
Abstract
Introduction
Studies show that 40 to 60% of long-distance hikers on the Appalachian Trail experience musculoskeletal (MSK) injuries, but these studies are over a decade old. The increasing popularity of hiking and injury prevention advances warrant re-evaluation of injury patterns. We sought to determine the frequency of self-reported MSK injuries in long-distance hikers on the Appalachian Trail and associations with prehike conditioning and on-trail injury prevention strategies.
Methods
The Appalachian Trail Conservancy surveys registered hikers annually. Our orthopedic team added 10 questions specific to MSK injury, training, and equipment to the 2018 to 2019 electronic, cross-sectional Appalachian Trail Conservancy survey. Descriptive statistics and frequencies were calculated. Categorical variables were compared using χ2 analysis. Correlations were performed for associations between training and gear and MSK injury. Logistic regression assessed the effect of training on MSK injury. Statistical significance was set at P<0.05.
Results
Of 1295 respondents (52% response rate), 61% (n=791) reported MSK complaints; 28% (n=363) reported overuse/chronic MSK injuries, and 18% (n=238) reported acute injuries. MSK complaints resulted in 11% (n=147) stopping their hike. Respondents who did not train (13%, n=168) were significantly more likely to report an MSK injury (odds ratio 2.82; 95% CI 1.92–4.24; P<0.001). Strength training, stretch/yoga, and endurance training were associated with less injury (all P<0.001). Stabilizing footwear and poles/sticks were associated with fewer MSK complaints (all P<0.001).
Conclusions
Prehike training and hiking gear correlate with fewer injuries. Further research is warranted to elucidate whether promoting injury prevention strategies can reduce MSK injuries among long-distance hikers.
Introduction
Musculoskeletal (MSK) conditions affect 20 to 30% of people worldwide and are the main contributors to disability. 1 In the United States, MSK injuries account for more than 1.7 million hospitalizations, 23 million emergency or outpatient visits, and 40 million physician office visits per year. 2 Identifying injury patterns and prevention strategies in recreational activities with high MSK injury rates provides background data for the creation of injury prevention programs.
Hiking is the fourth most popular outdoor activity in the United States. 3 The activity is increasing in popularity, with 45 million people participating in hiking in 2017, up from 32 million in 2008.3,4 MSK injuries are common among long-distance hikers, a subset of the hiking population. An example of a long-distance hike is attempting to complete the Appalachian Trail (AT), which runs from Georgia to Maine, covering approximately 3540 km (2200 mi) with a total elevation gain/loss of over 141,580 m (464,500 ft). To complete the trail in 1 season, an average AT hiker will backpack 13 to 32 km (8–20 mi) per day over 5 to 7 mo.
Previous studies have attempted to evaluate injuries in this population. A survey of 180 long-distance hikers during the 1987 to 1988 AT hiking season found 62% of hikers reported extremity or joint pain. 5 Another study surveyed 280 participants who hiked along the AT for at least 7 d (duration of hike: 140±60 [mean±SD] d) in 1997. 6 Among these hikers, acute and overuse MSK complaints were reported by 43% and were the most common cause for discontinuing the hike. In 2006, a survey evaluated the effects of ultralight backpacking and less rigid footwear in 128 long-distance hikers, hypothesizing that improvement in hiking gear may have decreased MSK injury rates over the years. 7 MSK complaints were reported in 42% of participants.
Although these studies show a pattern of MSK injuries in long-distance hikers, the studies are over than a decade old and have limited sample sizes. Given advances in hiking gear and training knowledge, as well as a large increase in the numbers of hikers, recent MSK injury patterns may differ from those previously reported. The goal of this study was to determine the frequency of self-reported types of MSK injury among long-distance hikers on the AT and their association with prehike conditioning, stabilization gear, and recovery days. In addition, we assessed on-trail strategies such as hiking patterns—some hikers consider a northbound route on the AT a strategy for on-trail training by hiking flat lands before reaching higher elevations. As an exploratory survey, the objective was to ascertain a more current picture of MSK injuries and injury prevention strategies reported by AT long-distance hikers.
