
Abstract
Telemedicine potentially offers enormous value to expeditions to remote environments. For healthcare professionals, telemedicine can provide access to specialist advice. Where no healthcare professionals are present, telemedicine may be the sole source of expert care.
This systematic review appraises and summarizes the current literature regarding telemedicine in patient management on expeditions to remote locations and identifies areas for future research. MEDLINE and EMBASE were systematically searched for relevant articles from 1980 through February 2018. Data were handled according to the PRISMA process and analyzed using type-specific critical appraisal checklists where possible. Two hundred twenty-five articles were identified, 33 of which were included in this systematic review. They encompassed a variety of remote environments, including maritime (13), polar (9), mountainous (5), jungle (1), and multiple austere environments (6). Although some environments were better reported than others, many overarching concepts were generalizable. Through channels of communication that included telephone, radio, videoconferencing, and email, telemedicine has been used effectively in a range of environments to initiate treatment, follow up with patients, and determine the appropriateness of evacuation. Telementoring, in which a remote expert guides a local care provider in performing a procedure or task, is a promising aspect of telemedicine that is currently being developed. As technology advances, the scope of telemedicine will continue to expand. However, each new telemedical development must be shown to do more than simply function in a remote environment. Instead, new technologies should be tested for improved patient, practitioner, or expedition outcomes, within a telemedical system.
Introduction
Telemedicine is the provision of healthcare to patients by a distant provider. 1 It allows direct patient management without the physical presence of the healthcare professional and enables isolated healthcare providers to access specialist advice. 2 As the popularity of adventure tourism and expeditions to remote environments grows, 3 telemedicine may become increasingly prevalent.
From the oceans to the Antarctic, expeditions are undertaken for different purposes in varied settings. 3 Each location presents different challenges. At sea, ships can be away for long periods of time. Medical facilities are limited, and there may be no medical personnel onboard. 4 Evacuation or redirection to healthcare may be possible, but it would often be disruptive and expensive. In contrast, research stations in the Antarctic may have good medical facilities, but evacuation during the winter months is nearly impossible. 5
This review summarizes the current literature regarding the use of telemedicine to assist in management of patients on expeditions in remote and austere terrestrial locations and identifies areas for future work.
Methods
Search Strategy
Embase and Medline were systematically searched via Healthcare Databases Advanced Search through February 2018 using the search strings in Table 1. Reference lists of full-text publications were hand-sorted to locate other potentially relevant publications. Titles and abstracts were screened for eligibility, and full texts of all articles that appeared relevant were obtained. These were checked against the inclusion and exclusion criteria to generate the final list of publications for review.
Search terms
Inclusion Criteria
All reviews, studies, and commentaries published in peer-reviewed journals concerning telemedicine and its contribution to diagnosis or patient management in remote or austere environments, such as maritime, polar, mountainous, jungle, or desert environments were included. We used a broad definition of “expedition” that included seafarers, cruise ship passengers, visiting researchers, and military personnel.
Exclusion Criteria
This review focused specifically on telemedicine for patients on remote terrestrial expeditions, rather than telemedicine in general. Consequently, articles that mainly focused on telemedicine for disaster medicine, battlefield medicine, aerospace medicine, rural medicine, and chronic disease management in settled populations in remote areas were excluded. Conference abstracts, unobtainable full-text articles, and articles not published in English or published before 1980 were also excluded. Because telemedicine’s performance is technology-dependent, articles published before 1980 were considered outdated.
Methods for Critical Appraisal
Study type-specific critical appraisal tools were used to review the articles where possible. These included a checklist for critical appraisal of case reports, 6 the Joanna Briggs Institute checklists for case series, 7 and the critical appraisal skills program qualitative checklist. 8 These checklists offered a systematic framework to critically appraise the varied sources of evidence.
Results
Thirty-four publications were included (Figure 1). Many were of low evidential quality, consisting of case series and reports, pilot studies, and company reports on activities of telemedical programs. Qualitative studies, retrospective studies evaluating existing services for telemedicine, and 1 research proposal were also included. No systematic reviews or randomized control trials regarding the use of telemedicine in remote environments were identified.
