
Abstract
Crocodile bites lead to fatal and nonfatal outcomes in humans. Mugger crocodiles (Crocodylus palustris) and saltwater crocodiles (Crocodylus porosus) are common in India. Most crocodile bites can cause severe injuries, especially to the extremities, due to the substantial bite force of the crocodile, which typically leads to extensive tissue damage, fractures, amputations, and vascular injuries. We report the case of a crocodile bite victim who presented with features of acute limb ischemia, was found to have vascular thrombosis of the common femoral artery, and was experiencing complete compression of the femoral vein due to external vascular compression by a hematoma. We discuss various injury mechanisms sustained in crocodile bites and the roles of point-of-care ultrasound and continuous tomography angiography, which could help identify these injuries. After thrombectomy and hematoma evacuation the patient recovered and was discharged without any physical dysfunction.
Introduction
Humans receiving bites from wild animals are often the result of 2 things: self-defense by the animal, or the victim is mistaken as the animal’s prey as the creature hunts for food. 1 A multicenter study sponsored by the World Health Organization reported an annual incidence of animal bites in India of about 2%, with a higher incidence in rural areas and among poor or low income groups. 2 Human–crocodile conflict is a rare event, and crocodilian attacks on humans are challenging to quantify. Though crocodile bites on humans are common in Africa, Australia, and South and Central America, they are relatively uncommon in India, especially in the southern regions of country. One possible reason for the decreased total incidence of crocodile bites might be that they occur in very remote areas and may go underreported. India’s most common crocodile habitats are in deep water rivers, lakes, and artificial bodies of water—they are found in various regions of India, including parts of Andaman and Nicobar Islands (Figure 1). Crocodiles are usually aggressive during the winter mo of November and December, when their mating season starts. The risk of human–crocodile conflict has increased as a result of increasing human activity in rivers and their natural habitats. 