Dr Lorenzo Albala: A 30-y-old helmeted man with a history of lumbar herniation status following microdiscectomy presented after a fall while mountain biking. The patient was riding in a New England trail system when the front wheel of the bike hit a root and he lost control. He flipped over the handlebar approximately 2 mi from the trailhead. The patient reported striking his head on the ground but had no loss of consciousness. During the fall, he also recalled the end of the handlebar striking his left lower abdomen and reported immediate severe pain.
The pain abated after a few minutes, and the patient attempted to ambulate down the trail, but within 10 to 15 steps he experienced a cramping sensation in his left lower extremity extending from his thigh to his calf. The discomfort improved with rest but recurred upon attempting to walk or ride his bicycle back to the trailhead, and he was forced to stop due to pain at increasingly frequent intervals. After 15 min, he noted that the sensation in his left foot was decreased, and he described it as if “walking on foam.”
Dr N. Stuart Harris: Although he struck his head, the likelihood of a significant head injury is minimal as he did not report headache or loss of consciousness. I am, however, concerned about the blunt trauma injury to the left lower quadrant. Did the patient exhibit other associated symptoms? Was the patient able to perform a physical exam at the trail side?
Dr Albala: The patient had no nausea or vomiting, and he did not report radiating pain into his flank or back. He did not note any tenderness or obvious outward signs of trauma to his head or cervical spine, and his helmet was intact. There was no external bleeding. Additionally, the patient stated that he urinated on the side of the trail and did not notice any blood.
Given the pain in his leg with ambulation, halfway to the trailhead he removed his shoes to inspect his feet. He did not appreciate any differences in perfusion. However, the ambient temperature was cool, and he had difficulty palpating his peripheral pulses.
Dr Luke Apisa: It is unlikely that the patient’s abdominal pain acted as a significant distracting injury from cervical spine trauma.1 Are abdominal injuries due to bicycle accidents common?
Dr Harris: Bicycle injuries are common in the United States and lead to approximately 500,000 emergency department (ED) visits annually. The majority of these visits are seen in the pediatric population.2 While head trauma is the most common injury associated with bicycle accidents, visceral abdominal injuries are not uncommon.3 A recent retrospective review in the pediatric population noted that 9% of all bicycle injuries were due to handlebar impact and contributed to almost 20% of all internal organ injuries.4 The handlebar end has a small surface area, and the force of the impact (mass × velocity2 / distance) can result in significant trauma to underlying structures. Handlebar injuries can include pancreatic injuries, traumatic abdominal wall hernias, duodenal hematoma, splenic and liver injuries, renal injuries, and rarely, vascular injuries.4-9 Handlebar injuries are less common in adults, presumably because of well-developed abdominal wall musculature as well as the reduced likelihood of riding recklessly, in comparison to children and adolescents.10 At this point, the patient requires evacuation and further evaluation.
Dr Apisa: The patient has injured himself about 2 mi from a trailhead. What are his options for evacuation?
Dr Albala: Land-based evacuation options are highly dependent on road proximity as well as access to communication networks. In this case, the patient was a few miles from a road but near an urban center. He was carrying his cell phone and had normal service and so could have activated emergency medical services via a 911 call at any time. However, his location in a park area would have limited traditional ambulance access to the fire road traversing the park. Local services, likely a combination of police, emergency medical technicians, and fire rescue, would have to interface with park services to plan an approach to the patient utilizing small off-road vehicles, on foot, or a combination of the two. If the patient was unable to self-evacuate at all, a litter carry for him would require at least 6 to 8 people.
On the other end of the spectrum, remote or backcountry areas with challenging terrain are infrequently serviced by roads. Mountainous and high-altitude environments and areas with thick vegetation may preclude a straightforward land-based approach and require higher level search and rescue capabilities. Helicopter or fixed-wing aircraft (including seaplane approach) and personnel with technical high-angle rescue or mountaineering skills are often required. Furthermore, the rescue personnel may need to provide a higher level of medical care as the time to reach and evacuate the patient is often prolonged.11
It is also likely that the aforementioned locations are beyond the reach of cellular communication. In these cases, the ideal tools involve satellite communication: personal locator beacons, satellite messengers, and satellite phones.12 Smartphone manufacturers are currently installing satellite-enabled microchips in premium cell phones to allow for emergency satellite messaging. Satellite capability may still be impaired by the surrounding environment and may require some movement to more favorable territory.13 Radio communications rely on line of sight; however, drone technology has been used to extend the communication reach of search and rescue teams.14 Additionally, wearable sensors (eg, Apple watch, glucose monitors, etc.) can provide remote patient monitoring.15
Dr William Binder: At present, we have a young man with what appears to be a lower abdominal injury. Do any commercial medical kits contain diagnostic technology? Would further diagnostics help in this location?
