
Abstract
Stress fractures in the distal phalanx of skeletally immature patients are rare and previously unreported clinical occurrences. We report on 2 adolescent sport climbers with such fractures of the dorsal metaphysis of the distal phalanx at the point where parts of the extensor tendon insert. A conservative treatment approach alone was sufficient in healing this fracture type in both patients after 12 wk. Clinicians should be informed of the existence of this rare clinical phenomenon and counsel patients that a conservative treatment approach may result in complete healing without the need for an invasive procedure.
Introduction
Distal phalanx fractures are the most common fractures of the hand in both adults and children. 1 Typical fracture patterns have been described for the adult as well as the growing phalanges.2,3 Even though stress fractures are the most common finger injuries among adolescent sport climbers, these lesions typically present as epiphyseal stress fractures at the base of the middle phalanges but have not previously been described in the distal phalanges. 4 -6
We report on 2 cases of chronic fractures in the distal phalanx presenting as stress fractures of the dorsal metaphysis. Further analysis of these specific cases allows for conclusions about the expansion of the insertion points in the extensor tendons of the growing hand.
Case Report
Case 1
A 13-y-old male rock climber presented to the Hand Clinic with a 3-mo history of progressive pain localized to the distal interphalangeal (DIP) joint of the right ring finger. Specifically, he noted that the pain was worst while using an “open grip position” during rock climbing. In this position, the DIP joint is flexed and the proximal interphalangeal (PIP) joint is almost entirely extended. The patient denied any acute trauma in the affected area. Upon clinical examination, the patient demonstrated a normal range of motion, but pain/tenderness was noted when the DIP joint was passively extended. Standard radiographs in the lateral view of the hand were diagnostic for a fracture of the dorsal metaphysis of the distal phalanx without articular involvement (Figure 1a and b). Furthermore, an ultrasound examination revealed that a small hyperechogenic fragment was visible without further displacement (Figure 1c).
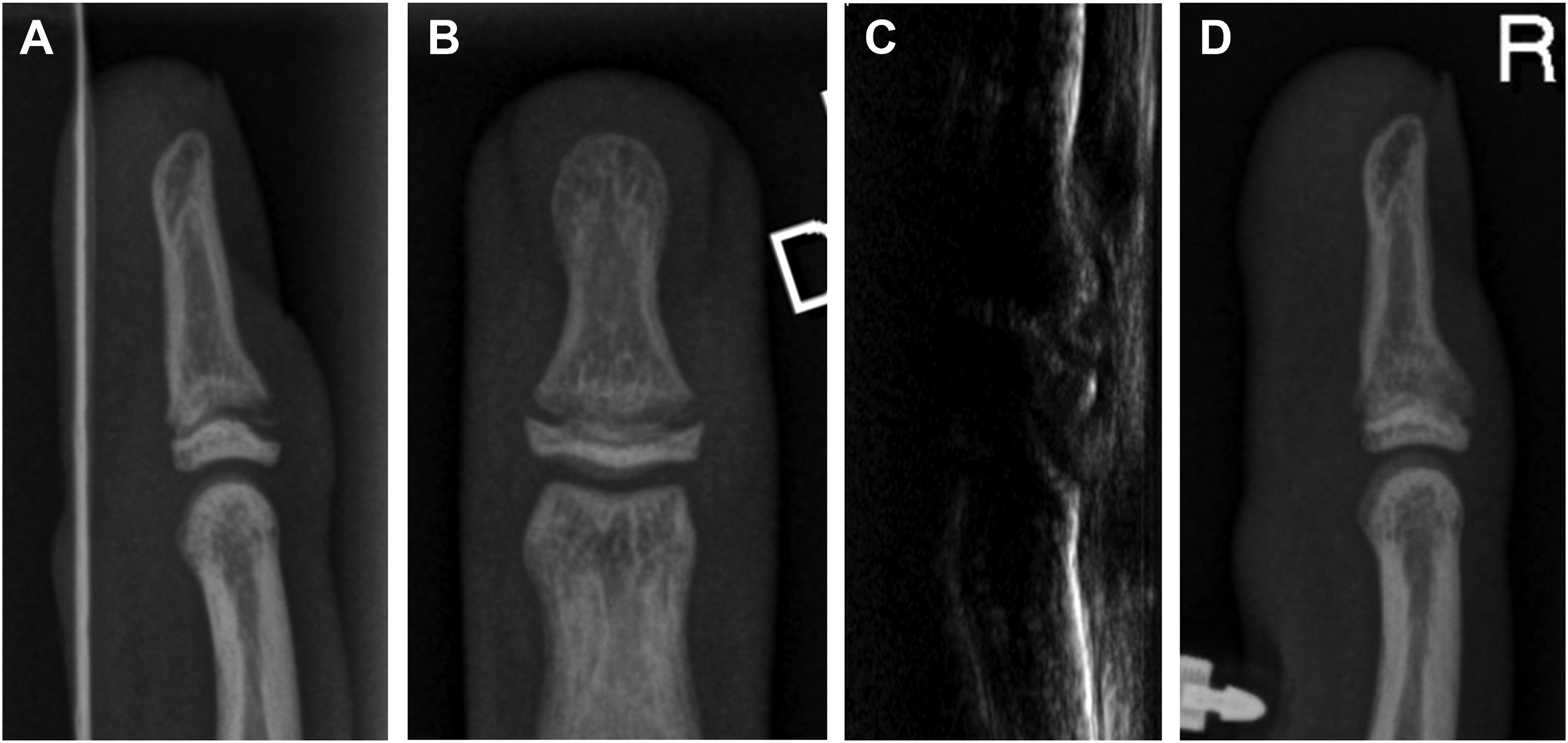
A and B, Radiographs of the distal phalanx of the right ring finger. C, Ultrasound image of the dorsal aspect of the right ring finger’s distal interphalangeal joint. D, Radiographic consolidation of the right ring finger after 3 mo.
Case 2
