
Abstract
Jellyfish stings are the most common cause of marine envenomation in humans. Various species of box jellyfish have been identified around Penang Island, Malaysia, and these include multitentacled and four-tentacled box jellyfish (class Cubozoa). The typical syndrome following envenomation from these jellyfish has been poorly documented, posing a greater challenge when managing an unidentified jellyfish sting from Penang Island. We report a case of a 32-y-old man from Penang Island who was stung by an unidentified jellyfish while walking into the sea. The patient reported that he felt an immediate and severe electric current‒like pain over both thighs, left flank, and left forearm, followed by chest discomfort and breathlessness. Vinegar was applied over the affected areas, and he was rushed to a hospital, where he was treated with analgesia, steroids, and antihistamine. He refused hospitalization and was discharged against medical advice. He then presented to a noncoastal hospital 377 km away in Kuala Lumpur on the following day with severe pain over the affected sites as well as chest discomfort, shortness of breath, and abdominal cramps. The electrocardiograph demonstrated features of Wolff-Parkinson-White. Serial blood test results showed elevated creatine kinase but normal troponin I levels. The patient was managed symptomatically over a period of 4 d and was discharged with cardiology follow-up. Appropriate health-seeking behavior needs to be emphasized. This case report provides an opportunity to document the signs and symptoms of envenomation from possibly an undescribed jellyfish species near the coastal waters of Penang Island.
Highlights
Jellyfish stings are the most common marine envenomation in Malaysia. Box jellyfish envenomation may manifest with a wide range of signs and symptoms of variable intensity, including potentially fatal cardiovascular manifestation. Close serial monitoring in a controlled environment is important and includes optimal pain control with opioids. Appropriate safety and health-seeking behavior need to be emphasized to minimize the risk of jellyfish stings.
Introduction
Jellyfish are the most common cause of marine stings; however, there is scarce documentation of harmful jellyfish species in Malaysia. 1 There are marked differences in the envenomation syndrome of the various groups of harmful jellyfish. Among the many harmful jellyfish species, those of the class Cubozoa (eg, box jellyfish) are the most harmful to humans, particularly children and the elderly. Chironex species, a large multitentacled box jellyfish, has the most toxic venom and may cause death within 70 min. Smaller-sized box jellyfish from the family Carukiidae are also known to have caused envenomation known as the Irukandji syndrome.2,3
A study by Low 4 described 9 scyphozoan jellyfish species found in Peninsular Malaysia: Chrysaora chinensis, Cyanea sp, Versuriga anadyomene, Rhopilema hispidum, Rhopilema esculentum, Phyllorhiza punctata, Acromitus flagellatus, Lobonemoides robustus, and Lychnorhiza malayensis. A preliminary survey report of jellyfish diversity and distribution along coastal waters of Peninsular Malaysia identified 8 different species of jellyfish inhabitants: Chironex sp, Chrysaora hysoscella, Chrysaora quinquecirrha, P punctata, Cyanea capillata, Cyenea lamarckii, Rhyzostoma pulmo, and Lobonema smithii. 5 A study of monthly abundance and distribution of jellyfish population in the coastal waters of Penang National Park identified P punctata, Chrysaora sp, Rhopilema sp, Chiropsoides buitendijki, and Carybdea morbakka. 6 In Sabah, 6 species belonging to 2 classes and 6 families have been reported: Chironex yamaguchii, Acromitus maculosus, Crambione mastigophora, Linuche aquila, Netrostoma sp, and P punctata. 7 The frequency and severity of jellyfish stings appear to be increasing in Southeast Asia; however, it may be significantly underestimated in Malaysia. 8 There have been reports of severe and fatal cases of chirodropid-type stings occurring in coastal waters of Langkawi and Sabah. 1 A 3-y study of jellyfish stings in Langkawi reported that a significant number of patients presented with mild Irukandji and Irukandji-like syndromes. 9 A recent study of 45 cases at the western coast of Peninsular Malaysia has also identified similar presentations. 10 However, the diagnosis of these cases was not verified. There could also be incidences of multitentacled box jellyfish stings that were mistakenly documented as Irukandji and Irukandji-like syndrome. Therefore, a careful documentation of all clinical presentations of jellyfish sting is important and needs verification. We present a case of an unidentified jellyfish sting presenting with mixed features of box jellyfish envenomation syndromes, which may suggest the possibility of a new type of multitentacled box jellyfish envenomation syndrome or possibly distinct from it as well.