1 There is little published literature outlining the initial assessment and management of crocodile bites. 1 We report a rare case of a crocodile bite in an adult patient who sustained a limb-threatening vascular injury due to extrinsic compression of common femoral artery by a hematoma.
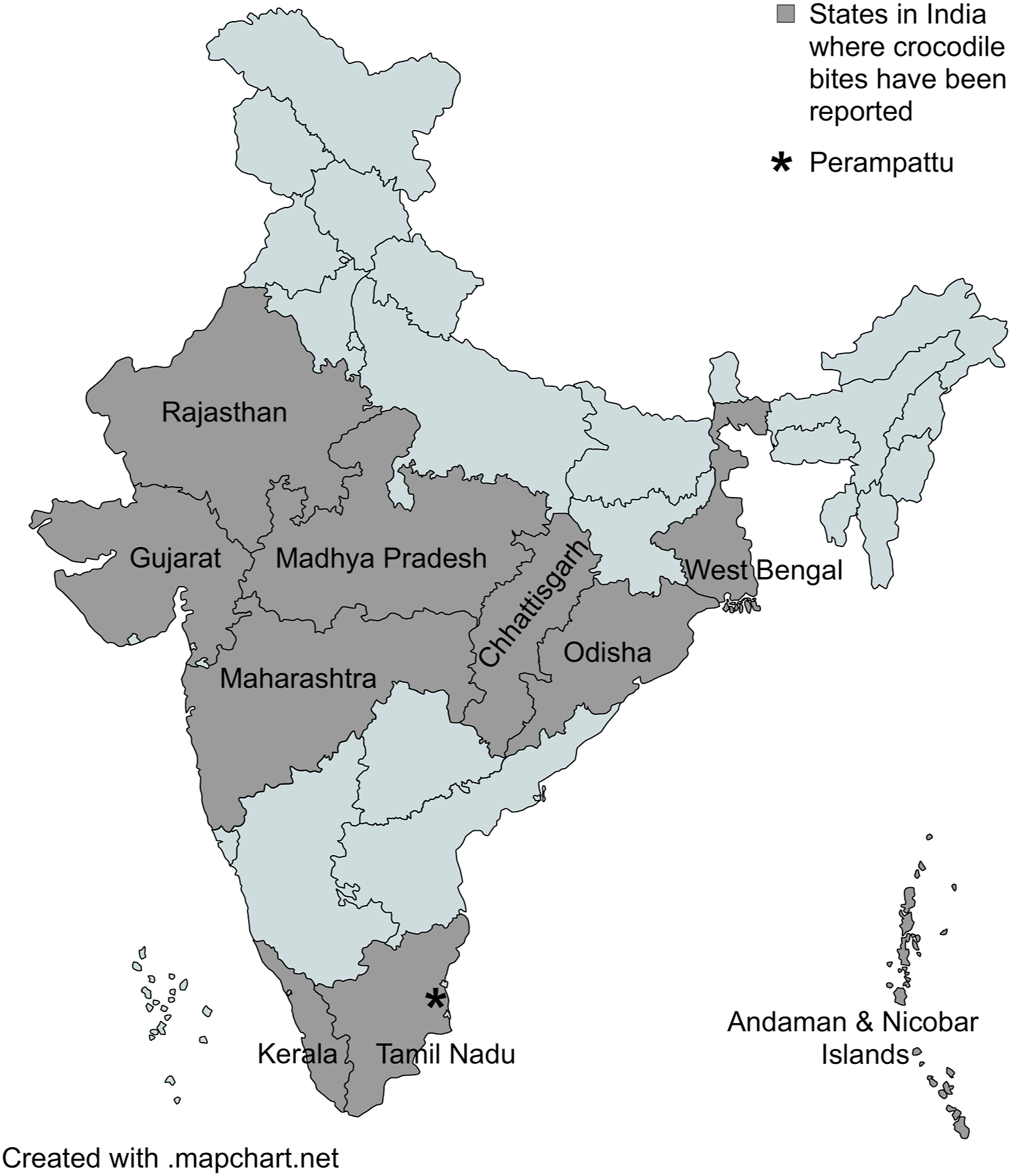
Map of India showing regions where crocodile bites have been reported to date, and location of Perampattu village (marked as ∗) where the patient sustained the attack.
Case Report
A 50-y-old man was brought to the emergency department after being bitten by a 3-m-long crocodile on his left lower limb and iliac region while washing himself by the river banks at 1630. He was taken to a nearby tertiary care hospital where his wound was dressed and his left lower leg was placed in a splint before he was then sent to our trauma center via ambulance. On arrival at 1904, he was conscious and oriented, with a Glasgow Coma Scale of 15, pulse rate of 74 beats·min-1, blood pressure of 140/80 mm Hg, respiratory rate of 14 breaths·min-1, O2 saturation of 98% on room air, and finger capillary refill time of less than 3 s. On local examination, 2 significant lacerations were found in the left iliac region: the first being 3×2×1 cm (length×depth×width), and the second being 4×3×1 cm (length×depth×width). In addition, the patient had a laceration measuring about 3×2 cm (length×width) in the anterolateral aspect of left thigh and 3 other puncture wounds in the anterolateral left thigh (Figure 2A). The patient also had a 1×1 cm (length×width) laceration in the lateral aspect of left knee and 2 lacerations (8×5 cm and 2×1 cm, length×width) in the lateral aspect of the left leg (Figure 2B). Pulses in the left-sided femoral, popliteal, anterior tibial, posterior tibial and dorsalis pedis arteries were not felt. However, pulsations were felt in the right lower limb distal artery.

(A) Bite wounds on left thigh and inguinal region and (B) bite wounds on left knee and left leg.
