
Abstract
The objective of this review is to provide recommendations on the evaluation and management of urologic conditions in a resource-poor or austere setting from the perspective of the urological literature. The material was synthesized predominantly from urologic society guidelines and journals to bring additional urology-focused insight to the topic to complement the currently available literature, which is largely based on recommendations from nonurologic specialties. We sought to provide a reference guide from a urology-based framework that encourages a collaborative multidisciplinary approach to the development of a resource that serves those in a wilderness, austere, or resource-poor setting.
Introduction
An increasing number of people are engaging in outdoor recreational activities across the United States. In 2017, the US National Park Service registered over 330 million recreational visits, up from 275 million just 10 y prior. Both the Appalachian Trail Conservancy and the Pacific Crest Trail Association have recorded a steady rise in the number of people hiking the entire trail each year. With an increase in outdoor recreation, a greater number of people are exposed to environments where medical services are not immediately available. A review of US National Park Service emergency medical service responses from 2012 to 2013 found that there were approximately 40 calls requesting medical assistance per million visitors. 1 Emergency department visits for urologic conditions exceed 2.4 million visits per year. 2 Extrapolating from this burden on emergency departments, one may recognize the potential for the development of urgent urologic conditions in the wilderness.
Despite the prevalence of urgent or emergent urologic conditions in the US population, as well as the increase in participation in wilderness activities, little urology-focused information is available regarding evaluation and management in a remote setting. One manner in which other specialties have addressed this problem is through telemedicine. Indeed, the American Urologic Association (AUA) has released a white paper on telemedicine in urology; however, it focused more on nonemergent situations and environments with readily available internet or network capabilities that allow for formal consultations with urologists. 3 The telemedicine approach is admirable and undoubtedly deserves resources for further development and investigation; however, it fails to provide assistance and education to non-urology-trained medical providers who may be working in conditions that require more acute management or where network connections are unavailable. To address this issue, we present a review of common urgent and emergent urologic conditions that may be encountered in settings without readily available urologic expertise.
Methods
Common urologic conditions were identified through a review of both the AUA curriculum on urologic emergencies 4 and literature within the field of wilderness and environmental medicine, such as Auerbach’s Wilderness Medicine text. 5 A review of the literature was performed with a primary focus on the AUA practice guidelines and AUA university core curriculum and a PubMed search for investigations performed by the urologic community. For each of these common urologic conditions, we describe patient presentation, evaluation, management, and indications for evacuation to a hospital or higher level of medical care. Recommendations target an audience of those trained in basic medical care, as well as emergency medical service personnel responding to those in rural, wilderness, or other resource-poor environments.
Brief Overview of Relevant Anatomy
The genitourinary system is an intricate network of anatomic and physiologic components that help to manage human metabolism, toxin excretion, volume status, hormone homeostasis, and sexual and reproductive function. Anatomically, the system is composed of 2 kidneys, their corresponding ureters and adrenal glands, the bladder, and the urethra (Figure 1). In males, we additionally consider the prostate, scrotum, 2 testes, and their associated structures.