Our second patient, a male indoor sport climber, presented to the Hand Clinic at the age of 15 y after several weeks of progressive pain in the dorsal aspect of the distal phalanx of his right middle finger while actively flexing or passively extending the DIP joint. As with the previous patient, acute trauma was not reported, and the physical examination revealed a full range of motion with notable pain/tenderness over the dorsal aspect of the DIP joint. Similarly, radiographs in the lateral view demonstrated a fracture of the dorsal metaphysis without articular involvement (Figure 2).
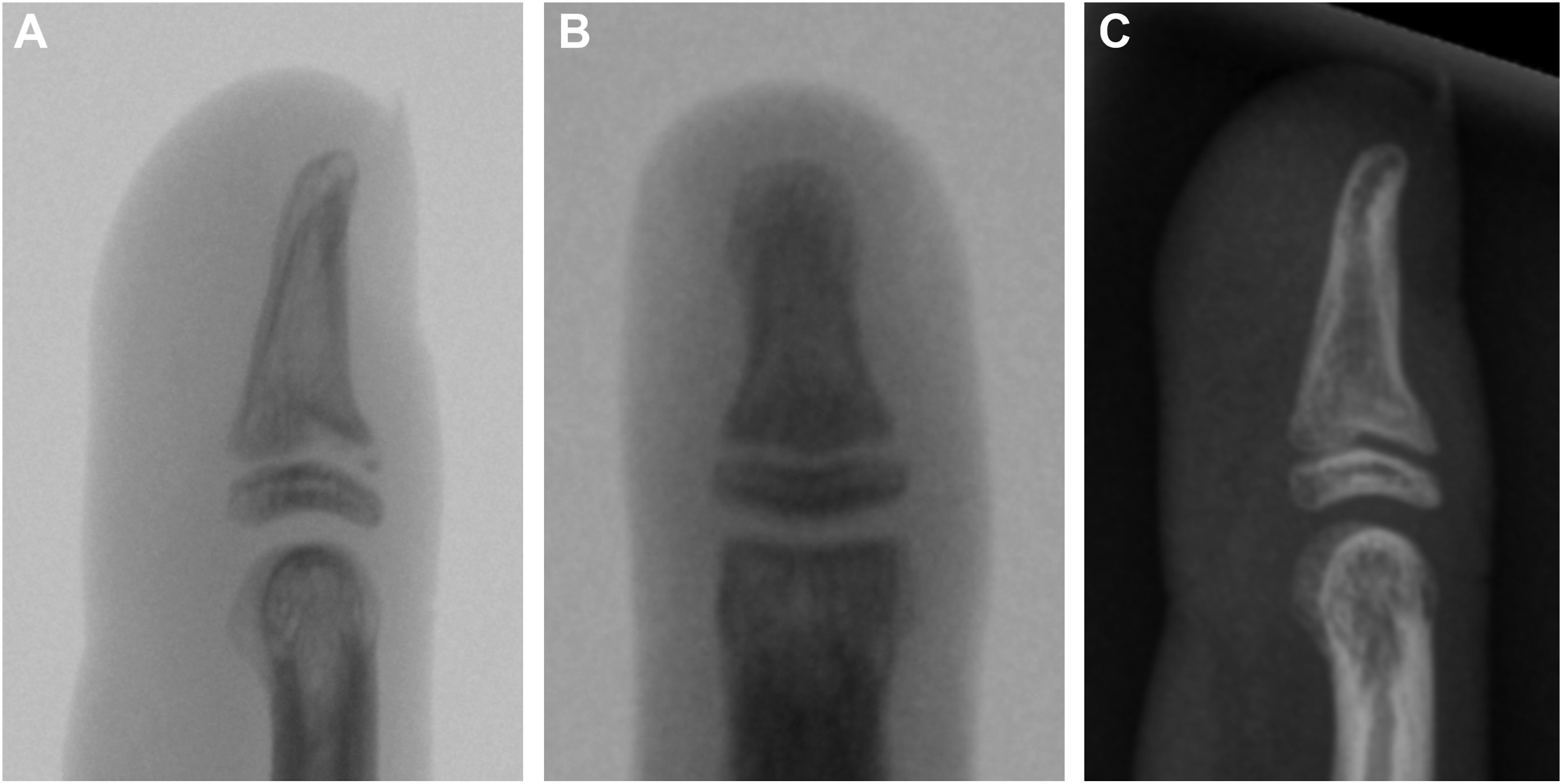
A and B, Radiographs of the distal phalanx of the right middle finger. C, Radiographic consolidation of the right middle finger after 3 mo.
Treatment
In both patients, a conservative treatment protocol was prescribed: a reduction in load-bearing activities of the finger and avoidance of terminal joint mobilization by taping of the DIP joint. A planned follow-up visit was scheduled for 12 wk after the initial consultation.
Outcome
Both patients complied with the treatment protocol as instructed, and neither required any interim consultations or interventions between the initial consultation and planned follow-up. At 12 wk, both patients reported resolution of their symptoms, and complete consolidation was noted on radiographs (Figures 1d and 2c).