Case Report
A 32-y-old West African man presented to the emergency department of a private hospital in Penang Island after he was stung by an unidentified jellyfish. He had traveled to Penang Island for a vacation and stayed at a hotel by the beach. According to the patient, at 0635, while performing a religious ritual, he walked into the sea to the waist level, when he suddenly felt an electric current‒like pain over both thighs, left flank, and left forearm. He did not see the offending agent. He complained of severe pain over the affected areas, with chest discomfort and breathlessness. Hotel workers attended to him and sprayed the affected areas (most likely with vinegar). At a nearby private hospital 1 h 35 min after the sting, his initial vital signs were blood pressure 136/104 mm Hg, heart rate 102 beats/min, SpO2 100% on nasal cannula 3L/min oxygen, and pain score 9/10 on verbal numerical rating scale (VNRS). Vinegar soap was applied to the affected area. He denied any comorbidities, medication, or allergies. He was given IV pethidine 50 mg, parecoxib 40 mg, pantoprazole 40 mg, hydrocortisone 200 mg, tramadol 50 mg, intramuscular chlorphenamine 10 mg, and oral paracetamol 1 g. He did not want to be admitted because of logistical reasons and was discharged against medical advice with oral etoricoxib, tramadol, and diclofenac gel. No skin sampling (scraping/biopsy) for nematocyst was obtained for analysis.
The following day, he traveled by public transportation to a teaching hospital in Kuala Lumpur 377 km south of the initial treating facility, 30 h after the initial incident. He complained of persistent pain over his thighs and left flank, generalized body