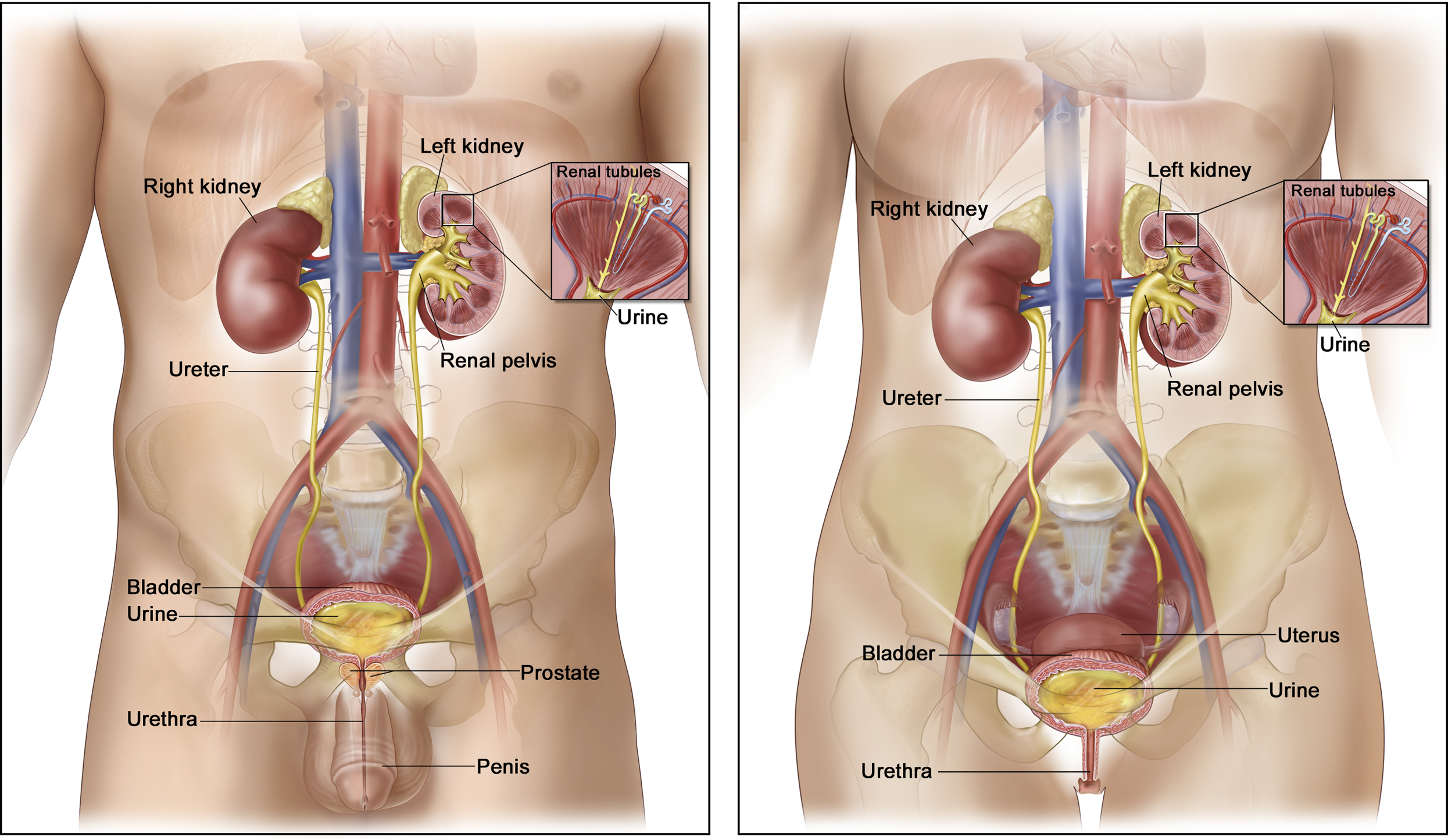
Genitourinary anatomy. For the National Cancer Institute © 2010 Terese Winslow LLC, US Government has certain rights. Reprinted with permission.
The kidneys are paired organs in the posterior abdominal cavity, surrounded by a fascial layer (Gerota’s fascia) within the retroperitoneum. The adrenal glands, small paired organs superior to the kidney, lie within Gerota’s fascia. The renal blood supply comes from the renal arteries, which emanate from the abdominal aorta. Each kidney drains into its associated ureter to transport urine from the kidney to the bladder. 6 The bladder is a hollow pelvic organ that acts as a reservoir for urine drained by the kidneys and assists in emptying urine through a set of coordinated neuromuscular processes. Finally, urine passes from the bladder through the urethra. In males, the urethra initially passes through the prostate gland before entering the penis. The female urethra exits anterior to the vaginal introitus.
Unique to the male genitourinary system is the scrotum, containing paired testes and their associated structures, such as the vas deferens and spermatic cord. 7 The testes produce sperm, which drain into the attached epididymis and subsequently into the bilateral vas deferens for transport to the ejaculatory ducts in the prostatic urethra.
First responders must be aware of potential urologic injuries based on the mechanism of action of the injury and its relation to relevant anatomy. By having a low index of suspicion in the case of rib fractures, pelvic crush injuries, or straddle injuries, one may have a low threshold to suspect kidney, bladder, or urethral injury, respectively. This knowledge extends beyond just traumatic conditions; therefore, we have included anatomic landmarks and physical examination as a critical component of each urologic condition discussed.