Methods
This was a cross-sectional electronic survey of AT long-distance hikers in the 2018 to 2019 season. Long-distance hikers on the AT have a choice to voluntarily register with the Appalachian Trail Conservancy (ATC) at the beginning of the hiking season. At the end of every season, the ATC emails a survey using SurveyMonkey Inc. to all registered hikers. The yearly survey created by the ATC includes questions about trail specifics such as hiking patterns, amenities, security, and trail crowding. Our orthopedic team added 10 questions specific to training and injury to the ATC yearly survey. We did not have input on the rest of the yearly survey. Participants answered a total of 57 questions. From the final survey, 15 questions were analyzed for this study (10 that were added and 5 that were part of the original ATC survey). The added questions can be found in Table 1. The remaining 42 questions were specific to trail conditions and amenities rather than hikers and were not used for this research. This study was deemed exempt by the Thomas Jefferson University institutional review board.
Survey questions from the ATC annual survey with absolute count and relative frequency of cases (%) using respondents per question as denominator
AT, Appalachian Trail; ATC, Appalachian Trail Conservancy.
The nonvalidated survey included structured and semistructured questions. Questions were not pretested. All registered long-distance hikers during the 2018 to 2019 AT hiking season were included in the study and contacted by the ATC through email for possible participation in the survey. Our research team did not have direct access to the hikers per the agreement with the ATC for the intent of preserving hiker confidentiality. Long-distance hikers on the AT who did not register with the ATC were excluded from the study. The survey invitation was sent once by email using the registered account information. There were no reminders or follow-up contact. The surveys were distributed electronically by the ATC in January 2019, coinciding with the ending of the hiking season. Survey results were collected by the ATC through the end of April to allow adequate time for response. Upon completion of the collection period, the ATC forwarded deidentified data to our orthopedic team for the purpose of analysis. No data were provided on the nonresponse group. Basic demographic information, such as age, sex, and body mass index, was not included.
Descriptive statistics and measures of frequencies are reported. Percentages were calculated from the number of the research cohort. All responses that were listed under “other, please specify” were reviewed by an orthopedic provider to determine MSK category. Those injuries that did not fall under MSK injury (eg, vitreous detachment) were not used for calculations. Pearson χ2 analysis was used to compare categorical variables. Simple logistic regression was performed to determine the effect of prehike training on having an MSK injury. Statistical significance was set at P<0.05. All statistical analyses were done using R Studio (Version 3.6.3, Vienna, Austria).
Results
A total of 2507 people registered as long-distance hikers on the AT in the 2018 to 2019 hiking season and were emailed an invitation to participate in the survey. Of those contacted, 1295 respondents completed the survey (52% response rate).
The majority of respondent start times coincided with the traditional start of the hiking season for the AT, which is February, March, and April. More respondents (70%, n=909) hiked a northbound route than hiked a southbound route (11%, n=142). Some backpacked different parts of the trail out of sequence, traveling both northbound and southbound during their hike (15%, n=190). There was no between-group difference in injury rate based on direction of hike (P=0.580).
When asked about what experience they had with hiking, 89% (n=1148) reported they had never attempted or completed a trip of similar length or duration, 6% (n=71) reported they had never hiked more than 16 km (10 mi) at a time, 13% (n=170) reported they had hiked 40 to 161 km (25–100 mi) in 1 backpacking trip, and 2% (n=28) reported they had completed a trail that was more than 805 km (500 mi) long before this hike.
In response to questions about training regimen, 13% (n=168) reported they did not train before starting the hike. Less than one-third of participants reported doing strength training (26%, n=338), stretch/yoga (19%, n=249), or endurance training (26%, n=338).