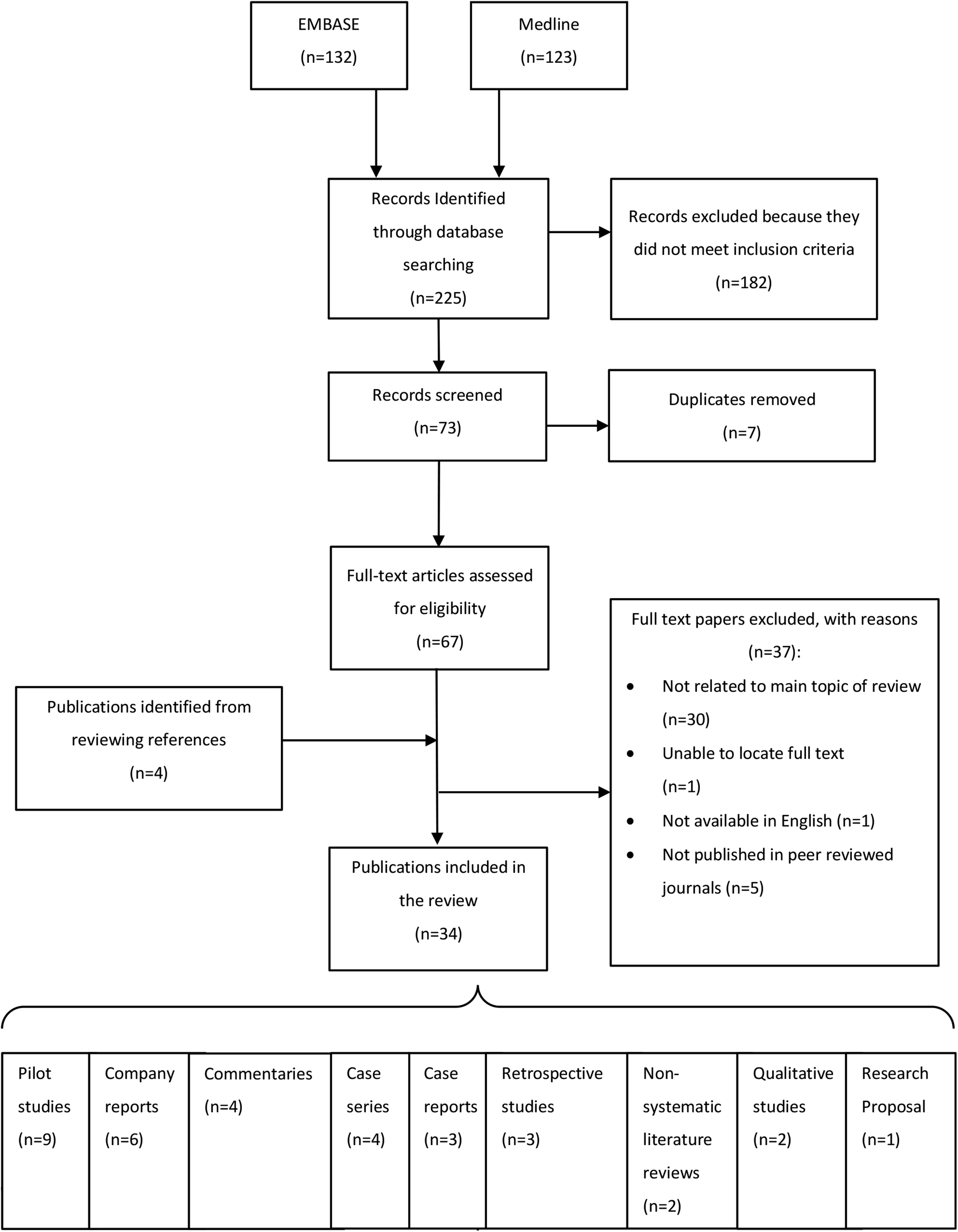
PRIMSA flow diagram.
The articles included dated from 1995 to 2017. The maritime and Antarctic environments were best represented. No reports focusing solely on desert or Arctic conditions were identified. Table 2 breaks the results down by environment and article type.
