
Abstract
Introduction
The Maltese Islands are a small archipelago of islands at the center of the Mediterranean where seaside activities are popular year-round among locals and tourists alike. We frequently treat injuries caused by sea creatures, jellyfish stings being the most common. Similar reports are seen in countries with similar climates and seascapes.1,2 We present a case of a child who sustained a marine envenomation caused by an unknown tentacled organism. In such cases, it is often difficult to find the causative organism, and the healthcare practitioner has to rely on the patient’s description of events and clinical signs and symptoms.
Case Report
A 4-y-old boy presented to the pediatric emergency department (PED) with significant upper lip swelling, acquired while he was swimming in the sea off the coast of Malta. The boy had been swimming along the rocky shore when he returned to the shore crying after a tentacled creature had stung him. He immediately developed facial swelling. His mother took him to a clinic, where he was given 5 mg promethazine orally and transferred to PED by private vehicle.
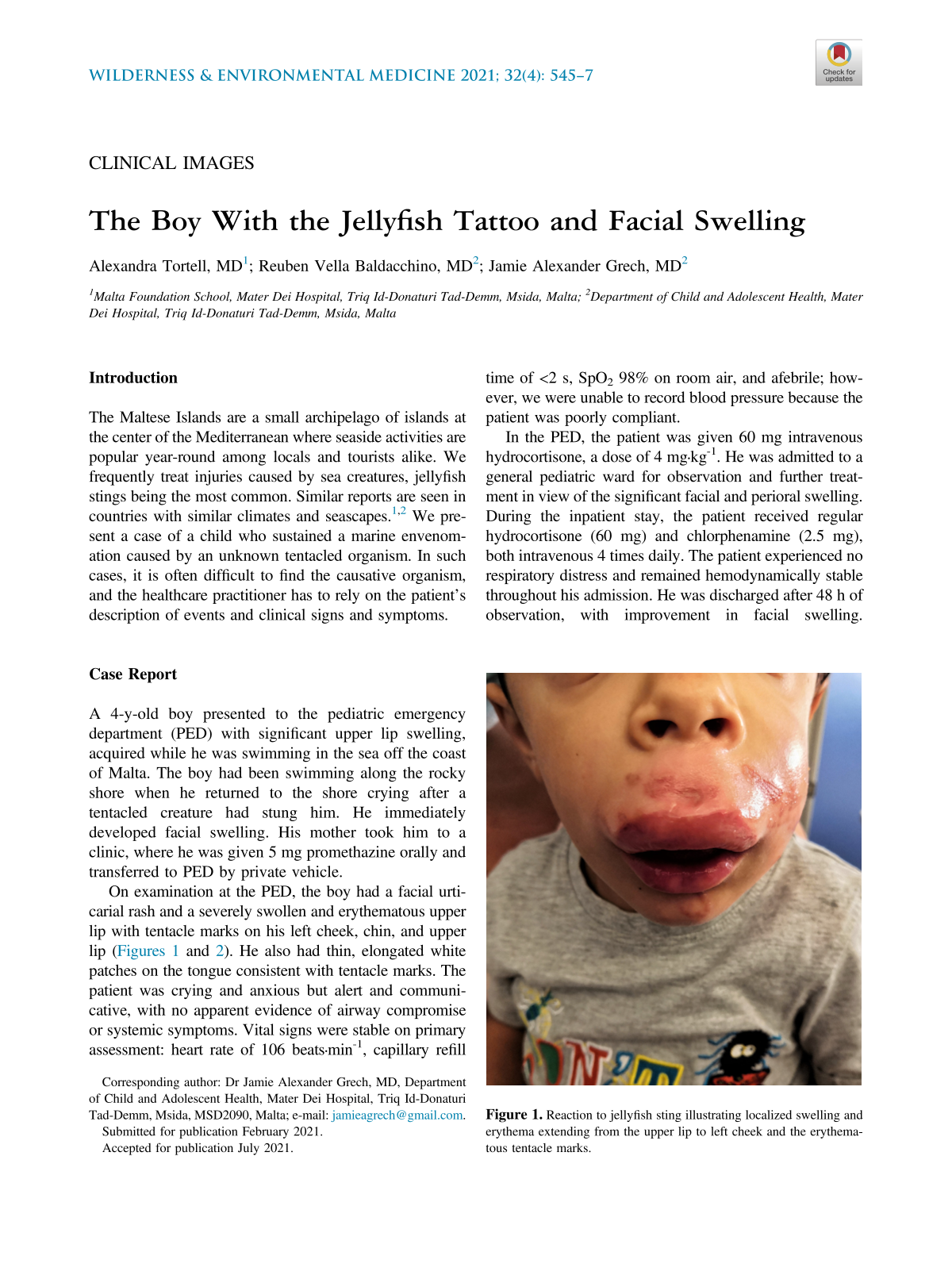
On examination at the PED, the boy had a facial urticarial rash and a severely swollen and erythematous upper lip with tentacle marks on his left cheek, chin, and upper lip (Figures 1 and 2). He also had thin, elongated white patches on the tongue consistent with tentacle marks. The patient was crying and anxious but alert and communicative, with no apparent evidence of airway compromise or systemic symptoms. Vital signs were stable on primary assessment: heart rate of 106 beats·min-1, capillary refill time of <2 s, SpO2 98% on room air, and afebrile; however, we were unable to record blood pressure because the patient was poorly compliant.

Reaction to jellyfish sting illustrating localized swelling and erythema extending from the upper lip to left cheek and the erythematous tentacle marks.

Reaction to jellyfish sting illustrating localized swelling and erythema of the upper lip, particularly when compared to the lower lip. Tentacle marks seen on the chin and left cheek.