Discussion
Stress fractures due to overuse in young athletes have been widely described in various sports. 7 Specifically, among skeletally immature climbers, the dorsal aspect of the middle phalanx base is prone to epiphyseal fractures (Salter-Harris type III fractures).8,9 These fractures are explained by an overuse of the “crimp grip position,” wherein the PIP joints are fully flexed and DIP joints are hyperextended. This results in high compressive forces on the dorsal aspect of the epiphysis and growth plate, which leads to the aforementioned fractures (Figure 3a). 10
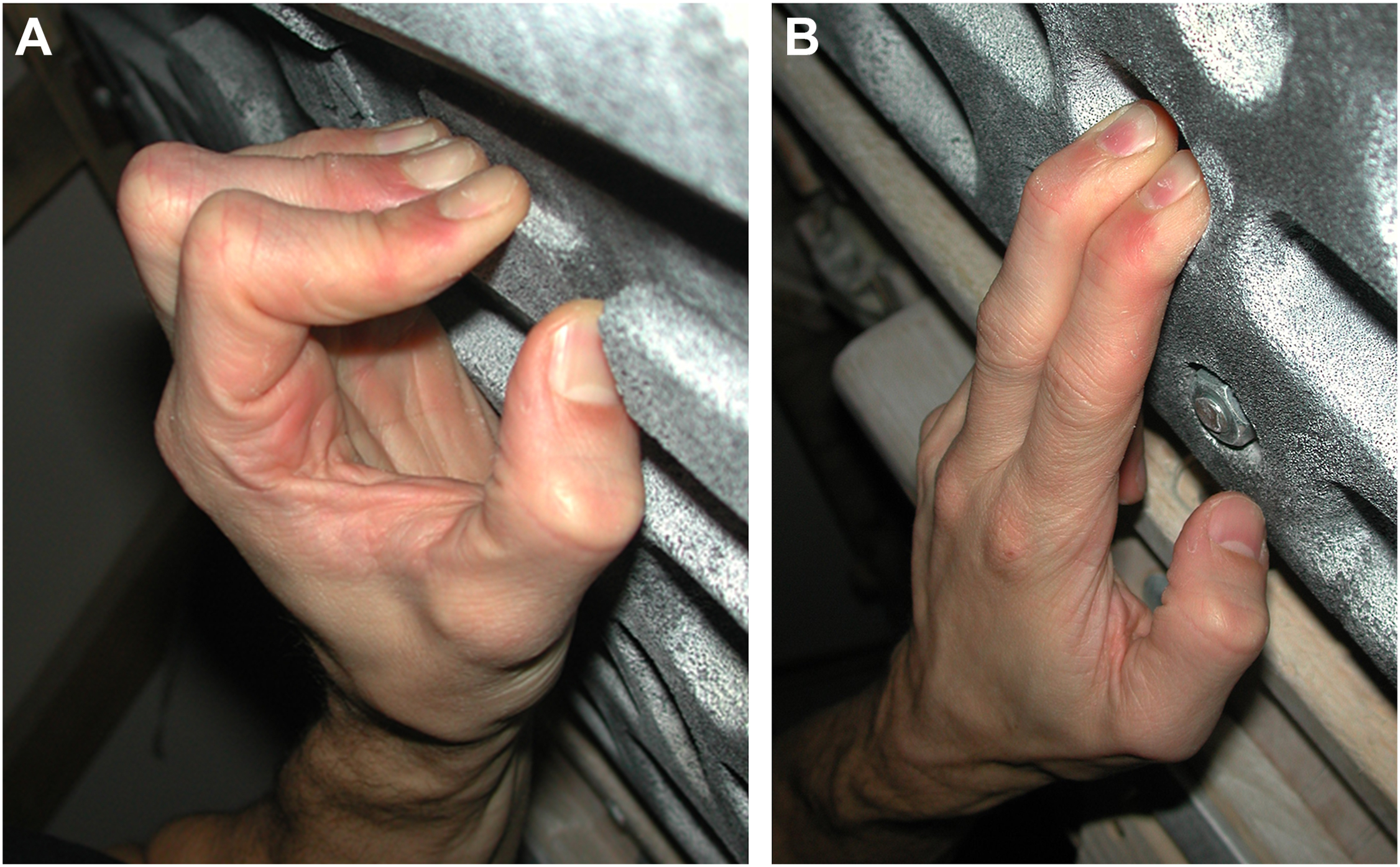
A, The “crimp grip” position with the proximal interphalangeal joints fully flexed and distal interphalangeal joints hyperextended. B, The “open grip” position is the most extreme grip position. In this arrangement, the distal interphalangeal joint is flexed and the proximal interphalangeal joint is almost completely extended. At times, a climber’s entire body weight will be supported with the fingers in this position.