Publications by article type and environment
Subjects included general use of telemedicine for consultation purposes; use of diagnostic aids such as ultrasound, electrocardiography (ECG), and photography; telementoring; feasibility of equipment operation in austere environments; user satisfaction with telemedical services; and development of telemonitoring equipment (Table 3). 9 -38
Publications categorized by topic a
Some publications may appear in more than one category.
The number of patients involved in each article varied according to publication type because many studies involving patients were case reports or case series. Four studies5,20-22 included specific cohorts of patients treated within a particular timeframe. One maritime 23 and 1 Antarctic 5 report provided data on the number of telemedical consultations undertaken and the incidence of each type of presenting complaint. Of 10,815 patients treated by the Italian telemedical maritime assistance service (TMAS) from 2012 to 2014, abdominal complaints and injuries were the most frequent cause of telemedical consultations, contributing to 17%, respectively. 23 Data from Japan’s Syowa station in the Antarctic found that 45% of 4932 telemedical consultations from 1956 to 2003 were for injury and trauma. 5 This type of data could be used to plan equipment provision and recruitment of specialists.
The articles included in this review also illustrated the range of medical equipment and services that have been used in remote environments, in particular the polar and maritime settings. All bases in the Antarctic had standard medical equipment, with larger stations having more advanced facilities such as plain radiography (x-ray) and ultrasound. 25 The largest US research stations had a dermatology telemedical program and specialized equipment (eg, a dermatoscope), as well as facilities to perform biopsies and basic staining. 26 Japan’s Syowa station had operating facilities, wherein 2 appendectomies under spinal anesthesia had been performed.5,39 ECGs were available on many ships and have been advocated internationally. French merchant or fishing ships navigating without limitation of destination or time and all passenger vessels have been mandated to carry an ECG machine and defibrillator (which can be used by a nurse or second captain). 20 Cameras, readily available in many environments, have been used to aid diagnoses. The transmission of photos via email has been particularly well reported at sea by the Italian TMAS and in the Antarctic environment by an Antarctic dermatology program.23,26 In addition, 2 case series9,10 and 1 case report 12 illustrated the use of photos to assist in the diagnosis and management of skin conditions and minor trauma and to transmit ECGs in the maritime environment. Cases included remote follow-up of a burn injury of a patient at sea and a diagnosis of toxic epidermal necrolysis that lead to a patient’s aeromedical evacuation.
Discussion
Defining “expedition” was a key factor in determining which articles were included or excluded from this review. Although an expedition has been described as “a journey with a purpose,” 3 that definition might also have included a trip to the grocery store. Therefore, the nature of the journey must be further clarified by the austerity or remoteness of its environment. However, even within the same geographical setting, “remoteness” is as much a question of facilities as linear distance from help. For example, a fishing vessel sailing in the same waters as a cruise ship might be considered more “remote,” given the fishing vessel’s relative paucity of medical equipment and experience. The same might be said of Antarctic bases, which varied in their facilities depending on the size of the base and the population it served.
A working definition might therefore be a journey with a purpose, but also one over a set timeframe, with limited medical provision and barriers to rapidly transferring a patient to definitive care. This formed the basis of the review. It was believed that cruise ship medicine met this definition; although rural, aviation, space, and disaster medicine all shared some of its scope, they were excluded. Rural populations and those affected by natural disasters involved settled populations rather than those making a journey and so were on an “infinite” timeframe. Medical decision-making in terrestrial aviation revolved primarily around whether an aircraft should be diverted to land and, as such, operated on a much shorter timescale and with different constraints compared with most expeditions. In space medicine, telemedical research has typically been directed toward exploratory class missions to the moon and Mars. Consequently, the challenges considered were different from those on Earth (eg, microgravity, communication delays of up to 15 min, and the length and evacuation costs of the missions themselves). This led to a presumption of better technology and skills on the part of systems and operators in the space medicine literature, in comparison to work from terrestrial expeditions.