Dr Harris: Mountain biking medical kits can range from equipment designed to treat minor wounds and lacerations to kits devised to treat emergent life-threatening conditions. These types of kits can include a combat application tourniquet, an EpiPen, a 6.0 endotracheal tube, a scalpel, 14-gauge decompression needles, as well as wound treatment supplies and splints. These items are potentially lifesaving, provided a rider with medical training is on scene. However, they are less advantageous for a solo rider or if an injured rider is accompanied by someone without necessary medical training.
I am not aware of any commercial kit that includes a handheld ultrasound system. It is possible that use of a portable unit could lead to a field diagnosis, such as intra-abdominal bleeding through a positive focused assessment with sonography for trauma (FAST) exam or potentially even a vascular injury. However, this would not change management, aside from reinforcing the need for rapid evacuation.
Dr Albala: The patient managed, over 1 h, to get to the trailhead and to his car. He drove for about 30 min to a trauma center, bypassing a closer ED. Upon arrival to the trauma center, his clothing was removed, and the ED provider noted that his left foot was pale and cool (Figure 1). No dorsal pedis or posterior tibialis pulse was noted on palpation or on Doppler. The patient also reported left lower quadrant abdominal pain.
The patient’s left foot was pale and cool to touch.
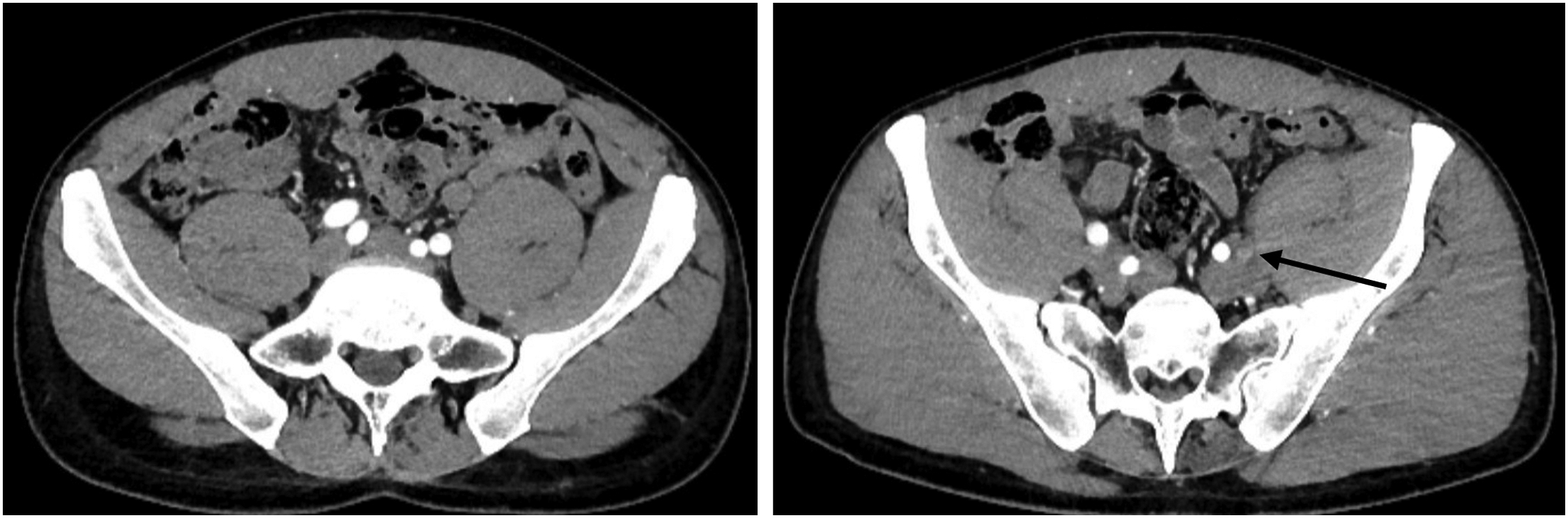
A CT angiogram of the abdominal aorta with lower extremity runoffs was performed (Figure 2) and revealed a complete occlusion of the left external iliac artery with distal recanalization. A posttraumatic dissection flap extended from the posterior femoral artery and superficial femoral artery bifurcation to the distal left femoral artery. There was no evidence of a flap more proximally in the aorta. The right-sided vascular tree was patent.