The wound was cleaned thoroughly and dressed, tetanus toxoid and tetanus immunoglobulin were administered, and the patient was given ceftriaxone and metronidazole as empiric antibiotics. Our bedside point-of-care ultrasound revealed no color flow in the left popliteal, anterior tibial, posterior tibial, and dorsalis pedis arteries—right femoral artery color flow was present. While checking for color flow in the left femoral artery, we found a hematoma (6.2×2.5 cm) in the muscular plane that was completely compressing the left common femoral vein, which had collapsed and was also compressing the left distal common femoral artery, as evidenced by no color flow in the artery distal to the hematoma (Figure 3). No vascular contrast extravasation was seen on computed tomographic (CT) angiography, but a filling defect was noted in the left distal external iliac artery and proximal common femoral artery (Figure 4). Our vascular team was informed immediately and the patient was taken to the operating room. Intraoperatively, no vascular injury was noted, but a soft thrombus was found in the left common femoral artery extending into the left external iliac artery. This was possibly due to extrinsic compression and stasis caused by the overlying hematoma. Thrombectomy was performed and the hematoma was evacuated—intraoperative wound culture was not taken. The postoperative course was uneventful. The patient received 10 d of ceftriaxone and metronidazole in addition to wound care. No signs of infection were noted in the postoperative period. Due to the patient’s multiple wounds, he remained in the hospital for 2 wk and was fully ambulatory at discharge.
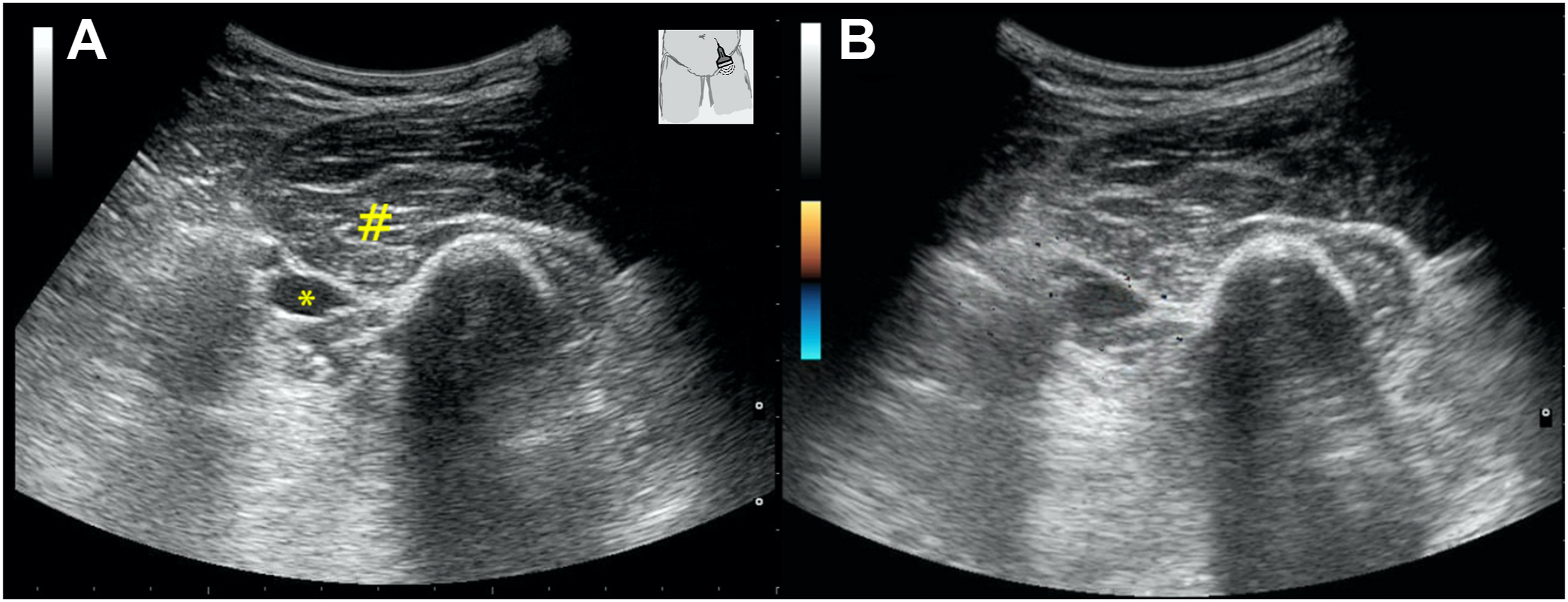
(A) Ultrasound image showing hematoma (marked as #) compressing left common femoral artery (marked as ∗). (B) Color Doppler image showing no color flow in the left common femoral artery.