During a long-distance hike, backpackers can use “zero days” for recovery; they do not log any mileage on those days. When asked how many zero days each hiker took, 10% (n=123) reported none, 13% (n=173) reported 1 to 5 d, 15%, (n=192) reported 6 to 15 d, 2% (n=19) reported 16 to 30 d, and 3% (n=33) reported more than 30 d.
When asked about the type of stability equipment they used on the hike, 58% (n=749) had running or trail shoes, 24% (n=305) had hiking boots, 70% (n=902) had trekking poles or a walking stick, 20% (n=263) had a knee brace, 7% (n=90) had an ankle brace, and 3% (n=34) had a traction system for ice or other difficult terrain.
Knee injury/pain was reported by 37% (n=483) of respondents, and foot injury/pain was reported by 29% (n=374). Among other specific self-reported MSK injuries were ankle sprains (13%, n=174), medial tibial stress syndrome (11%, n=145), Achilles tendon injury/pain (12%, n=156), and IT band syndrome (9%, n=114) (Figure 1).
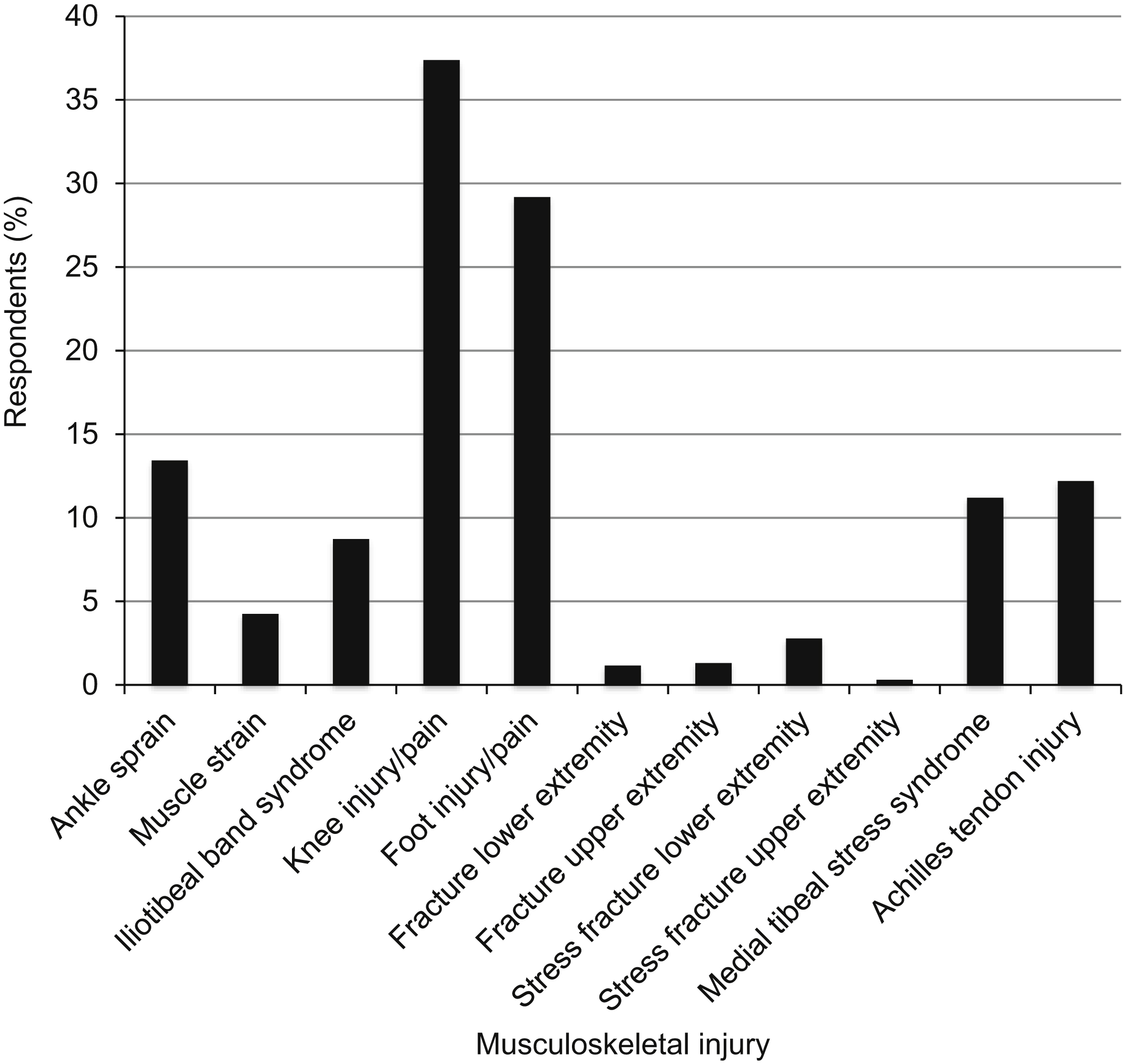
Musculoskeletal complaints reported by respondents.