Urgent/Emergent Urologic Conditions
Acute Urinary Retention
Acute urinary retention is the inability to empty the bladder and may become a true urologic emergency. Untreated urinary retention can ultimately lead to kidney failure, severe infection, pain, and, in extreme circumstances, bladder rupture. Urinary retention is 13 times more likely to occur in men than in women owing to obstruction from the prostate, and incidence increases with age. 8 Retention can also be seen secondary to black widow spider envenomation 9 or trauma that causes pelvic fracture or spinal cord injury. In addition, certain medications commonly used while traveling may predispose individuals to acute urinary retention (eg, antihistamines, over-the-counter cold medicines). 10
Presentation
Sudden inability to urinate accompanied by suprapubic pain and lower abdominal discomfort. People with urinary retention are often in a significant amount of distress. Less acute presentations may include urinary dribbling or overflow incontinence.
Evaluation
History should focus on recent trauma, prior episodes of urinary retention, history of genitourinary surgery, recent hematuria or passage of blood clots in the urine, and urinary symptoms. Physical examination demonstrates suprapubic tenderness, and the bladder may be palpable.
Management
Urethral catheterization is both diagnostic and therapeutic. 11 Initial catheterization is often attempted with a 16-French Foley catheter. If the patient is a male with a known history of an enlarged prostate or difficult catheterization in the past, an 18-French coude catheter is also a reasonable first choice. The catheter may be left in place until an appropriate evaluation in a clinical setting.
In extreme circumstances, such as failed catheterization attempts or concern for urethral trauma (blood at urethral meatus), a suprapubic bladder aspiration should be considered. Careful attention must be paid to abdominal surgical history because this may alter the patient’s abdominal and pelvic anatomy. Suprapubic aspiration is ideally performed with ultrasound for identification of the hollow fluid-filled bladder and instrument guidance (Figures 2 and 3).
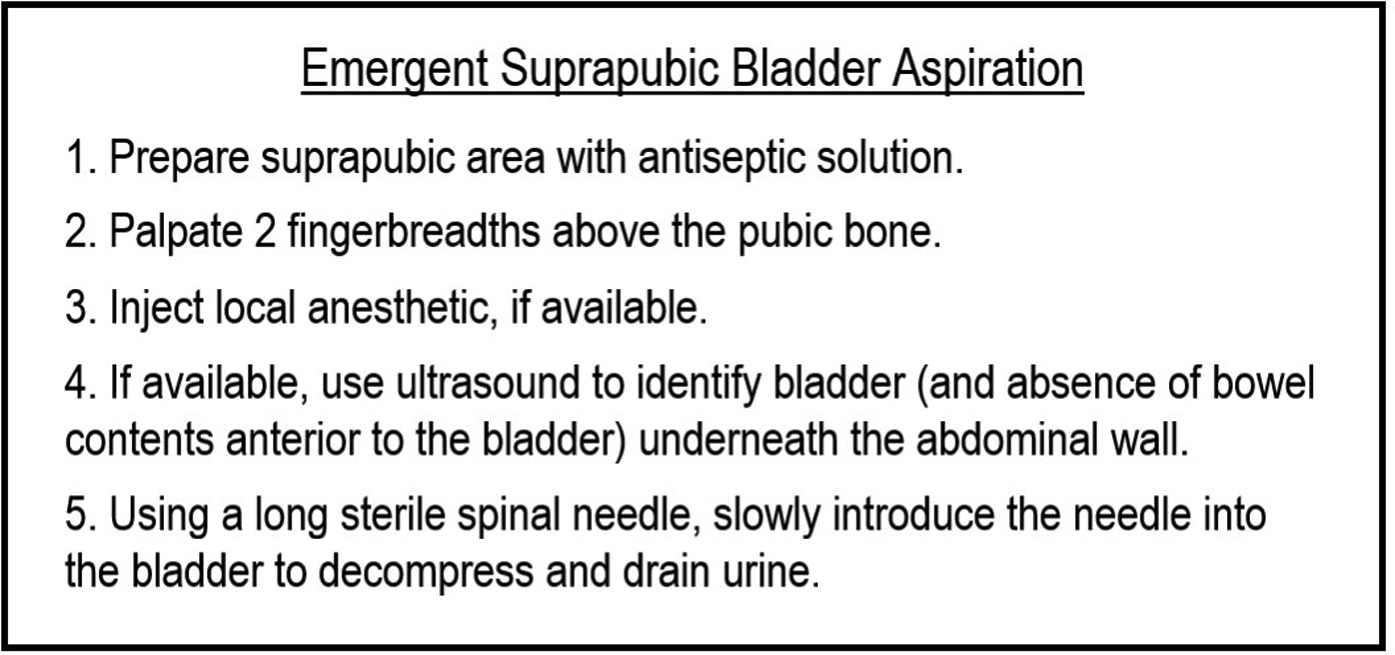
Suprapubic aspiration technique. Stepwise technique for urgent urinary aspiration.