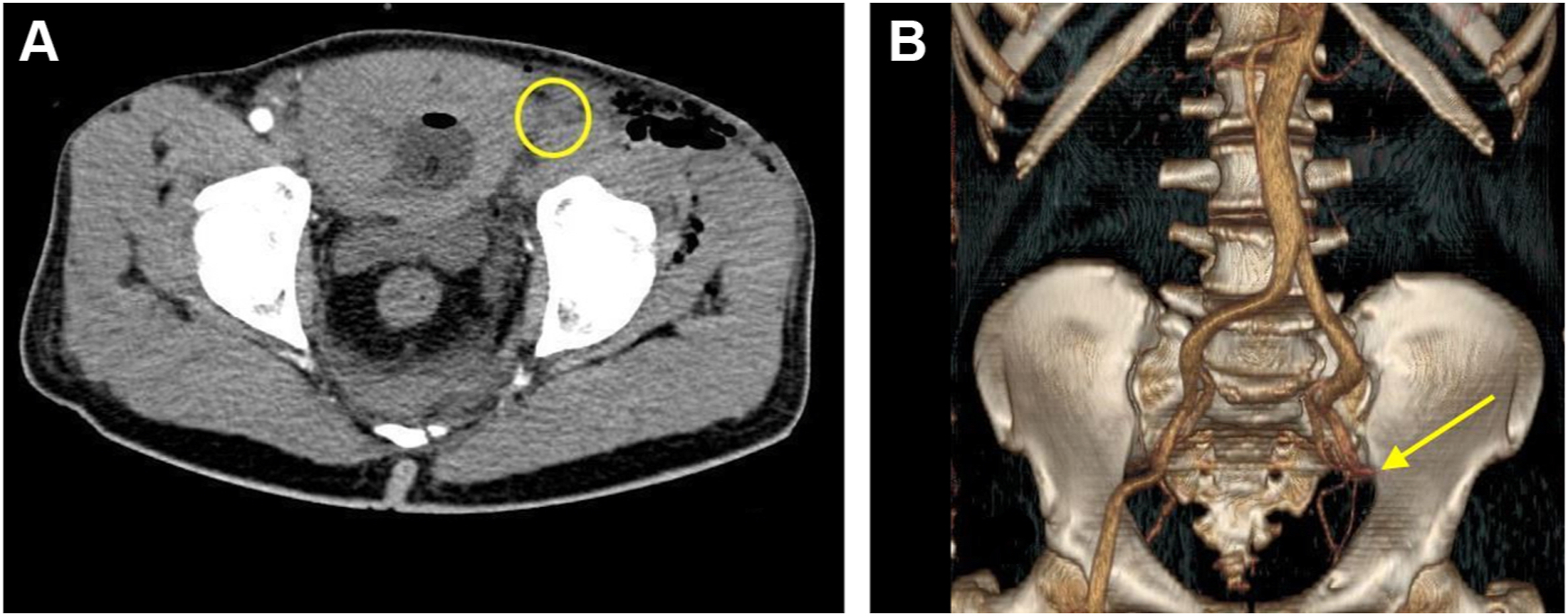
(A) Computed tomographic angiography showing filling defect in the left distal external iliac and left proximal common femoral artery (marked with yellow circle). (B) 3-dimensional reconstructed image showing complete cutoff of flow beyond external iliac (marked with a yellow arrow).