In contrast, the “open grip position,” wherein the DIP joint is flexed and the PIP joint is (nearly) fully extended (Figure 3b), leads to a different force distribution in the fingers. In this state, major tension forces are applied to the distal phalanx. A stress fracture occurs when repetitive tension stress exceeds the strength of the phalanx, causing a small part of the bone attached to a tendon or ligament to tear away from the central part of the bone. 11 Hence, when examining the case examples described here, relative to the distal phalanx, it is reasonable to conclude that a portion of the distal extensor digitorum communis tendon must attach to the proximal rim of the metaphysis of the distal phalanx.
Although it has been previously described that the extensor digitorum communis tendons insert into the distal phalangeal epiphyses of their respective rays, our ultrasound examinations in children show an additional metaphyseal insertion of the extensor tendon (Figure 4). 12
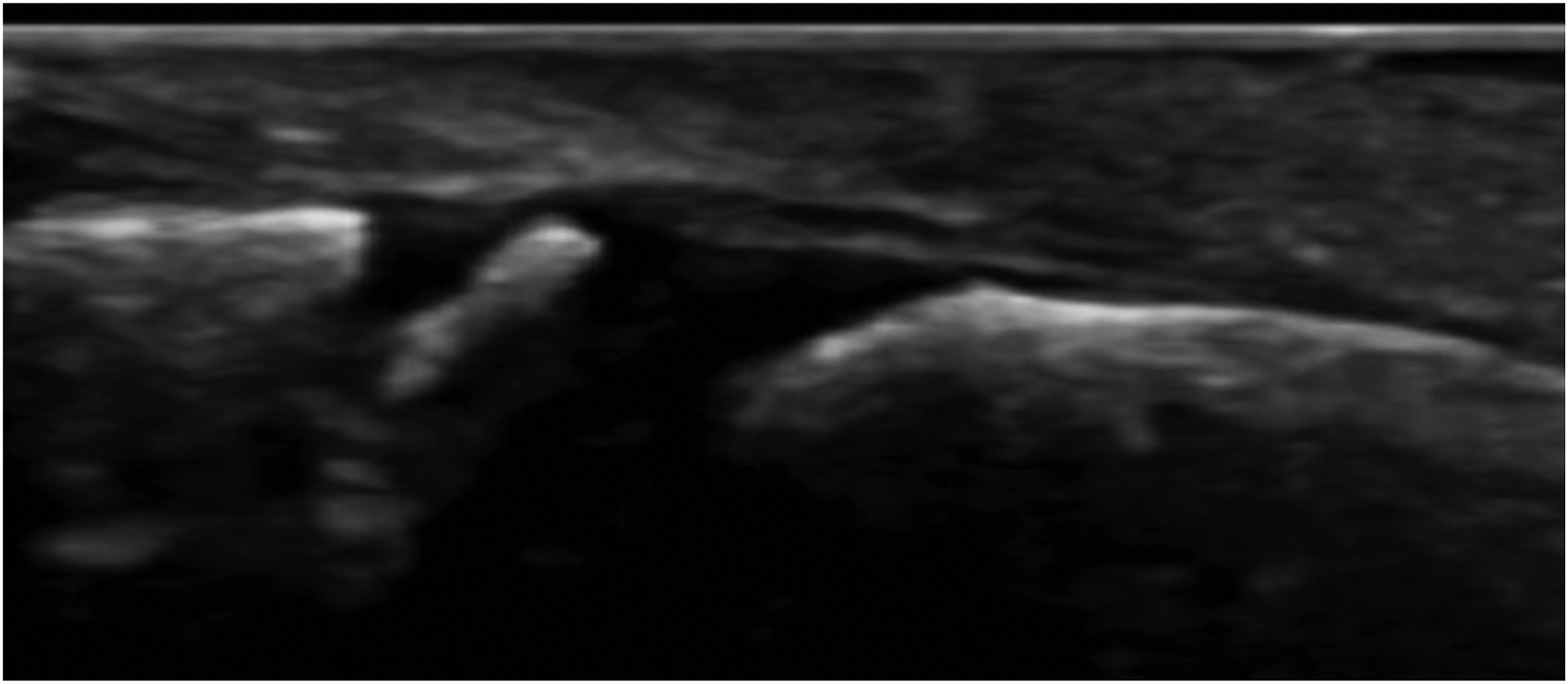
Ultrasound image of the dorsal aspect of the right middle finger’s distal interphalangeal joint in a healthy 8-y-old child.
