
Abstract

To the Editor:
Hump-nosed vipers of the genus Hypnale are venomous pit vipers endemic to Sri Lanka and southwestern India. They are the most common cause of venomous snakebites in Sri Lanka, causing 27 to 77% of all snakebites. 1 Usually, their bites cause local envenoming only. 2 Less frequently, bites can cause significant morbidities, such as acute kidney injury, chronic kidney disease, 3 venom-induced consumption coagulopathy, 4 chronic wounds, and amputations of digits. 2 Death after hump-nosed viper bites is very rare, and the mortality rate is about 0.9 to 1%.2,5 When death does occur, it is usually in the days after the bite. To our knowledge, sudden death has not been previously reported after a hump-nosed viper bite. We report a fatal case of proven H hypnale bite in which the victim died approximately 45 min after the bite.
A 60-y-old male, diabetic estate worker was bitten by a hump-nosed viper while he was working on property situated about 5 km away from his house. He lived in Nivithigala, a remote village in the Ratnapura district, and had gone to the estate in his own 3-wheeled vehicle at around 1000. The snakebite occurred on the left dorsum of his foot at around 1030. He killed the snake, came back home by his vehicle at around 1045, told the story to his wife, and identified the snake as a Polon thelissa (the Sinhala name for hump-nosed pit viper). He and his wife planned to go to a nearby local hospital situated about 8 km from their house. At that time, he had mild pain at the site of bite and few drops of bleeding. While he was changing his shirt, he collapsed and noted pain in his left arm. He was carried to the local hospital at about 1115. He did not speak on the way to the hospital, and upon arrival, he was declared dead by the admitting medical officer. The snake, which was brought to the local hospital, was identified as a hump-nosed viper by the admitting medical officer. The man’s body was transferred to Teaching Hospital Ratnapura for postmortem examination, along with the offending snake. According to the standard key, 6 the snake was identified as H hypnale (Figure 1) by the corresponding author. Autopsy examination showed pulmonary and myocardial hemorrhage. Kidneys, liver, brain, and coronary vessels were macroscopically normal. Acute renal tubular necrosis, acute ischemic damage to the brain, and pulmonary hemorrhage were observed on microscopic examination (Figure 2).

A hump-nosed pit viper (Hypnale hypnale), the snake responsible for the bite (only a portion of the snake was available). Thick black arrow indicates the loreal pit (characteristic feature of pit vipers), and thin black arrows indicate 5 large head scales (one of the features that differentiates hump-nosed vipers from Sri Lankan green pit vipers).
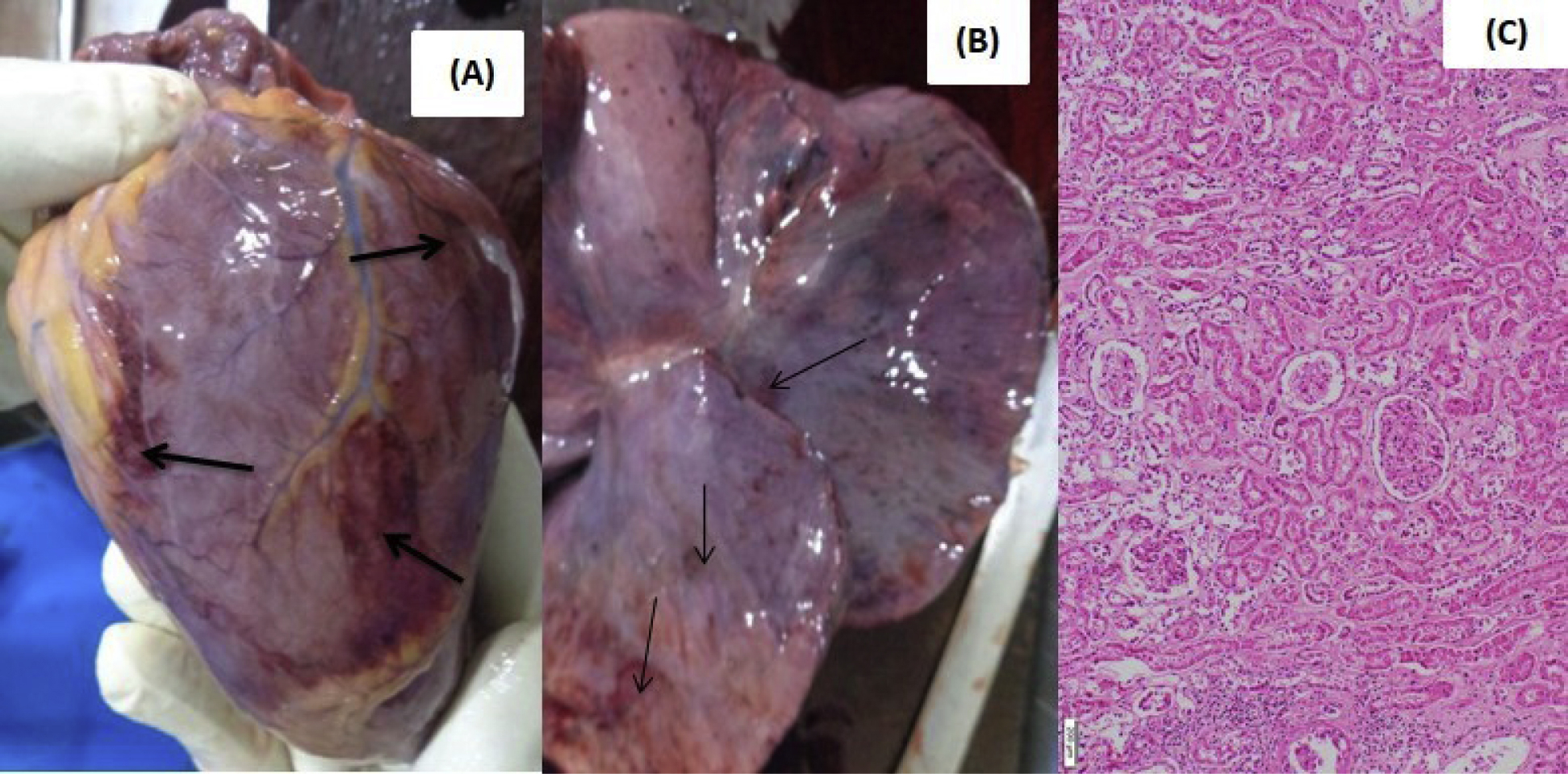