Discussion
There are 23 different species of crocodiles worldwide of which the mugger crocodile (Crocodylus palustris) and saltwater crocodile (Crocodylus porosus) are common in India. Crocodiles are more commonly distributed in the Andaman and Nicobar Islands, West Bengal, Kerala, Odisha, Gujarat, Chattisgarh, Rajasthan, Madhya Pradesh, Maharashtra, and Tamil Nadu (Figure 1). 3 Our patient sustained a bite from a 3-m-long crocodile along the banks of the Kollidum River in Tamil Nadu, a state in the southern part of India where mugger crocodiles are commonly reported. 4 Most adult crocodiles are >3-m-long and have enormous biting capacity. The muscles used for opening their mouth are weak but the force with which they bite is powerful enough that it makes it very difficult for the victim to escape. Of all the 23 species of crocodiles, the measured average bite force exerted by sexually matured adults was found to range between 900 to 8983 N (202–2019 lb). 5 Even though most crocodile bites are reported as unprovoked, the true nature of these attacks is uncertain. 1 Humans often encounter crocodiles when they bathe and wash clothes along the banks of a river. Cases of human–crocodile encounters have also been reported among fishermen and people snorkeling. 1
The mechanisms of injury in crocodile attacks include deep puncture and tearing wounds from their long sharp teeth as well as blunt injuries from the crocodile’s strong bite force and battering from the tail of the animal. 6 The penetrating force can cause penetrating vascular trauma and hematomas, and the shearing forces can cause extensive tissue damage, blunt vascular trauma, fractures, and amputations. The anatomic distribution of wounds commonly include injuries to the extremities, which is consistent with the attack behavior of the crocodile that involves striking from below or from the side. In fact, a retrospective review of crocodile bites in southern Malawi found that >80% of soft tissue injuries were in the extremities. 6 In our case, a similar pattern was seen with injuries in the left lower limb, with multiple penetrating injuries probably caused by the long conical teeth of the animal.
Prehospital management is vital in crocodile bite victims since these bites typically occur in remote areas and transport to the hospital may be delayed. Therefore, emergency medical services personnel should focus on immediate hemorrhage control, immobilization of affected body part, early wound decontamination, and rapid transport to a trauma center. Currently, there are no data about the utility of prehospital antibiotics for animal bites. Although a sepsis trial of prehospital antibiotics did not show any survival benefit when antibiotics were administered in an ambulance, recent recommendations and studies have suggested a possible benefit for early antibiotics administration. 7 –9 Hence, early antibiotics may be considered when longer transport time is anticipated. In addition to the injuries caused by bites, there are case reports of victims being dragged into water and sustaining complications due to drowning. 10 Emergency medical services teams should also focus on airway stabilization and starting the patient on oxygen if patient is hypoxic.
As with all trauma patients, routine primary assessment and stabilization after advanced trauma life support protocols must be followed when crocodile bite victims present to the emergency department. Due to the possibility of extensive soft tissue injuries and vascular damage, these patients may present with profound hemorrhagic shock. Hemorrhage control and activation of massive transfusion protocols are critical steps in managing these patients. To prevent further vascular damage, early immobilization of the injured limb is advisable. Copious wound washing and emergent debridement should be done for all wounds to mitigate the possibility of wound infections in crocodile bite wounds. Multiple microorganisms can grow in the wound due to the unusual flora in crocodile teeth and the oral cavity—gram-negative bacteria and anaerobes are commonly found.6,11 Pseudomonas pseudomallei, Pseudomonas aeruginosa, Enterococcus sp, Aeromonas hydrophila, Enterobacter agglomerans, Citrobacter diversus, and Clostridium species are the main organisms that have been isolated from wound swabs of studies of crocodilian bite microbiology.12,13 Antibiotic coverage must cover gram-negative rods and anaerobic organisms. Doxycycline should specifically be included in cases of crocodile bites because Vibrio vulnificus has also been shown to grow from the wounds. 11 Wounds sustained by crocodile bites are usually contaminated, therefore every patient with an unknown history of immunization or <3 doses has to be given tetanus toxoid and tetanus immunoglobulin.