This configuration also aligns with the findings of Hoch et al, 13 who demonstrated through plastination histologic cross-sections of the fingers that a part of the extensor tendon indeed inserts into the proximal part of the diaphysis (Figure 5). 14 We believe that this anatomic configuration resembles that which is found in the ulnar and radial collateral ligaments that extend beyond the edge of the physis to integrate the periosteum of the distal phalanx, as detailed by Bogumill 15 and verified via histologic sections.
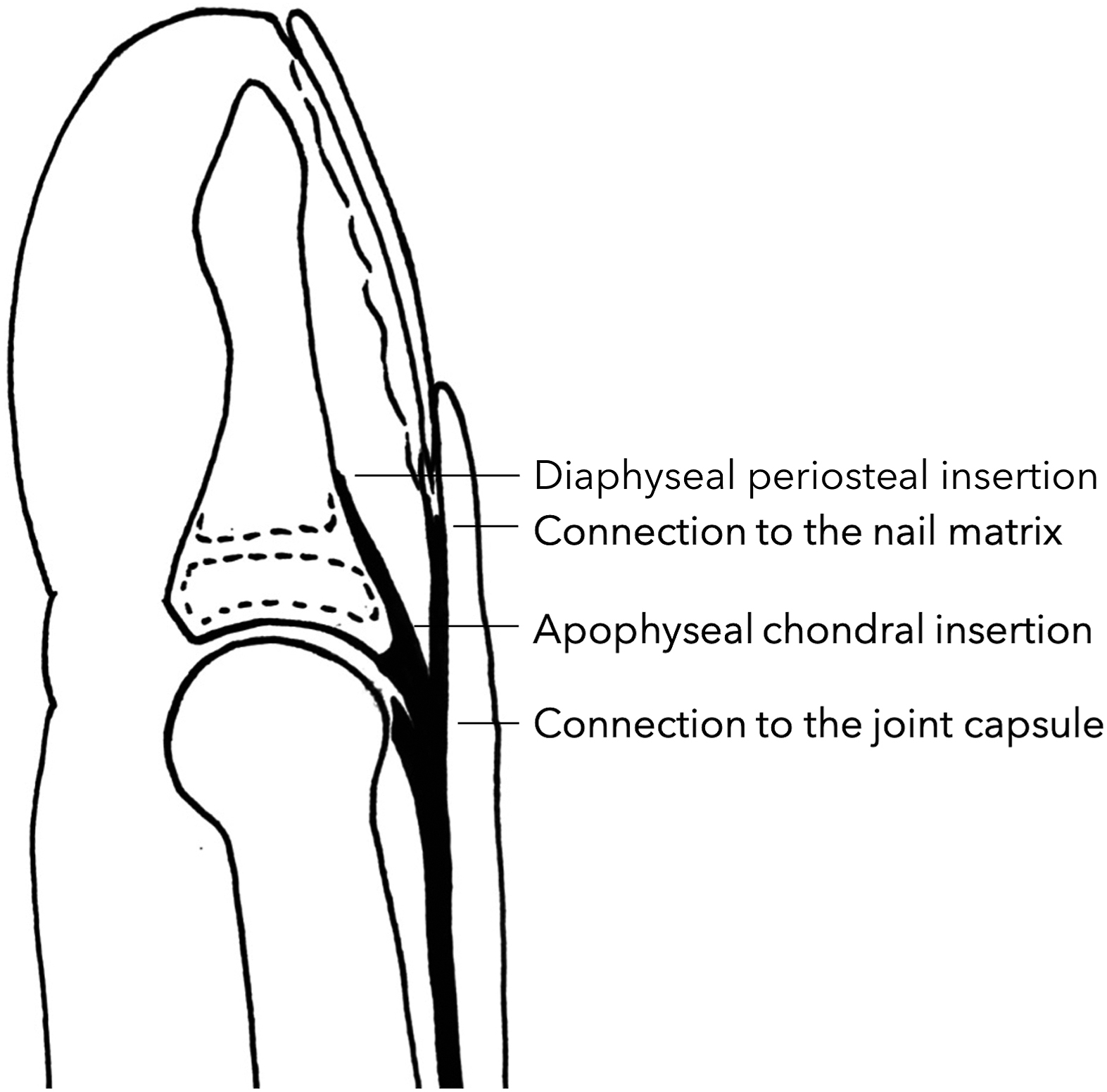
Graphic representation of the quadruple insertion of the pars terminalis of the dorsal aponeurosis (extensor tendon). After Frenz et al. 14
The constellation of presenting symptoms and objective findings in the cases discussed herein represent a distinct type of injury. First, this fracture type appears to result from a highly specific overuse, namely, the “open grip position” in sport climbing. Second, this fracture type is specific to skeletally immature patients. Fusion of the epiphysis in the distal phalanges of the hand typically begins at the age of 12 y in girls and occurs between the ages of 13 and 17 y in boys. 16 Consequently, in skeletally immature patients, the metaphyseal area is less stable and more susceptible to chronic stress and microfractures. The resulting metaphyseal fractures are analogous to Salter-Harris type II fractures. Third, this type of fracture pattern may be more likely to occur in males, like the cases presented herein, given the timing of physeal closure and the stability of the epiphysis, both of which are influenced by testosterone.4,6
As mentioned previously, the specific type of fracture described herein is not commonly encountered in clinical practice. This rarity may be attributable to the unique biomechanical stresses inherent to sport climbing. Furthermore, individual differences in age and physiological variability may contribute to the development of this specific fracture type. Moreover, unless x-rays are obtained in a strict lateral view, this fracture type can be easily overlooked.