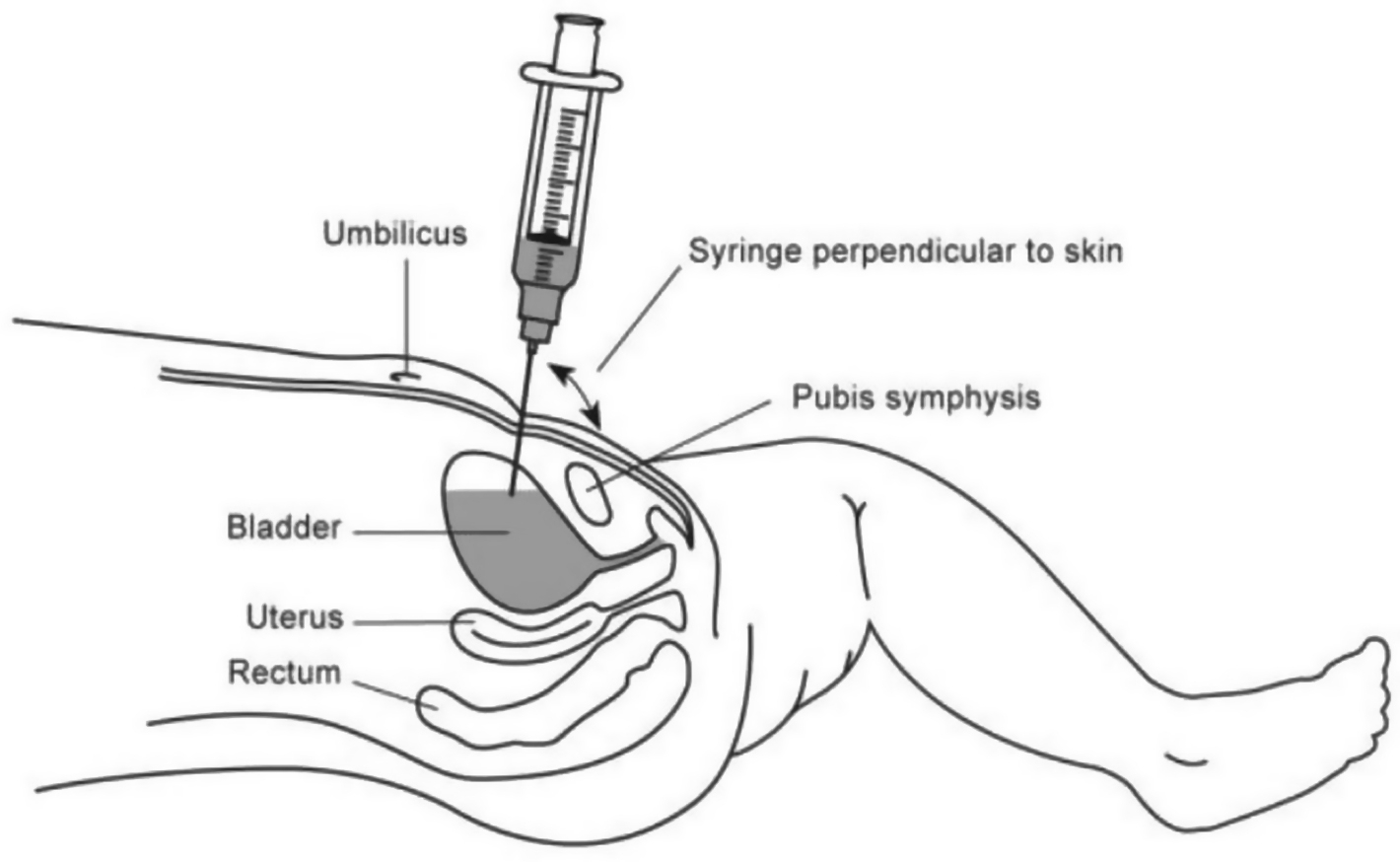
Urinary aspiration diagram. Reprinted with permission from Government of Western Australia Child and Adolescent Health Service.