Postmortem findings. A, Myocardial hemorrhages (indicated with arrows). B, Pulmonary hemorrhages (indicated with arrows). C, Histologic appearance of acute renal tubular necrosis at ×40.
Out of 3 species of genus Hypnale, deaths have been previously reported following envenoming by H hypnale7,8 and H zara. 9 However, no deaths have been reported so far regarding H nepa envenomation. This is because its bites are very rare. Hypnale envenoming involving more than 1 system is more likely to be fatal. 7 -10 In our patient, although he was diabetic, a detailed medical history confirmed that he had good diabetic control with regular treatments and no microvascular or macrovascular complications. Because the patient was dead on admission to the local hospital, resuscitation with cardiac massage was not attempted. Circumstantial evidence suggests that our patient’s death was due to the effects of Hypnale venom. On postmortem examination, there were myocardial and pulmonary hemorrhages suggestive of myocardial dysfunction causing arrhythmia as the cause of rapid death. It is possible that sudden death after snake envenoming may occur due to direct intravenous bite with rapid flow of venom to the heart. In our patient, however there were no such fang punctures.
Currently, there is no antivenom for hump-nosed viper envenoming in Sri Lanka, and patients are managed symptomatically. Hypnale venom is procoagulant and contains thrombin-like enzymes that cause venom-induced consumption coagulopathy and bleeding. This may cause fatal complications such as intracranial and pulmonary hemorrhage. 7 Pericardial and endocardial hemorrhage has previously been observed in fatal cases of H hypnale bites. 4 In addition, cardiac complications such as cardiac arrest, atrial fibrillation, and ischemic changes on electrocardiogram may cause deaths in H hypnale envenoming. 8 Snake venom may also cause coronary vasospasm, thus causing ischemia to the myocardium. 11 In addition, cardiac output may be reduced owing to myocardial necrosis caused by snake venom. 12 The other causes of cardiac arrest after snakebite may be hyperkalemia due to acute kidney injury, vascular collapse, and hypovolemic shock due to bleeding. Myocardial damage may also occur due to disruption of myocardial cell membranes and myofibrils. To date, the shortest reported duration for death after a hump-nosed viper bite is 6 h from admission to the medical facility, 13 although this may be more than 6 h considering the time since the bite. According to the literature, death due to hump-nosed viper bite may occur anywhere between 6 h and 16 d. 7 -9,13 Our patient, however, died before coming to the hospital 45 min after the snakebite. Even if an effective antivenom was available in acute care hospitals, fatality may still occur rapidly after envenomation by hump-nosed pit viper, as highlighted by the case presented.