ache, fever, mild drowsiness, numbness over the affected limbs, sore throat, and abdominal cramps. Vital signs at presentation were temperature 36.5°C, blood pressure 139/85 mm Hg, heart rate 83 beats/min, SpO2 97%, respiratory rate 18 breaths/min, and pain score 7/10. Examination of the cardiovascular, respiratory, and abdominal systems was normal. Examination of the sting area showed red to purplish skin lesions (Figure 1a).
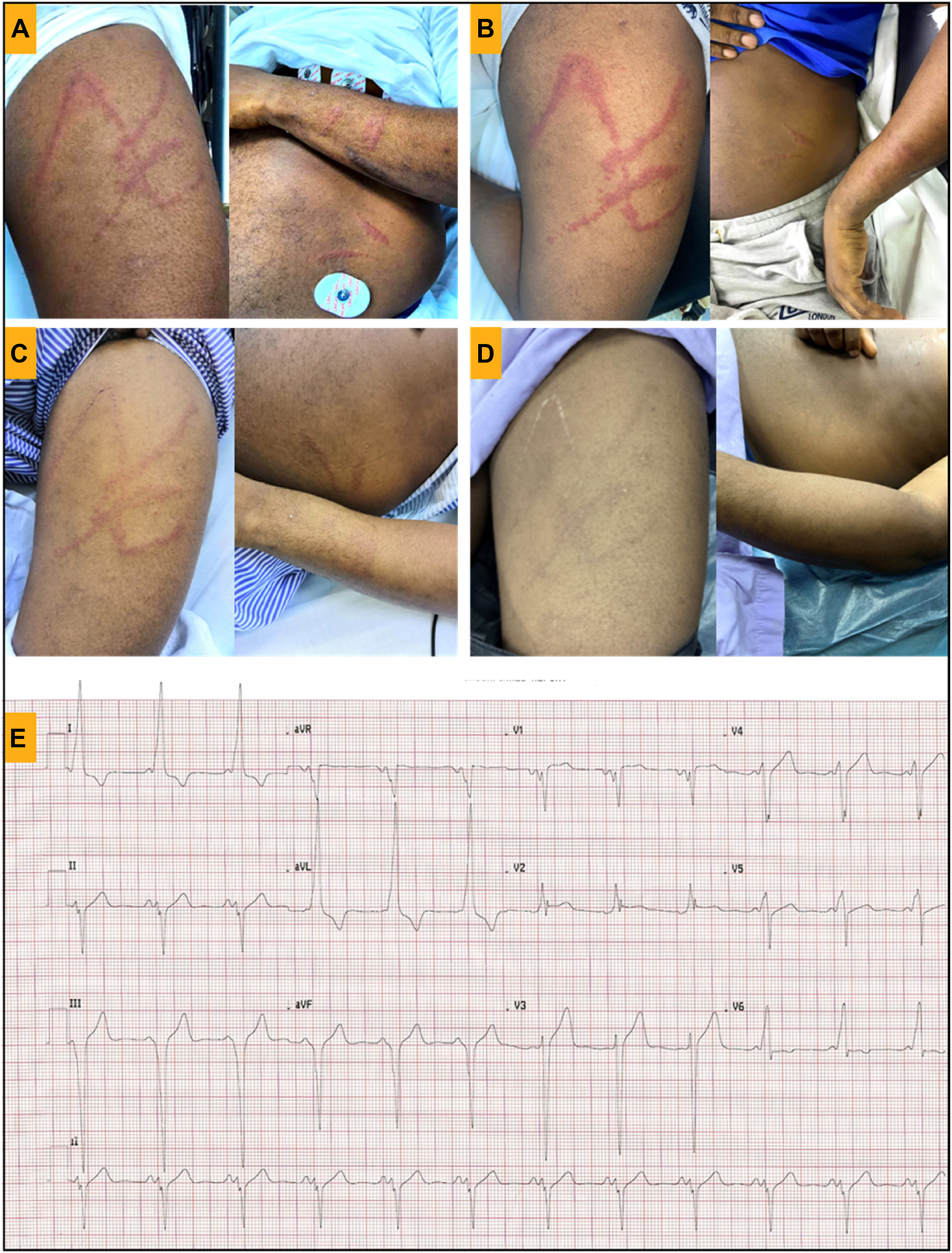
Jellyfish sting lesion over left anterior thigh, forearm, and flank at A, 30 h; B, 62 h; C, 140 h; D, at 30 d after the incident; E, electrocardiograph showing Wolff-Parkinson-White with short PR interval and delta waves, with secondary ST segment changes and left ventricular hypertrophy according to limb leads criteria.
A 12-lead electrocardiogram (ECG) demonstrated features of Wolff-Parkinson-White (WPW), with a short PR interval and delta waves, secondary ST segment changes, and left ventricular hypertrophy according to limb leads criteria. Cardiac ultrasound revealed good cardiac contractility with no regional wall hypokinesia and a thickened left ventricular wall. The patient was given IV tramadol 50 mg and saline hydration. Blood investigation showed elevated creatine kinase (CK) level of 647 U/L, with troponin I level at <10 pg/nL (Table 1). The chest radiograph was normal. Repeat ECG showed no evolving changes.
Laboratory investigation of the patient from admission to the emergency department until discharge
CRP, C-reactive protein; CK, creatinine kinase; PT, prothrombin time; aPTT, activated partial thromboplastin time; INR, international normalized ratio; ALP, alkaline phosphatase: ALT, alanine transaminase.