Indications for evacuation
Inability to catheterize a patient in acute urinary retention should prompt evacuation to a medical facility capable of performing a complicated urethral or suprapubic catheterization.
Renal Colic and Urolithiasis
Kidney stone disease is growing in prevalence in the US population. 12 Exposure to excessive heat and conditions that promote dehydration have been associated with an increased risk of stone formation.13,14 Nonobstructing kidney stones themselves are not a cause for concern. However, should a stone cause urinary obstruction, this may rapidly become an acute issue.
Presentation
The classic presentation is characterized by acute, colicky flank pain. As the stone traverses the ureter, the pain distribution may change and refer to the lower abdominal quadrant or radiate to the ipsilateral groin or scrotum. Patients may also experience urinary urgency/frequency, abdominal pain, or hematuria.
Evaluation
A detailed history may reveal risk factors associated with stone formation, such as poor oral fluid intake, history of stones, family history of stone disease, inflammatory bowel disease or previous bowel surgery, gout, type II diabetes, or hyperthyroidism. Physical examination findings typically demonstrate a distressed patient unable to rest comfortably, costovertebral angle tenderness, and occasional mild unilateral abdominal pain to deep palpation. It is important to note that these symptoms mimic many other nonurologic acute abdominal and pelvic conditions. A simple and rapid urine dipstick test can be used to identify red blood cells, a nonspecific marker of potential urolithiasis. Using this information, a simplified risk calculator, the STONE score, can be used to predict the presence of a ureteral stone as compared to another etiology (Table 1). 15
STONE Score
Low risk: 0–5. Moderate risk: 6–9. High risk: 10–13. 15
If available, a portable ultrasound used by an experienced technician can supplement the workup to evaluate for hydronephrosis (swelling of renal collecting system); however, this modality will miss many ureteral stones. 16
Management
Medical management or surveillance of stone disease in the field is reasonable when there is acceptable pain control, absence of infectious symptoms (fever, malaise), ability to take in adequate oral fluids, and no history of underlying renal dysfunction. The fundamental components of medical management in the field consist of medical expulsive therapy. This consists of hydration with >2 to 3 L of fluid per day and pain control with oral nonsteroidal anti-inflammatory drugs. If available, a ureteral smooth muscle relaxant, such as tamsulosin (0.4 mg oral daily), can be used to assist in stone passage; this is most effective for small stones measuring <6 to 7 mm. 17 This medication should be used with caution because it can cause side effects of importance to those in remote or technically challenging areas: dizziness, orthostatic hypotension, syncope, and somnolence.
Indications for evacuation
Indications include suspicion of urinary obstruction along with signs of infection (eg, fever), inability to tolerate oral intake secondary to nausea/emesis, severe pain uncontrolled by oral analgesics, and lack of improvement with medical expulsive therapy. The imaging modality of choice to evaluate acute flank and suspicion of urinary stone disease remains noncontrast computed tomography, which is available at most hospitals.
Penile and Testicular Injury
Injury to the major urologic organs, such as the kidneys, ureters, and bladder, is generally seen in association with major, multiorgan trauma. Evaluation of the genitourinary system after a significant traumatic incident is best performed at a medical center with experienced trauma physicians. In contrast, the external male genitalia may be injured in isolation during traumatic episodes.
Presentation
Genital injuries include a heterogenous group of conditions secondary to blunt and penetrating trauma, amputation, bites, burns, and avulsions. The genitals are a hypervascular part of the human body, often with multiple sources of arterial flow, and such injuries are often accompanied by hemorrhage. Blunt trauma to the scrotum/testicles may result in significant scrotal swelling. Difficulty with urination may be a side effect of external genital trauma and cause pelvic pain and a palpable distended bladder.