When asked if they completed their planned hike, 55% (n=708) were successful and 42% (n=546) had to stop before completion. Injury was listed as the primary reason for discontinuing the hike for 11% (n=147) of participants (Figure 2).
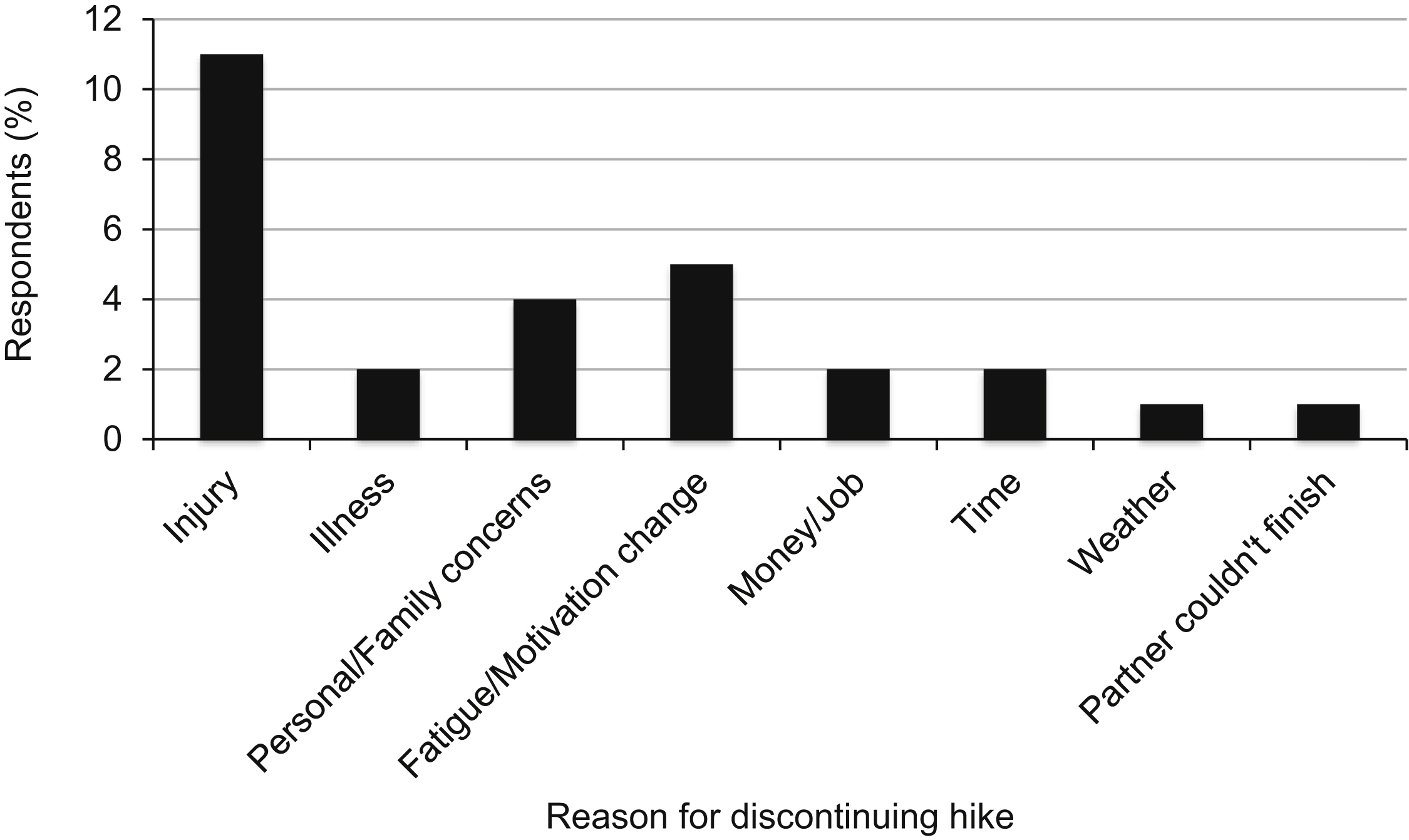
Top reasons reported by respondents for discontinuing the hike early among those surveyed who did not complete their planned hike.
When asked how long they took to seek treatment, 33% (n=430) did not seek treatment, 22% (n=289) sought treatment within 1 wk of the injury, 4% (n=53) sought treatment within 2 to 4 wk of the injury, 4% (n=53) sought treatment within 2 to 4 mo of the injury, and <1% (n=1) sought treatment after waiting more than 4 mo. When asked how long the injury took to heal from the onset of symptoms, 20% (n=263) reported less than 1 wk, 9% (n=118) reported 2 to 4 wk, 23% (n=294) reported greater than 1 mo, and 8% (n=109) reported it had not healed at the time of the survey. There were 26% (n=337) of respondents who reported they did not take any time off from hiking on the trail for an injury.
Hikers were asked to determine the longest total distance they completed before experiencing an injury. Of those surveyed, 3% (n=44) reported an injury in the first 0 to 16 km (0–10 mi), 13% (n=174) reported 18 to 80 km (11–50 mi), 6% (n=81) reported 82 to 161 km (51–100 mi), 16% (n=210) reported 163 to 805 km (101–500 mi), and 24% (n=312) reported completing greater than 805 km (>500 mi) before the injury.