The Remote Envenomation Consultancy Service (RECS) was consulted, and he was referred to the cardiology team. Once again, he did not want to be admitted and discharged himself against advice with an outpatient cardiology clinic appointment. The patient returned to the emergency department 22 h later with persistent pain over the affected sites (Figure 1b). He denied chest pain or breathlessness. Vital signs and physical examination were unremarkable. An ECG showed persistent WPW changes, and the troponin level was <10 pg/nL. However, the CK level increased to 1216 U/L. He was admitted for observation and pain management, and his condition gradually improved. The CK level on the following day was 763 U/L, and his ECG remained unchanged. He was discharged after 2 d of admission with a final CK level of 392 U/L with an outpatient echocardiography and cardiology clinic appointment (Figure 1c). A review of patient progress 30 d after injury did not reveal any persistent signs of envenomation or chest pain. The wound from the sting has healed with minimal scarring (Figure 1d). A repeat ECG showed no changes (Figure 1e).
Discussion
Few jellyfish sting cases have been reported in Malaysia, although it is the most common marine envenomation consulted to RECS (unpublished data). Being in proximity to Thailand and the Philippines, where 20 to 50 sting-related deaths were reported to occur annually, a similar problem is likely to occur in Malaysia.11-12 To date, in regular on-site surveys by the Centre for Marine and Coastal Studies (CEMACS) of the waters around Penang Island, Chironex fleckeri and C yamaguchii have yet to be identified. 1 The Cubomedusae that have been identified were C buitendijki and Morbakka spp. C yamaguchii is indigenous to Sabah waters. There is however an abundance of C chinensis in the waters of Penang Island. This finding is also supported by regular specimens collected by local fishermen of Penang.
Both Irukandji and Irukandji-like syndrome have been diagnosed among jellyfish sting patients in Langkawi and the west coast of peninsular Malaysia. 10 Irukandji syndrome is a complex of symptoms and signs indicating a particular type of envenoming and can be caused by a variety of jellyfish belonging to multiple genera. Although Irukandji syndrome was originally described after stings by Carukia barnesi, other jellyfish such as Morbakka spp, including Morbakka fenneri, can cause similar presentations.13,14 Irukandji syndrome is described as a minor local sign and symptom with the hallmark of severe musculoskeletal pain occurring after the sting from C barnesi jellyfish.2,14 Some patients with identified nematocysts consistent with C barnesi have reported rapidly developing dyspnea and musculoskeletal pain. 15 Symptoms of Irukandji syndrome typically occur within 30 min but can range anywhere from 5 to 120 min.14,16 The rapid onset of symptoms is attributed to the length of the penetrant tubules, which allow the toxins from the venom to enter directly into pierced capillaries. 17 Irukandji syndrome typically presents with causes delayed symptoms compared with those caused by multitentacled box jellyfish stings, that is, the victim is often out of the water by the time they recognize they have been stung by a four-tentacled box jellyfish compared with those stung by multitentacled box jellyfish who develop symptoms immediately. Local symptoms are typically mild stinging pain at the affected site within seconds with later papular erythematous skin lesions, approximately 2 cm in diameter. 16 The recent publications on “Irukandji-like” cases from Thailand reported clinical presentations that are quite different from those of Irukandji-like syndrome reported in Australia. 18 Most of the clinical manifestations in this report were not consistent with those of Irukandji-like syndrome and may represent a new syndrome of jellyfish envenoming, quite possibly distinct from Irukandji.