Evaluation
In any traumatic event, primary focus should be adherent to the prehospital trauma life support trauma assessment protocol. 18 If an injury to the external genitalia is recognized, a full physical examination including penis, urethral meatus, scrotum, bilateral testicles, lower abdomen, and perineum should be part of the physical examination. Laboratory evaluation in the field can include a urine dipstick analysis to determine the presence of hematuria (Tables 2 and 3).
Scrotum injury grade
Adapted from American Association for Surgery of Trauma Injury Scoring Scale. 41
Penis injury grade
Adapted from American Association for Surgery of Trauma Injury Scoring. 41
Management
All wounds, lacerations, and abrasions should be copiously irrigated and washed to remove contamination in a timely manner. Superficial wounds caused by animal bites should not be closed, and affected individuals should receive appropriate antibiotics in accordance with local resistance patterns (eg, penicillin/beta lactamase inhibitor, cephalosporin).
Simple, small, clean penile lacerations (grade I) that involve only the superficial skin without damage to the underlying fascial layer may be closed primarily with aseptic technique. More severe penile injuries should not be closed primarily in the field. Penetrating penile injuries may be associated with concomitant urethral injuries in 11 to 29% of cases. 19 As such, a urethral catheter should not be placed if there is blood at the urethral meatus, a high-riding prostate on rectal examination, a penile hematoma, or suspicion of urethral injury. Instead, consideration should be given to placement of a suprapubic tube.
In the rare instance of a penile amputation (grade IV/V), direct pressure should be applied, rather than use of the tourniquet technique, and the amputated penis should be transported with the patient. The amputated penis should be wrapped in sterile dressing, placed in a plastic bag, and placed in a container with ice. 20 The amputated penis may be reconstructed with good urinary and sexual outcomes, although this requires multidisciplinary expertise. 21
Blunt scrotal trauma may lead to rupture of the testicle in 50% of cases. 22 These patients should be transported to a medical center to undergo either an initial ultrasound evaluation or direct operative exploration.
Indications for evacuation
All cases of penile or testicular trauma should ideally be evaluated at a medical center with a qualified urologist. Injuries with a high-velocity mechanism or concern for intra-abdominal or retroperitoneal insult with hematuria on dipstick should be evacuated for radiologic evaluation at a medical center.
Testicular Torsion
Testicular torsion occurs when the testes twist on their blood supply, thereby compromising arterial flow and resulting in ischemia. This is due to a congenital anomaly (bell clapper deformity) that allows the testicles to freely rotate on the spermatic cord within the scrotum.
Presentation
Torsion is most common in young males (<25 y of age) and is found more commonly on the left side. Patients often report acute-onset, severe unilateral testicular pain and accompanying nausea and vomiting. Torsion often occurs after vigorous activity and may be more common in low-temperature and low-humidity environments. 23
Evaluation
Classic physical examination features include an absent cremasteric reflex, testicular swelling, tenderness to palpation, and a high-lying, horizontal testicle. The cremaster reflex is tested by lightly stroking the superior and medial aspect of the thigh in a downward direction. Many of these findings may be inconclusive. Ultrasound has been proposed as an increasingly available tool in the austere environment. 24 If Doppler ultrasound is available, decreased or absent arterial flow is demonstrated within the testicle. Without imaging, the TWIST score may be considered. This is a validated clinical scoring system used in the setting of suspected testicular torsion (Table 4). 25
TWIST Score
Low risk: 0–2. Intermediate risk: 3–4. High risk: 5–7. 25
Management
Surgical exploration is mandatory to assess the viability of the testis and to re-establish testicular blood flow. If a hospital with trained surgeons is not available, manual detorsion can occasionally be successful. This is performed by externally rotating the affected testicle. This maneuver is colloquially called an “open book” detorsion because the testicle should be rotated externally from medial to lateral as if one was opening a book. Even if manual detorsion is successful, the patient should still be referred promptly to a urologist for orchidopexy when possible.