Channels of Communication and the Rise of Videoconferencing
Telemedicine is possible as long as there is communication, be it by fax, email, telephone, radio, or videoconferencing. Although verbal communication may have been at the heart of telemedicine, images and other media have assisted consultations. This has been possible for over 20 y in even the most remote parts of the world, as demonstrated by a pilot study published in 1997 in which ECG tracings, audio clips, videos, and still images of healthy participants were transmitted successfully during an expedition on Mount Logan. 30 With technological advances, videoconferencing for real-time telemedical consultations has become available in remote locations including at sea, 11 in the Antarctic, 5 in the mountains, 14 and in the jungle. 33 Routine videoconference teleconsultations were conducted monthly at Japan’s Syowa Antarctic station. 5 Even before 1999, videoconferencing was used for daily ward rounds at Everest Base Camp 14 and while accompanying Martin Strel on his swim of the length of the Amazon river (129 real-time consultations were undertaken during the journey). 33 Videoconferencing has allowed remote doctors to speak directly to both patients and local care providers, observe examinations, and guide care providers through simple procedures and examinations. 5 Its advantages over voice communication were demonstrated in a case report of a mariner expressing suicidal thoughts at sea. Unlike voice calls alone, videoconferencing allowed the psychiatrist to perform a full psychiatric assessment including assessment of appearance and behavior as part of mental state examination. Mania was diagnosed, and psychiatric hospitalization abroad could be avoided because the patient was deemed safe to fly. 11
Prevention of Unnecessary Evacuation
As well as facilitating diagnosis and management of patients, telemedicine has been effective at preventing unnecessary evacuations (eg, when used to diagnose and treat pericarditis in a worker in the Antarctic 2 and to manage an episode of supraventricular tachycardia in a passenger on a cruise ship). 10 Its effectiveness was also demonstrated by a retrospective study in the Antarctic Amundsen-Scott and McMurdo research stations, where telemedicine combined with ultrasound was used to prevent 17 unnecessary evacuations out of 66 cases between 2002 and 2003. 21 A retrospective study over 32 mo between 2009 and 2012 on an orthopedic teleconsultation program for the US military found that of 597 referrals, 26 evacuations were prevented. 22 Although this may not be generalizable to the civilian population on expedition, given that the military has extensive access to medical facilities and personnel, it offered a good example of how specialist opinions via telemedicine could prevent unnecessary evacuations.
ECGs
The provision of ECG equipment on ships has been subject to debate, so the topic has been studied in more depth than in other environments. Those questioning the value of ECGs on ships believed them to be too difficult to perform accurately, risking false positives or negatives. 4 However, studies have also illustrated their value, with case reports 10 outlining scenarios in which ECGs facilitated decisions regarding initiation of treatment and evacuation. One example was the case of a passenger on a cruise with a supraventricular tachycardia of 220 beats·min-1, diagnosed remotely as Bouveret’s disease junctional tachycardia by a cardiologist based on the ECG. Evacuation was avoided on the cardiologist’s recommendation, and the patient was treated with amiodarone and outpatient follow-up on return. 10 In a retrospective study on the use of ECGs on ships, 20 of 179 cardiac presenting complaints identified in 2008 and 2009, ECG enabled diagnosis of 23 ST elevation myocardial infarctions, 21 non-ST elevation myocardial infarctions, and 15 arrhythmias. However, the same study also found that although 74% of vessels were equipped with an ECG machine, a small proportion (4 of 63) of ECGs could not be transmitted owing to either lack of equipment or transmission problems. 20 Another study found that 23% of users (n=30) had difficulties in recording ECGs and 17% (n=22) had difficulty with transmission. 18 However, the value of ECG on ships appeared to outweigh its difficulties, and its ability to assist decision-making has been clearly demonstrated. Furthermore, although not every vessel may have had an ECG machine, it has still been beneficial for some ships to have been equipped to aid others. This was demonstrated in a case report in which the French TMAS directed a fishing vessel without ECG equipment to change course to another, better equipped ship after a fisherman onboard developed chest pain. 10 Extensive anterior myocardial infarction was diagnosed and treated appropriately.10,20
Radiology
Remote imaging has been a valuable diagnostic tool, particularly in the management of trauma. The contribution of radiography and telemedicine to patient care in the Antarctic was demonstrated in a case series from 1995 where they were used to diagnose and manage a Colles fracture and a dislocated hip without evacuation. 13 Because injury and trauma contribute to almost half of the medical consultations in the Antarctic, 5 x-ray facilities have been particularly useful to Antarctic stations in reducing the burden of evacuations. A low-quality commentary from 2002 suggested introducing radiology facilities on cruise ships. 15 Since then, x-ray has become commonly available on cruise ships and is now recommended in the American College of Emergency Physicians’ 2014 healthcare guidelines for cruise ship medical facilities. 40