The skin lesion in our patient appears to be similar to one of the cases previously described as “Irukandji-like” syndrome in Thailand. 18 Recent cases consulted to RECS have also observed similar skin lesions with confirmation of nematocyst sampling pointing to Chrysaora spp sting. The skin lesion from a large-sized Morbakka spp sting may also appear similar to that in the case presented. This is most likely due to the broad ribbon-like tentacles of these species rather than the thin, vermicelli-like tentacles of smaller-sized four-tentacled box jellyfish species. There was immediate onset of extensive pain over a large area of the presumed tentacle contact, with delayed manifestation of abdominal cramps and generalized body aches. These presentations are not strictly consistent with “Irukandji-like” syndrome. Instead, they may represent a new type of jellyfish envenomation, perhaps closer to a multitentacled box jellyfish (Chironex spp) envenomation, but possibly distinct from that as well. The later systemic features including the cardiac features would fit just as well as a slightly atypical box jellyfish envenomation. It is important to acknowledge the difference between classical Irukandji syndrome and clinical presentation mimics possibly from other jellyfish species that should not have been labeled as “Irukandji-like.”9,10,18 The patient’s clinical course was not consistent with the classic interpretation of Irukandji syndrome. Besides experiencing immediate pain and having significant skin markings, the described clinical evolution does contain some elements consistent with mild-to-moderate manifestation of Irukandji syndrome, such as dyspnea, hypertension, abdominal cramps, severe myalgia, and other uncommon effects that may be associated with catecholamine storm.19,20 Anxiety following the sting incident may also contribute to the confusion.
ECG changes and elevated cardiac marker levels have been reported in box jellyfish envenomation. 21 -24 To date, no WPW changes on ECG have been documented in cases of jellyfish sting envenomation. The WPW feature in our patient appears to have persisted and therefore might have been pre-existing. This feature is not consistent with the West African repolarization variant and is most likely not related to the jellyfish sting envenomation. However, the chest discomfort may have been triggered from catecholamine surge, causing coronary vasospasm. Therefore, such an abnormality incidentally discovered following a jellyfish sting should be documented and closely monitored.
Treatment for jellyfish sting is mainly supportive, and to date, no specific antivenom is available except that for C fleckeri. Therefore, preventive measures are the best option, and these include avoidance or minimization of contact, especially during the jellyfish season. 12 Full-body Lycra stinger suits or the equivalent have been shown to provide adequate protection from stings.25,26 Topical sting inhibitors and thick layers of petroleum-based ointments may help in minimizing sting frequency and severity.
Initial first aid should consist of removing the victim from the water in order to prevent further contact with jellyfish tentacles and risk of drowning. The intention of first aid for jellyfish sting is to decrease venom exposure as soon as possible and provide a reasonable measure of pain relief prior to arrival at a medical facility. Household vinegar (containing acetic acid 5%) is traditionally recommended to deactivate nematocysts prior to removal of remaining tentacles on the skin. However, this long recommended first aid has recently become controversial because of an in vitro finding of the effect on nematocyst discharge upon contact with vinegar. 27 Different species of harmful jellyfish are present in Penang waters, and therefore, vinegar alone may not be appropriate for first aid. 28 -31 Seawater is recommended as a rinsing agent, and lidocaine spray has been shown to relieve pain as well as prevent nematocyst discharge. 28 First responders and prehospital care providers should be aware of recommended first aid measures for stings by the locally relevant jellyfish species. 31 The use of heat has been shown to relieve pain; however, the availability on site could limit its use. Cold compression for noncubozoan sting has been shown to have a similar analgesic effect as heat application, and it is likely more readily available and accessible at the beach. 32
Public awareness of the appropriate preventive methods against jellyfish sting and health-seeking behavior needs to be encouraged in Malaysia. Healthcare providers in Malaysia need to be aware of harmful jellyfish sting envenomation management. Careful identification and documentation of clinical effects in comparison with reported syndromes can provide helpful guidance for ultimately determining optimal clinical management even for unidentified species that cause semi-identifiable envenomation. An interagency collaboration on jellyfish surveillance and related injuries could enhance policies and guidelines on local management and train emergency response teams in high-risk areas.
Footnotes
Acknowledgments
The authors thank Professor Colin Robertson (Edinburgh) and Mr Idwal Jones (Hamburg) for reviewing this article.
Author Contributions: conceptualization (AKI); validation (NKS, GA, SMJ, MMH, AKI); resources (NKS, AKI); writing ‒ original draft (NKS, AKI); writing ‒ review and editing (NKS, GA, SMJ, MMH, AKI); visualization (NKS, AKI); supervision (SMJ, AKI). All authors approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.