SD = 1.62; t(41) = −2.71, p = .01, 95% CI [−2.20, −0.32], d = 0.83. There were no reported instances of harm or unintended effects in either group.
Acceptability
Consumer Satisfaction
There were no differences in overall satisfaction with treatment across treatment conditions, t(39) = 0.55, p = .58, 95% CI [−2.29, 4.02], d = 0.17. Emerging adults in the STANDARD (M = 24.70, SD = 3.72) and the SLEEP condition (M = 23.83, SD = 6.20) rated the intervention favorably (maximum CSQ score = 32).
Qualitative Treatment Satisfaction
Themes Endorsed in Qualitative Interview with Sample Quotations
Seventeen participants (56.6%) found the text messages to be helpful and motivating, though half of the participants found the text messages to be repetitive in their content. Nine participants specifically stated that they would have preferred fewer texts. Nearly all participants (n = 27, 90%) had suggestions on how to improve the text messages, including: making the texts more personal (e.g., “Treat the texts as if you were texting a friend, using questions like, ‘Did you go running today?’”), getting texts about health facts, desires for recipes or exercise regimens, and having the daily texts address the content of texts the participants had sent in the night before. Eight participants in the SLEEP condition (61.5%) found the sleep texts to be helpful.
Four participants (13.3%) specifically mentioned liking the simplicity of the Stoplight Eating Plan, though three (10%) had difficulties with the Stoplight Eating Plan. Twelve participants (40%) stated that additional social support, whether through study staff or through interacting with other participants, would have strengthened the program. Eighteen participants (60%) requested access to additional exercise materials or dietary materials.
Feasibility
Adherence/Engagement
There were no significant differences in text messaging adherence by treatment condition across the entire 3-month intervention period, t(41) = −0.51, p = .61, Hedges’ g = −0.15, the first week of treatment t(41) = 0.17, p = .89, Hedges’ g = 0.05, or the final week of treatment t(41) = −0.32, p = .75, Hedges’ g = −0.10. Specifically, those in the SLEEP and STANDARD conditions sent messages on 68.33% (SD = 25.10) and 64.15% (SD = 28.58), respectively, of intervention days over the 3-month intervention period. During the first week of treatment, the mean adherence of those in the SLEEP and STANDARD conditions were 87.21% (SD = 17.10) and 86.31% (SD = 18.10), respectively. On the final week of active intervention (including text messages generated by the automated system), SLEEP and STANDARD condition adherence was 51.12% (SD = 36.36) and 54.75% (SD = 37.83), respectively.
Exploratory Analyses
Body Mass Index
Effect of Time, Condition, and Interaction of Time and Condition on Primary Outcomes
Note. PSQI = Pittsburgh Sleep Quality Index.
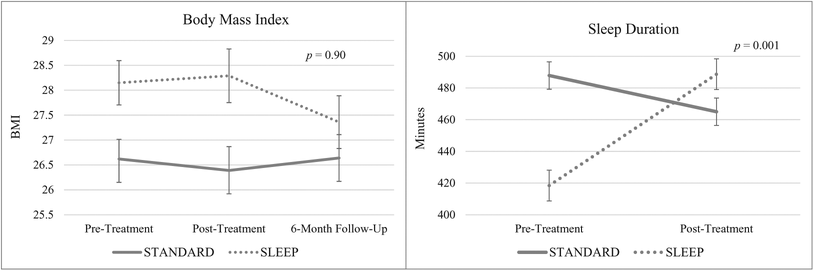
Interaction of Experimental Condition by Time on Body Mass Index and Sleep Duration
Objective Sleep Outcomes
There were no significant changes in sleep duration from pre- to post-intervention for the full sample (p = .06) nor were there significant differences in sleep duration at baseline by intervention condition (p = .55; see Table 3). However, we observed a large significant time-by-condition interaction for sleep duration (p < .001; ηp
2 = 0.31), with those in the SLEEP condition demonstrating greater increases in sleep duration from pre-intervention (M = 418.44, SD = 68.15) to post-intervention (M = 488.69, SD = 97.00) than those in the STANDARD condition from pre-intervention (M = 482.56, SD = 52.88) to post-intervention (M = 460.99, SD = 64.41; see Figure 3). In exploratory stratified analyses, we observed that those in the SLEEP condition demonstrated large and significant improvements in total sleep time (p = .001, d = 0.84) from pre-intervention to post-intervention, but not in the STANDARD condition (p = .21; see
Subjective Sleep Quality
There was no significant impact of time (p = .58), condition (p = .64), or interaction of time × condition (p = .23) on the PSQI total score (see Table 3). In exploratory stratified analyses, we observed that from pre- to post-intervention those in the SLEEP condition experienced a large and significant improvement in their PSQI total score (p = .03, d = 0.54), though no significant improvement was noted in PSQI total score from pre-intervention to the 6-month follow-up. For those in the STANDARD condition, there were no improvements in PSQI total score from pre- to post-intervention or from pre-intervention to the 6-month follow-up (p's > .54; see
Discussion
This pilot study tested the feasibility and acceptability of a text-messaging intervention for weight loss in emerging adults, including intervention for sleep behavior modification. In general, there were no differences in treatment satisfaction or engagement with text messaging across the two treatment conditions, with relatively high engagement with the text-messaging system occurring in both conditions. Engagement with the text-messaging system was significantly higher than that observed with adolescent populations (Jensen et al., 2019) and similar to or slightly higher than that observed in older adults (Napolitano et al., 2013; Shapiro et al., 2012). Furthermore, this text-messaging intervention appears feasible to administer to an emerging adult population for whom text messaging is a preferred form of communication (Napolitano et al., 2013).