Respondents who stated they did not train before the hike were more likely to report an MSK injury (80% vs 58%, P<0.001), an overuse/chronic injury (42% vs 26%, P<0.001), medial tibial stress syndrome (17 vs 10%, P=0.011), a lower extremity stress fracture (5 vs 2, P=0.036), or Achilles tendon pain/injury (18 vs 11%, P=0.019) (Table 2). They were more likely to report knee injury/pain (51 vs 35%, P<0.001) and foot injury/pain (38 vs 28, P=0.006). They were also more likely to report multiple injuries (P<0.001) (Table 2). Regression showed that respondents who did not train had greater odds of an MSK injury (odds ratio 2.82, 95% CI 1.92–4.24) that reached statistical significance (P<0.001).
Descriptive table comparing those who reported prehike training to those who reported not doing any prehike training
MSK, musculoskeletal.
Significant at P<0.05.
Correlations revealed that strength, stretch/yoga, and endurance training were associated with avoiding injury (all P<0.001). Stabilizing gear such as running shoes/trail shoes/hiking boots and trekking poles/hiking sticks were associated with less injury (all P<0.002) (Table 3). Specific injury types were correlated with a respondent discontinuing a hike early, including Achilles tendon injury/pain (P=0.02), ankle sprains (P=0.01), IT band syndrome (P=0.049), and medial tibial stress syndrome (P=0.03) (Table 4).
Musculoskeletal injuries associated with having to discontinue the hike
Significant at P<0.05.
Musculoskeletal injuries associated with having to discontinue the hike
Significant at P<0.05.