In both patients, a conservative treatment approach consisting of reduction in load-bearing activities of the finger and avoidance of terminal joint mobilization was successful. Therapeutic finger taping around the DIP joint prevents terminal joint flexion, specifically during return of activity.
Given that the “open grip” position explains the pathomechanics of this fracture type, we recommend a balanced training regimen in skeletally immature climbers (specifically those aged ≤18 y). The training should focus on increased volume and diversity of climbing routes rather than increased climbing intensity to help minimize the likelihood of injury and preserve the individuals’ climbing capabilities over the long term.
Future investigations on this topic should explore whether there is an optimal amount and duration of activity restriction needed following stress fractures of the distal phalanx. Moreover, studies should seek to quantify whether (and to what degree) the resumption of normal activity prior to full bone consolidation increases the relative risk for secondary complications, long-term sequalae, or other unfavorable outcomes.
Given the rapid growth in the popularity of both professional and recreational sport climbers, recognition of this unique presentation and fracture pattern is clinically meaningful for healthcare providers who are engaged in the treatment of young patients who present with climbing injuries. In doing so, clinicians will be able to accurately diagnose and manage this rare but important fracture type.
Footnotes
Acknowledgements
Author Contributions: study concept and design (ADW, AS); data acquisition (AS, ADW, LR); drafting and critical revision of the manuscript (ADW); approval of final manuscript (ADW, LR, AS).
Financial/Material Support: None.
Disclosures: ADW reports support from Balgrist University Hospital for any publication or related fees associated with this study and a working contract or agreement with Balgrist University Hospital and University Children’s Hospital of Zurich.