Findings from the qualitative acceptability analyses suggest that emerging adults generally found the interventions and the daily text messages to be helpful. Some found that the interventions were too difficult or overwhelming, particularly while navigating the early years of college. We received consistent feedback that the participants desired fewer texts per day with more diverse content and greater personalization. In a similar pilot study in adolescents, similar reports were endorsed (Jensen et al., 2019). Consistent with Woolford and colleagues’ findings (2010), there was a strong desire across both conditions for greater information and resources about nutrition facts, exercise regimens, and meal plans. Almost half of our participants desired more involvement with study staff or other participants.
Given the results of our qualitative analyses, future interventions may benefit from more appointments with study staff throughout the intervention to increase accountability or using other means (e.g., social media) to foster additional accountability and comradery. Facebook groups in conjunction with text messaging and personalized feedback have been shown to be effective in enabling weight loss in college-aged students (Napolitano et al., 2013). Future work on improving the content of text messages is warranted, focusing on increasing personalization as well as providing resources to young adults through text messages.
Exploratory Outcomes
Exploratory analyses were undertaken to examine whether a future, fully powered trial is warranted. These analyses should be interpreted with caution given that this pilot trial is not well-equipped to provide a robust test of intervention efficacy. We did not observe significant reductions in BMI in either condition across time. However, it is notable that for both conditions, BMI remained stable across the 6-month assessment period. This finding is encouraging, particularly as we intervened in a population with high risk for weight gain. Overall, our findings suggest that a text messaging intervention may help stabilize weight during a period of high risk for weight gain, though we acknowledge that our study was not initially designed with a weight-gain prevention approach. Furthermore, the sleep modification did not appear to make a difference in weight loss compared to the group without the sleep modification. A study that was similar in size and purpose to our study, but that employed a 12-week educational program rather than a mobile health intervention, found that participants in the sleep modification group lost weight at a faster rate than the group without sleep modification (Logue et al., 2012). It is possible that a simple text-messaging intervention including sleep components might not significantly improve sleep to the level required to subsequently lower weight.
Interestingly, we found that sleep modification via a text-messaging intervention had a large effect on improving the sleep duration of emerging adults, with those in the SLEEP condition sleeping over 1 hr more following the intervention; those in the STANDARD condition had no significant change in their sleep. It is worth noting that those in the STANDARD condition did have greater sleep duration at baseline than those in the SLEEP condition (although this difference was not statistically significant), which may have resulted in a ceiling effect for sleep improvement. The improvement in sleep duration we observed in the SLEEP condition is comparable to the self-reported sleep improvement noted in a text-messaging intervention for improving sleep hygiene (Gipson et al., 2019) and to improvements in other health domains documented in the mobile health intervention literature (Murawski et al., 2020). Simple text-message interventions appear to serve as a feasible method for promoting sleep behavior modification for emerging adults.
This study possesses several notable strengths, including a mixed method design allowing for qualitative characterization of acceptability, a novel, ecologically valid approach to intervention delivery, and attention to a relatively understudied population in the obesity prevention/intervention literature. Conversely, several limitations should be considered when interpreting study findings. First, our sample size was small, which limited our power to detect differences between groups. Second, because feasibility/acceptability of the STANDARD intervention has been demonstrated with an adolescent population (Jensen et al., 2019) we did not include a no-treatment control group in the present study. Similarly, we did not employ a waitlist control group, so we are unable to determine if the changes that we observed are attributable to natural history effects. Third, characteristics of our sample limit generalizability of this study, including the relatively homogenous study sample (i.e., mostly white, female young adults, overweight). Studies that include individuals across a diversity of social identities including race/ethnicity, gender, sexual orientation, socioeconomic status, and intersections of these identities will be important to assess whether this intervention would be similarly feasible/acceptable for diverse clients. Fourth, the lack of blinding of the interventionists may have impacted treatment delivery. Fifth, while the interview questions were open ended, they were leading, which may have resulted in demand characteristics in the responses. Sixth, we did not assess objective sleep outcomes after the post-treatment assessment, limiting conclusions about maintenance of treatment benefit. Seventh, we used waist-worn accelerometers which can approximate total sleep time but may overestimate this variable and are inferior to wrist-worn devices and polysomnography for assessing sleep duration and quality (Takeshima et al., 2014); we also did not control for time of the academic year for sleep assessment, which may have impacted young adult sleeping patterns. Eighth, it is possible that expectancy effects contributed to the finding that participants in the SLEEP condition had increases in sleep duration following the intervention period, given that the treatment conditions were not blinded to participants. Ninth, paying participants to self-report via text message may have produced overestimates of feasibility relative to what would be observed absent financial incentives. Tenth, we did not assess for use of medications which may have influenced sleep behavior. Finally, we did not use sleep diaries to corroborate sleep and wake times, which may have influenced our objective sleep outcomes.
Study Implications
Both qualitative and quantitative satisfaction data suggest that emerging adults found the predominantly text message-delivered intervention to be acceptable and useful in their behavior change efforts. Given that emerging adults prefer communicating through text message over any other medium (Napolitano et al., 2013), this is an effective method for delivering intervention content. This intervention approach has the potential to increase the dissemination of the intervention because intervention intensity is low and intervention messaging is automated. Relatedly, the computerized delivery of text messages provides for customization of messages in response to behavior change (or lack thereof). Next, our findings suggest that including sleep modification content in our intervention improved sleep behavior. Our study results imply that fully powered studies of tailored text messaging interventions for emerging adults are warranted. Future research may also consider replicating this study for emerging adults who are at high risk for weight gain, but are still normal weight, to examine whether this low-intensity intervention would be effective in preventing weight gain (Vella-Zarb & Elgar, 2009).