Questions used for the survey with response rates, absolute, and relative frequency using respondents per question as the denominator can be found in Table 1. Final calculations were completed after “other, please specify” categories were screened.
Discussion
Our research provided current data on self-reported MSK injuries in long-distance hikers on the AT and found an inverse relationship between prehike training and MSK injury. Identifying injury patterns and prevention strategies in recreational activities helps in the development of injury prevention programs, and this survey served as an initial step in that process.
In our study, knee injury/pain was reported by over one-third of respondents and was the most commonly reported site of MSK pain. Although earlier studies did not isolate complaints related to the knee, 1 study found that 43% of hikers reported acute joint pain, and another found 44% of long-distance hikers reported knee/ankle pain.5,6 Research evaluating lower limb kinematics and kinetic changes in participants carrying loads for prolonged periods of time found fatigue in the quadriceps muscles. 8 The fatigued muscles then were unable to effectively absorb impact forces, leaving the participants at increased risk of knee injury. This finding may explain the high rate of knee pain in long-distance hikers and could present an opportunity for injury prevention training in the form of muscle strengthening. Because of the way the survey question was worded, we were unable to decipher whether the knee pain was due to acute injury, overuse injury, or exacerbation of a chronic condition, such as pre-existing osteoarthritis. Future work should delineate the causes of the reported knee pain to help determine possible prevention strategies.
When participants reported specific MSK injuries rather than generic joint pain, overuse MSK complaints represented the largest category, with 28% (n=363) of participants reporting medial tibial stress syndrome, Achilles tendonitis, iliotibial band syndrome, or stress fractures. Overuse MSK injuries result from repetitive microtraumas resulting in breakdown in tendons and bone. 9 During tendon healing, fatigued tendons under repetitive stress lose the ability to repair, resulting in weakened collagen cross-linking and disruption of tendon vasculature. 10 Similarly, if microdamage accumulates faster than bone remodeling can occur, bone stress and eventual fracture results. Both intrinsic and extrinsic factors have been linked to MSK overuse injuries. Intrinsic factors include muscle weakness, malalignments, and inflexibility. 9 Extrinsic factors include “training errors” such as large changes in activity duration or frequency.9,11 Walking more than 32 km (20 mi) per week has also been found to be a strong predictor of MSK overuse injuries, placing long-distance hikers at risk. 12 Acute injuries were less commonly reported than overuse injuries, with 18% (n=238) of respondents noting ankle sprains, muscle tears, or a traumatic fracture. These results suggest overuse MSK injuries of the lower extremity may be an appropriate target for injury prevention programs and could include muscle strengthening, flexibility training, and graduated activity development.
Previous studies did not find a correlation between prehike conditioning and injury rates in long-distance hikers, which contradicts our results.5,13,14 This difference may be a result of construct definition. For example, in 1 study, prehike conditioning was defined as performing hard physical activity for 4 h·wk-1. 13 Defining this construct differently in terms of hours of training or types of training may yield different results. Our survey asked participants about previous hiking distances and cross-training history. We chose these definitions because building stamina and using multimodal approaches to fitness are linked to MSK injury prevention in other recreational activities. Few of our respondents had hiked over 805 km (>500 mi) in 1 trip before this attempt, and less than one-third had added strength, stretch, or endurance into their training regimen. Each of these types of prehike training was associated with lower MSK injury, suggesting that further research needs to explore both how to define prehike conditioning as well as how different prehike training regimens affect MSK injuries. Although we were unable to assess optimal prehike training regimens, we were able to find a correlation between prehike training and reduced MSK injury.