Multiple scoring systems like the mangled extremity severity score (MESS); predictive salvage index; nerve injury, skeletal injury, shock, and age score; limb salvage index; and Hannover fracture scale have been suggested for predicting the extent of injuries in extremity trauma. 14 MESS scoring is commonly used to estimate the viability of an extremity after trauma and to determine need for salvage vs empiric amputation (Table 1).15,16 In our patient, the score was calculated as 7, predicting a low likelihood of limb viability. Using the MESS scoring system, this assumes that the crocodile bite has been a high-energy mechanism.
Crocodile bites can present with both blunt and penetrating vascular injuries. 1 Duplex ultrasonography and CT angiography are the common diagnostic modalities used to evaluate a patient with a suspected vascular injury. In our case, although we initially suspected vessel injury (given the penetrating nature of the wound), intraoperatively, we found that a large hematoma had compressed the vessel, causing stasis and soft thrombus formation, which caused pulselessness. At this point, the use of point-of-care ultrasound was pivotal. The ultrasound showed a hematoma that completely occluded the femoral vein as a result of extrinsic compression and compression of the common femoral artery (CFA). In this case, it appeared that extrinsic compression and stasis had caused an acute thrombus to form in the CFA. The ultrasonographic appearance of an acute thrombus has been reported to be hypoechoic or anechoic.17,18 The absence of color flow in color Doppler of the CFA confirmed this hypothesis in our patient. Acute compartment syndrome after a crocodile bite has been reported, leading to vascular compression and presenting with features of acute limb ischemia. 19 The anterior compartments of the thigh and lower leg are the most common locations for compartment syndrome in the lower extremity. However, in our patient, other clinical features of compartment syndrome (such as pallor, paresthesia and paralysis) were absent. Direct extrinsic arterial compression could have resulted in a similar presentation to that seen in our patient, and has been reported in the literature. The literature has documented 1 case report of extrinsic femoral artery occlusion after internal fixation of an acetabular fracture and 3 other cases of thrombosis after extrinsic iliac artery occlusion post acetabular fracture repair. 20 A few other rare cases of extrinsic vascular compression by external bodies have been reported, including lymphangioma, neurofibroma, fecal impaction, and leiomyoma. 21 –23
Apart from the penetrating vascular injury reported in crocodile bites, they can also present with blunt vascular injuries due to the unique mechanism of injury. There are multiple case reports of injuries to the external iliac, common femoral, and common iliac arteries as a result of blunt trauma without concomitant bone fractures in patients who sustained road traffic accidents. 24 One such reported injury is motorcycle-scooter-handlebar syndrome, where the vascular injury occurs without any bony fracture. 25 The mechanism of this injury has been thought to be due to intimal tear or inner circumferential intimal fracture. The inguinal portion of the CFA is tethered by arterial branches, periadventitial connective tissue, and femoral sheath, and this portion is vulnerable to compression against the superior pubic ramus. Hence, similar injuries should also be suspected when managing patients who present with crocodile bites.
Conclusions
The key elements for managing crocodile bite injuries—both in prehospital and in-hospital settings—should focus on hemorrhage control, immobilization of extremities, and early identification of vessel injuries caused by the enormous bite force. Both blunt and penetrating vascular injuries are commonly seen with crocodile bites. Extrinsic vascular compression causing arterial thrombosis also needs to be evaluated as a potential differential diagnosis. Point of care ultrasound and CT angiography are very useful tools in identifying these injuries. In addition to maintaining focus on advanced trauma life support guidelines, emergency care providers must focus on thorough wound washing, debridement, and appropriate antibiotic coverage for gram-negative rods and anerobic organisms due to the unusual oral flora of crocodiles.
Footnotes
Acknowledgements
Author contributions: Study concept and design (AK, SMA); drafting of the manuscript (AK, SMA, EG, PK); critical revision of the manuscript: (AK, SMA, GR); approval of the final manuscript (all authors).
Financial/Material Support: None.
Disclosures: None.
Consent for publication: The patient has given informed consent for publication of the case report and accompanying images.