For those remote environments without access to x-ray facilities, portable ultrasound has been a developing tool for diagnosis. Two nonsystematic reviews36,37 published by the same author on the use of point-of-care ultrasound summarized the literature regarding the use of portable ultrasound in prehospital and austere environments. Fifteen of the included studies demonstrated the accuracy of portable ultrasound for diagnosing hemoperitoneum, pneumothorax, pericardial effusion, and abdominal aortic aneurysm in emergency department patients. 37 One study that assessed the use of prehospital ultrasound in patients with blunt abdominal trauma found that management was changed in 30% (n=30) of patients. 41 Eight studies were reported in which point-of-care ultrasound was used in austere environments including the Amazon jungle, the International Space Station, the Artic, and after a hurricane in a village of a developing country. The challenges of ultrasound examination in these environments were uncooperative patients, inadequate lighting, limited power supplies, lack of physical space, and time constraints. Despite these limitations, portable ultrasound remains a promising avenue for prehospital and remote environments owing to its portability, potential smartphone compatibility, and ability for remote interpretation of scans. 37
In the Antarctic, a case report 2 and a retrospective study 21 have been published on the use of ultrasound for telemedicine at McMurdo and Amundsen-Scott research stations. Both reported the use of store-and-forward interpretation (wherein images were transferred via email to be interpreted after completion of the examination) and real-time interpretation (where the remote doctor visualized the examination while it was in progress). Store-and-forward was adequate in the majority of cases, and real-time assessments were arranged when necessary. In 51 of 62 store-and-forward scans, ultrasound contributed positively to patient management, leading to initiation, confirmation, or prevention of treatment and establishing need for further investigations, second opinion, or evacuation. In fact, evacuation was prevented in 26% of cases. However, 2 scans did not provide enough diagnostic information and 7 gave false positives or negatives. This study illustrated the usefulness of ultrasound for patient management but also its dependence on operator skill; examinations performed by physicians with basic ultrasound training had the potential to generate more misleading scans than those performed by a skilled sonographer. 21
Remote Telementored Ultrasound
Ultrasound is operator dependent. It takes several years to train a sonographer, and the Royal College of Radiologists recommends that clinicians who perform focused assessments with sonography for trauma scans should first have undertaken at least 50 examinations under supervision. For clinicians to become competent at ultrasound examinations of other systems, even more repetitions may be required. 42 Where a local care provider on an expedition may not be competent at performing an ultrasound, the possibility of using telementoring, where the local ultrasound operator is guided by a remote expert, has been explored. Remote telementored ultrasound (RTUS) has been used successfully in the Antarctic, when a physician with basic ultrasound training was guided by a cardiology team in Texas via video-teleconferencing to obtain optimal images for echocardiography. This allowed the diagnosis of pericarditis to be confirmed and its progression assessed. The effusion was shown to be resolving, which avoided evacuation and allowed the patient to be managed medically in the Antarctic. 2 RTUS was also described in a case report published in 1999 at Mount Everest Base Camp where videoconferencing facilitated an ultrasound chest examination that demonstrated consolidation in the patient’s left lung. 14 Since then, RTUS has been shown to be able to provide high-quality images of multiple organ systems. 43
Three pilot studies29,31,35 explored the use of RTUS in remote environments using specifically designed equipment that included a portable ultrasound and a head-mounted web camera that allowed the remote expert to visualize the examiner’s hands, the patient, and ultrasound images for 1-way video and 2-way audio communication. A variety of operators, locations, and ultrasound examinations were tested. Two climbers with no ultrasound experience were guided remotely to perform lung ultrasounds in an expedition medical tent at Mount Everest’s advanced base camp on 2 patients who were acclimatizing. As well as real-time audio guidance, the climbers were given cue cards for visual guidance on probe position and were able to perform the examination without difficulty. The images were suitable for excluding pneumothorax and quantifying the presence of comet tail artifacts, which are a sign of high-altitude pulmonary edema. 31 Another pilot study assessed the feasibility of RTUS in 8 locations, including 2 remote outdoor environments (Banff and Lake Louise). 35 Focused assessments with sonography for trauma scans were performed on healthy volunteers by ultrasound operators with experience varying from medical trainee to nonmedical personnel. The presence of lung sliding to exclude pneumothorax was demonstrated by all users, 35 but the study did not comment on whether views of different structures were adequate to diagnose or exclude other pathology. Although these pilot studies have demonstrated that the technology for RTUS in remote environments is available, further studies are needed to assess its effectiveness at diagnosing different pathologies, as well as what types of expeditions would benefit from investing in RTUS and how much training the local user would require.