Recovery days may also be useful to prevent or lessen the impact of overuse MSK injuries such as tendinopathies and bone-stress reactions. Once acquired, excessive loading and insufficient recovery can lead to a failed healing response in these injuries. Currently, there is no clear consensus in the literature on the optimal quantity or frequency of recovery days in long-distance hiking or their ability to prevent overuse injuries in hikers. However, relative rest is a treatment strategy and therefore an important concept in MSK injury prevention and treatment programs. 9 We attempted to assess how long-distance hikers use recovery days. However, we had a high item nonresponse rate (58%, n=755) to the question about zero days, making it difficult to assess their use in our study population. It is possible the terminology “zero days” was not as widely accepted as believed at the start of the study, and therefore the question will need to be reassessed before future surveys.
Specialized gear may play a role in injury prevention. Studies on the effectiveness of footwear choice to decrease MSK injuries among long-distance hikers have been inconclusive, but use of hiking boots or trail shoes correlated with lower MSK injury when compared to participants who did not report using either of these shoe types (ie, those who reported wearing sandals) in our study. 7 Trekking poles have been shown to improve balance while carrying a load and to reduce muscle activity around the lower extremity joint on downhill grades.15,16 They were widely carried by the respondents and were associated with lower MSK injury in our study, which agrees with previously reported results. Previous studies did not address joint braces for stability. About 27% of our study population carried a knee or ankle brace, suggesting the possibility of pre-existing medical conditions in the joints. We had not anticipated that possibility. An additional survey question will need to be added to future studies to help decipher pre-existing conditions when long-distance hikers are surveyed for this purpose. We will also need to expand the medical conditions lists to include such MSK complaints as osteoarthritis because it may have accounted for otherwise unspecified joint pain found in this population.
Less than 25% of participants sought medical treatment within 7 d of an injury. It is unclear whether the injuries were not substantial enough to warrant treatment, whether medical care was not available, or whether the hikers chose not to seek treatment despite the level of injury. However, 8% of those injured on the trail reported that the injury had not healed at the time of the survey, suggesting some injuries occurring on the trail result in MSK complaints that transition to chronic in definition.
Limitations
This study has several limitations. Only using long-distance hikers who registered with the ATC may have introduced selection bias. For example, more experienced hikers who were not interested in being recognized or less experienced hikers who were not aware of the registration process may have been excluded. The limited response rate (52%) may have created bias because those who responded may not adequately reflect the target population.
Another limitation is the use of self-reported injuries. Although diagnosis by a medical provider may have provided information that is more accurate, the hikers determined that not all of the injuries required medical attention or they chose not to seek care. Relying on hikers to self-report injuries provided insight into their MSK injuries, but it created the potential for inaccurate reporting. Recall bias may have also influenced results because participants were given the questionnaire at the end of the hiking season.
In addition, the questions in the survey were untested. They may not have collected the information as intended or they may have introduced surrogate information bias (forcing respondents to choose from a list of options). By adding “other, please specify,” we attempted to decrease this bias and give participants an opportunity to generate their own answers. Item nonresponse was an issue and may have led to biased estimates. It may have partly been a result of question design, such as in the example of using the terminology “zero days”, which may not have been as widely used by hikers as believed during study design. Unmeasured confounding may have also influenced results, including creating a barrier to determine how basic demographics such as age, sex, and body mass index influenced outcomes. We were unable to establish optimal descriptive statistics and correlations across data owing to limited, untested questions and lack of demographic information.
Conclusions
Among multiple MSK injuries reported, overuse/chronic injuries were reported more frequently than acute MSK injuries in long-distance hikers who responded to this survey. Although prehike training strategies, utilization of stabilization gear, and use of recovery days varied among respondents, those who reported that they did not train before the hike were more likely to have an MSK injury, whereas those who used stabilizing footwear and aids were less likely to do so. Further research is needed to understand whether prehike conditioning and on-trail strategies can decrease MSK injuries in the AT long-distance hiking population.
Footnotes
Acknowledgements
Acknowledgments: We thank the Appalachian Trail Conservancy for their collaboration.
Author Contributions: Study concept and design (MK, AC); data acquisition and analysis (MK, AC); drafting, critical revision, and approval of the final manuscript (MK, AC).
Financial/Material Support: None.
Disclosures: None.