In the PED, the patient was given 60 mg intravenous hydrocortisone, a dose of 4 mg·kg-1. He was admitted to a general pediatric ward for observation and further treatment in view of the significant facial and perioral swelling. During the inpatient stay, the patient received regular hydrocortisone (60 mg) and chlorphenamine (2.5 mg), both intravenous 4 times daily. The patient experienced no respiratory distress and remained hemodynamically stable throughout his admission. He was discharged after 48 h of observation, with improvement in facial swelling. Discharge medications were cetirizine 2.5 mg twice daily and prednisolone 30 mg daily for 3 d.
Discussion
Jellyfish are pervasive across many regions and are responsible for a large range of aquatic human envenomations. Environmental changes in sea temperatures, pH, and salinity have resulted in changes in the distribution of jellyfish and lengthening of reproductive periods, resulting in a greater number of invasive species causing greater numbers of human envenomations.
The effects of cnidaria envenomation largely depend on the species responsible; however, they can be associated with clinical features ranging from local pain, vesicular or urticarial eruptions, itching, erythema, edema, and lymphadenopathy to widespread systemic features such as anaphylaxis and cardiac arrest. 3 Cardiovascular collapse can occur secondary to a phenomenon known as Irukandji syndrome, whereby systemic manifestations of muscle spasm, severe sweating, hypotension, and cardiac failure occur 20 to 30 min after envenomation. This is thought to result from systemic catecholamine excess, but the exact mechanism is poorly understood. 3
Nematocysts stored in cnidocytes found in the tentacles of jellyfish are responsible for the toxic effects seen after contact with venomous species. There can be up to several billion nematocysts, 4 which, upon mechanical stimulation of the tentacle, uncoil and penetrate dermal and epidermal skin layers within a fraction of a second. The nematocyst thread is immersed in a collection of antigenic proteins and enzymes that are responsible for the variety of clinical features after exposure to toxic jellyfish tentacles. 4 Multiple variables, relating to both the victim and the jellyfish, affect the extent of envenomation. The victim’s body weight, the site of injury, and surface area of exposed skin, combined with the individual’s reactivity to the varying molecules released by a diverse range of nematocysts, determine the response to and extent of injury. 5
Initial contact is often associated with pain at the time of inoculation. The subsequent reaction may vary, with some individuals showing evidence of delayed type IV hypersensitivity reaction with delayed cutaneous manifestations and histologic features similar to those seen in allergen-mediated contact dermatitis. Anaphylaxis with subsequent shock is an uncommon yet well-described manifestation of jellyfish envenomation in previously sensitized individuals. 5 However, cross reactivity between sea nettle antigens and certain jellyfish such as Physalia physalis can result in anaphylactic reactions without previous exposure. 5
Sea anemones are closely related to jellyfish. Both belong to the phylum Cnidaria, with the most common species of the former in the Mediterranean being Amaranthus viridis. Anemones are more prevalent close to rocky shores and are frequently encountered in areas with swimmers. They are sedentary creatures that typically have iridescent yellow-green tentacles with purple tips. This makes anemones particularly attractive to swimmers, especially unsuspecting young children who end up being stung. 2 Similar to jellyfish, anemone tentacles possess nematocysts, which may release venom on contact. Sea anemone venom is typically less potent than jellyfish venom, but anemone tentacles are more numerous and may still cause severe reactions. 2
Management of both jellyfish and sea anemone stings is largely limited to seaside management and rarely requires hospital admission. The victim should be removed from the water to avoid complications while immersed. Airway, breathing, and circulation should be stabilized if necessary. Vinegar, or 5% acetic acid, should be used liberally for more than 30 s over the injured area. This deactivates the nematocysts, preventing further envenomation. Gentle removal of tentacles can be achieved by plucking remnants off the victim while taking care to minimize manipulation and further nematocyst discharge. The affected areas should be immersed in water of about 45°C to denature active enzymes found in venom. Appropriate analgesia should be used. Topical or systemic antihistamines and glucocorticoids can be used according to the extent of injury. 6 The use of promethazine as the initial antihistamine may have been a cause for concern because of the risk of respiratory depression, particularly in a patient at risk of respiratory failure. 7
Perioral cnidarian envenomation in the pediatric population has not been reported frequently. A retrospective review of all children presenting to a PED after jellyfish envenomation between 2010 and 2015 reported only 3 patients sustaining facial envenomations. One of these patients required hospitalization for 3 d for buccal swelling, dyspnea, and trismus. 8 Despite our patient’s uncomplicated inpatient course, prudence in such cases is necessary because of the risk of delayed cutaneous eruptions, placing the patient at risk of airway compromise. 3
In cases similar to ours when the envenomating species is unknown, one must rely on the patient’s description. However, the shape and type of skin lesion may provide a hint to the identity of the offending creature. Knowledge of the exact location, time of day, time of year, and depth, as well and the local distribution of dangerous organisms, is also helpful. 1
Conclusion
Seaside first aid could have mitigated the extent of injury, possibly preventing the need for hospitalization in this case. The use of promethazine at the primary healthcare facility in the setting of perioral edema increased the risk of respiratory depression. This, together with the risk of delayed cutaneous eruption, further emphasizes the need for observation and hospitalization.
Young children tend to be particularly prone to envenomation injuries because they have thinner skin than adults, particularly in sensitive areas such as the face, genitalia, and axillae. Education aimed at providing current information about first aid seaside management might improve treatment at the initial medical contact, possibly mitigating effects after envenomation.
Footnotes
Acknowledgment
The authors express their gratitude to the patient’s caring clinician, Dr Doriette Soler, for her support in our report of this case.