The issue of training was explored in a pilot study of ships’ officers being taught to use ultrasound independently for store-and-forward interpretation. Unfortunately, a large proportion of their scans gave false negative results, and some could not be interpreted because the organ in question was not visualized. 27 Although the study was limited because the seafarers only had 30 min of practical teaching, RTUS may be a more effective use of teaching resources; independent sonography skills would deteriorate without regular practice, and false negatives may have adverse effects on patient care.
Telementoring for Damage Control Surgery
The use of telementoring to assist in damage control laparotomies in austere environments for traumatic noncompressible truncal intracavity hemorrhage has been explored. 38 In a pilot study, military medical technicians performed damage control laparotomies on a surgical simulator with the assistance of telementoring via 1-way video and 2-way audio communication. The subjects were split into those who performed the surgery with and without telementoring. The results were not supportive; there was no difference in blood loss between the 2 groups, and none of the candidates could close the laparotomy wound. 34 The report itself was of poor evidential quality because the number of participants was not stated and the methodology was unclear. Questions also remained regarding the provision of anesthesia. Furthermore, damage control surgery is part of a chain of resuscitation, rather than an end in itself. Despite these limitations, the use of telementoring for surgery in remote environments still has potential, although it may be more pertinent for battlefield medicine and space medicine than for the expeditionary focus of this review.
Areas for Further Development
The success of telemedicine depends on multiple factors, including the local equipment and caregiver, the remote physician’s expertise, and, of course, the communication between both parties. A number of maritime studies have suggested improvements that would enhance patient care and which may be extrapolated to other remote environments. First, education of both local care providers and remote physicians should be promoted. A user satisfaction survey on telemedicine found that seafarers were keen for training to be focused on isolated environments, 18 and interviews from caregivers on recommendations for maritime telemedicine suggested that healthcare providers needed more awareness of the working conditions in remote environments. 19 The provision of electronic medical references onboard ships has been proposed, and it has been suggested that the process of contacting telemedicine providers should be simplified because it can be confusing for care providers if there are too many methods to contact help. 19 Equipment for monitoring and telemedical communication should be optimized. 19 Telemedical carts have been developed by the Italian TMAS that included standard monitoring equipment, as well as a glucometer, 12-lead ECG, spirometer, electronic stethoscope, and camera that could be easily linked to a provided computer. 23 Further work will be needed to determine whether this equipment has a quantifiable impact on patient care.
An article published in 2019 by Australian Broadcasting Corporation News highlighted the benefits of training of local care providers, when the sole doctor at an Australian Antarctic base broke a bone in her dominant hand during the winter season. Via telemedicine, a hand surgeon diagnosed the severity of the injury and advised treatment. The hand surgeon and an anesthesiologist were able to remotely guide local surgical lay assistants (nonmedical personnel trained to assist a doctor) via a videolink and x-ray imaging to perform a nerve block, reduce the bone, and apply a plaster cast. Part of this procedure’s success was attributed to the 2 wk of hospital training received by the surgical lay assistants before deployment, along with monthly refresher training by the base doctor. 44 This example illustrated the success of a telemedical system, rather than simply telemedical technology. The combination of planning and regular training with adequate medical and communication facilities and appropriate remote expertise allowed the successful diagnosis and treatment of the patient.