Occlusion of left external iliac artery with distal recanalization. Note that the left external iliac artery is not perfused at this level (right, arrow).
Dr Binder: How common are vascular injuries in biking? What are the injury patterns reported in mountain biking? I have not seen this previously.
Dr Stephanie Lareau: In the United States, there are more than 8 million mountain bikers, and there are more than 30 million worldwide. Injury rates are high. Some studies report up to 40 injuries per 1000 h of riding, although other reviews have noted a lower incidence.16,17 Limb or life-threatening injuries occur at a rate of 2.5 per 1000 h of riding.16 Numerous North American ski resorts offer lift-accessed terrain, and this has resulted in steeper, longer, and more technical rides, increasing the risk for serious injuries.18
As expected, abrasions and bruises are the most common injuries noted in mountain biking. Fractures are also common, with the clavicle followed by the distal radius and scaphoid being the most frequently fractured bones.17 Head and traumatic spinal injuries are also noted. The British Columbia Trauma Registry reported that of the 399 mountain bikers admitted to trauma centers, 12% had head injuries and 12% had spine fractures.19 Of the 5% of abdominal injuries reported by the British Columbia Trauma Registry, no vascular injuries were cited.19 While vascular injuries secondary to handlebar trauma have been reported in pediatric bicycle accidents, there is a paucity of literature on adult vascular handlebar injuries. One case report describes a celiac artery dissection after a mountain bike crash with a grade 3 of 4 splenic laceration with hemoperitoneum.20 Overall, vascular injuries appear to be rare within reported mountain biking injuries.17,21,22
Dr Apisa: What happened after the CT angiogram?
Dr Albala: The patient was started on a heparin infusion and taken to the operating room for vascular surgery. At approximately 7 h after initial injury, the patient underwent a thrombectomy and external iliac stent insertion.
Dr Sunita Srivastava: There were several factors that mandated an emergent approach. The first was that the patient was acutely symptomatic and, being young without pre-existing collaterals as we see in older patients with atherosclerotic disease, there were no collaterals to ameliorate the acute loss of flow from the injury. In addition, acute limb ischemia can only be tolerated for 6 to 8 h without impacting peripheral nerve and muscle function. The ischemia to both the peripheral nerves and muscles could have resulted in permanent impairment.
Anticoagulation alone would not have been sufficient to clear the thrombosis incited from the blunt injury, but rather, it prevented thrombus propagation until the vascular injury could be corrected. The patient required a femoral exploration due to the extension of the thrombus/dissection to the femoral bifurcation, and after this was addressed by cutdown and exploration with repair, the more proximal external iliac thrombosis was addressed with self-expanding stent placement. Additionally, the patient’s external oblique fascia was torn, indicating that the handlebar pushed into the retroperitoneal space, injuring the external iliac artery. Manual inspection of the defect led to the retroperitoneal space and vessel. The fascia was repaired after reestablishing inline flow to the limb. Fasciotomies were not performed because the calf was soft and not edematous upon inspection during the groin closure likely due to expeditious restoration of flow. Compartment syndrome requiring fasciotomies can occur after establishing perfusion following a prolonged period of ischemia. Fortunately, this did not occur.
Dr Lareau: What was the outcome?
Dr Albala: The heparin infusion was discontinued 5 h postoperatively. The patient was started on daily 81 mg aspirin and 75 mg clopidogrel. He was discharged on postoperative day 3. Lower extremity ankle-brachial index and stent Doppler ultrasonography were normal at 3 wk and 3 mo postoperatively. Clopidogrel was discontinued after 1 mo. At the 3-mo postoperative visit, he denied any claudication symptoms, pain, or paresthesias. The patient was counseled about continuing lifelong daily aspirin as well as prophylactic anticoagulation for long flights.
Conclusion
Mountain biking injuries are most commonly musculoskeletal. In blunt trauma to the abdomen, however, there is a risk of solid organ injury and vascular injury. There are minimal effective treatments for these conditions in the field, highlighting the importance of rapid evacuation to definitive medical care. Thorough physical exam and high suspicion of serious injury were important in this patient’s successful outcome.
Footnotes
Acknowledgements
Disclosures: William Binder is Editor-in-Chief of WEM and Stephanie A. Lareau is Education editor of WEM. Per WEM policy, they had no involvement in the editorial or peer review process for this manuscript.
References
1.
KhanA.D.LiebscherS.C.ReiserH.C.SchroeppelT.J.AnstadtM.J.BosargeP.L.et al.Clearing the cervical spine in patients with distracting injuries: an AAST multi-institutional trial. J Trauma Acute Care Surg2019; 86(1), 28–35.
2.
HussainB.SittoT.M.SethuramanU.Thrombosis of external iliac and common femoral arteries secondary to blunt trauma due to handlebar injury. Am J Emerg Med2021; 49, 291–293.
3.
VandewalleR.J.BarkerS.J.RaymondJ.L.BrownB.P.RouseT.M.Pediatric handlebar injuries: more than meets the abdomen. Pediatr Emerg Care2021; 37(9), e517–e523.
4.
CherniawskyH.BratuI.RankinT.SevcikW.B.Serious impact of handlebar injuries. Clin Pediatr2014; 53(7), 672–676.
KangabamB.Traumatic Spigelian hernia following blunt abdominal trauma. Cureus2023; 15(2)e35564.
7.
DhakreV.W.KadamS.B.GowdaA.IyerS.Handlebar sign: a bruise with underlying visceral injury. BMJ Case Rep2019; 12(11)e231835.
8.
HiroseT.OguraH.KiguchiT.MizushimaY.KimbaraF.ShimazakiJ.et al.The risk of pediatric bicycle handlebar injury compared with non-handlebar injury: a retrospective multicenter study in Osaka, Japan. Scand J Trauma Resusc Emerg Med2015; 23(1), 66.
9.
LuuA.M.MeurerK.HerzogT.UhlW.BraumannC.Diagnostic double strike in the emergency room - two cases of complete pancreatic ruptures due to bicycle handlebar injuries on two consecutive days. J Med Case Rep2018; 12(1), 85.
10.
BohmerJ.H.ProustA.F.Adult bicycle handlebar injury. Am J Emerg Med2006; 24(5), 624–625.
11.
TingL.WilkesM.Telemedicine for patient management on expeditions in remote and austere environments: a systematic review. Wilderness Environ Med2021; 32(1), 102–111.
12.
KeefeR.F.WempeA.M.BeckerR.M.ZimbelmanE.G.NaglerE.S.GilbertS.L.et al.Positioning methods and the use of location and activity data in forests. Forests2019; 10(5), 458.
13.
JonesB.TangA.NeustaedterC.Remote communication in wilderness search and rescue: implications for the design of emergency distributed-collaboration tools for network-sparse environments. Proc ACM Hum Comput Interact2020; 4(GROUP), 1–26.
14.
McRaeJ.N.NielsenB.M.GayC.J.HuntA.P.NighA.D.Utilizing drones to restore and maintain radio communication during search and rescue operations. Wilderness Environ Med2021; 32(1), 41–46.
15.
DavisC.B.LorentzenA.K.PatelH.CheungD.WrightA.LemeryJ.et al.The intersection of telemedicine and wilderness care: past, present, and future. Wilderness Environ Med2022; 33(2), 224–231.
16.
FioreD.C.FwllowsK.M.HennerT.A.Injuries in mountain biking and implications for care. Muscles Ligaments Tendons J2020; 10(2), 179–191.
17.
CarmontM.R.Mountain biking injuries: a review. Br Med Bull2008; 85, 101–112.
18.
KotlyarS.Cycling injuries in Southwest Colorado: a comparison of road vs trail riding injury patterns. Wilderness Environ Med2016; 27(2), 316–320.
19.
KimP.T.W.JangraD.RitchieA.H.LowerM.E.KasicS.BrownD.R.et al.Mountain biking injuries requiring trauma center admission: a 10-year regional trauma system experience. J Trauma2006; 60(2), 312–318.
20.
LiB.V.Damodaran PrabhaR.NarraM.NguyenH.Traumatic dissection of the coeliac artery and splenic injury following blunt trauma. BMJ Case Rep2019; 12(8)e229405.
21.
AnsariM.NourianR.KhodaeeM.Mountain biking injuries. Curr Sports Med Rep2017; 16(6), 404–412.
22.
WillickS.E.EhnM.TeramotoM.KlattJ.W.B.FinnoffJ.T.SaadK.et al.The National Interscholastic Cycling Association Mountain Biking Injury Surveillance System: 40,000 student-athlete-years of data. Curr Sports Med Rep2021; 20(6), 291–297.