Telemetry (real-time patient monitoring) and telementoring (remote guidance of a less-experienced care provider by an expert) both have potential to contribute to the safety and success of expeditions. Wearable telemetry with a global positioning system for routine monitoring has been developed and made commercially available,32,45 although its impact on patient and expedition outcomes has not yet been fully assessed. Another application, yet to be tested, is the use of real-time monitoring to provide anesthetic support in the Antarctic to assist local doctors performing invasive procedures. 24 For telementoring, seafarers have enthusiastically suggested the development of videoconferencing on ships to guide nonmedics in performing medical procedures 9 such as joint relocation and suturing. 17 However, advocating the approach would require further research into its feasibility, effectiveness, and potential for harm (along with its associated medicolegal ramifications).
In the future, drones may be employed as a link in a telemedicine system because they are able to access remote locations promptly. Drones have been used for surveillance in the initial assessment of disasters, along with transport of equipment such as automated external defibrillators, lab specimens, and blood products. 46 -48 However, the role of drones in telemedicine remains largely unproven. One study demonstrated the feasibility of using a drone to assist in telemedicine by providing a wireless communication network between a surgeon and a robot to perform telesurgery when the operator was located remotely from the site of the patient. 49 Another article from the gray literature describes a drone with videoconferencing capabilities and the capacity to deliver medical equipment, designed to provide telemedical assistance. 48 Drone technology has been improving rapidly, but, like other promising new avenues of telemedicine, its role within a telemedical system requires exploration and evaluation.
Limitations
Many of the articles included in this review were small studies in specific environments. Although some environments were better reported than others, some concepts were generalizable. For example, telepsychiatry by videoconferencing may only have been documented in the maritime environment, but it is likely to be possible in any location with access to videoconferencing.
Although the inclusion and exclusion criteria have been clearly stated, the definition of an “expedition” will always be somewhat subjective. The broad definition of “remote and austere environments” maximized the likelihood of relevant studies being located. Only articles available in the English language were included. As telemedical services have been provided and used by a multitude of nations, restricting the search to a single language limited the potential for articles to be identified. Additionally, because technology has been the key driver in telemedicine, the earliest acceptable date of publication of included articles was a matter of debate. For example, 4 of the Antarctic reports1,13,24,25 included were written before the introduction of INTELSAT in 2004, which greatly improved satellite bandwidth and enabled videoconferencing. INTELSAT also no longer restricted communications to certain times of day (unlike the previous satellite, INMARSAT). 5
Conclusions
Telemedicine on expeditions can be used to initiate treatment, follow up with patients remotely, and decide on the necessity of evacuation. Indeed, telemedicine’s role in the prevention of unnecessary evacuation was a consistent thread running through the publications in this review. With ever-improving satellite communications, telemedicine is available anywhere in the world. Once restricted to voice communication alone, increasing data bandwidth has expanded the scope of telemedicine to include images, videos, and diagnostic information from point-of-care testing such as ultrasound. Videoconferencing has been used successfully in the most remote of locations for patient assessment, as well as facilitating telementoring.
Although telemedicine has already assisted many people in remote locations, it is important to continue developing this field and critically appraising its success to ensure that delivery of healthcare in these environments is of the highest standard possible. New technologies must be shown to do more than simply function in a remote environment. They should demonstrate improved patient, practitioner, or expedition outcomes within a telemedical system that includes training, equipment provision, and follow-up care.
Footnotes
Acknowledgements
Author Contributions: Study concept and design (LT); acquisition and analysis of the publications (LT); drafting of the manuscript (LT); critical revision of the manuscript (MW); and approval of final manuscript (LT, MW).
Financial/Material Support: None.
Disclosures: None.