Indications for evacuation
Immediate evacuation to a medical center for evaluation and treatment is of utmost importance. Salvage rates approach 100% in patients who undergo detorsion within 6 h from the start of pain. The longer the delay in treatment, the worse the outcome for testicular viability. 26
Paraphimosis
Paraphimosis occurs in uncircumcised males when the foreskin or prepuce becomes fixed behind the coronal ridge of the glans penis. This condition is most often iatrogenic after urinary tract instrumentation; however, other causes have been reported in the literature that may be of importance to the outdoorsman (eg, Plasmodium falciparum infection 27 ) or those working in resource-poor areas.
Presentation
The foreskin of the uncircumcised or partially circumcised male is retracted behind the glans penis and unable to be reduced. This may result in venous and lymphatic obstruction, characterized by pain, swelling, and discoloration. Delayed treatment can lead to gangrene and tissue necrosis.
Evaluation
A targeted history should be undertaken and the penis should be handled with care because it is often edematous and swollen.
Management
Attempts to reduce the paraphimosis should be made in a timely manner to reduce the risk of progression to infection and tissue necrosis. Several conservative measures are reported in the literature.
28
In the field, an initial attempt can include the following algorithm. Patients often benefit from oral and/or topical pain control if available. Reduction of swelling Manual compression: Circumferential firm pressure using a gloved hand to the distal penis for several minutes, in an attempt to reduce tissue edema. This may allow for reduction of the foreskin. Ice: Half-fill a rubber glove with ice and water and tie a knot in the cuff to secure the contents. Place the edematous glans penis into the invaginated thumb of the glove for 5 min.
29
Compression wrap: Use an approximately 2-inch elastic bandage wrapped around the penis starting at the glans. IMPORTANT: remove in 5 to 7 min to avoid ischemia.
30
Reduction of foreskin Place both thumbs on the distal glans. Use both forefingers and middle fingers on the proximal aspect of the constricting foreskin to apply countertraction. Press firmly with thumbs and pull with fingers to reduce constricting band over the entire glans.
Indications for evacuation
Failure of conservative measures or clinical signs of ischemia or infected tissue should prompt evacuation to a medical center for possible surgical (ie, dorsal slit or circumcision) or advanced pharmacologic intervention. Successful reduction of paraphimosis does not need to be evacuated. All patients should be referred to a urologist in the future for discussion of potential elective circumcision.
Priapism
Priapism is a rare condition; however, it remains one of the few true urologic emergencies and therefore requires prompt evaluation and emergency management to avoid permanent damage to the penis. Two main forms of priapism exist: ischemic and nonischemic. Ischemic priapism represents a compartment syndrome. Priapism is a persistent erection characterized by little or no cavernosal arterial blood flow and is tender to palpation. Nonischemic priapism is caused by unregulated arterial inflow, and the penis is typically neither fully rigid nor painful. Priapism has been linked to envenomation from such remote fauna as Brazilian wandering spiders, 31 widow spiders, 32 and scorpion stings. 33
Presentation
Priapism presents as an erect penis of greater than 4 h duration. 34 In these cases, the erect penis either persists long after sexual stimulation or is completely unrelated to stimulation. Pain may be reported but is not required for diagnosis. In some cases, nonischemic priapism can develop after blunt perineal trauma.
Evaluation
A thorough history should be taken, including the duration of erection, degree of pain, history of priapism, history of pelvic/genitourinary trauma, spinal cord injury, history of hematologic abnormality (eg, sickle cell disease, leukemia), or recent envenomation by black widow spider or scorpion. 35 History should also include medications known to cause priapism, including antihypertensives, antidepressants/psychoactive drugs, alcohol, and illicit recreational drugs. Physical examination should include the genitalia, perineum, and abdomen.
Management
The ultimate goal of priapism management is detumescence with the preservation of erectile function. Initial management is to determine the etiology of the priapism, which requires laboratory blood analysis. Oral systemic therapy is not indicated for the treatment of priapism. 34 If transport to a medical facility is expected to take significantly longer than 4 h, trained providers may make an initial attempt at therapeutic aspiration using aseptic placement of a needle into the cavernosal bodies at 3 o’clock and 9 o’clock in the penile shaft. In the exceedingly rare case of priapism secondary to envenomation by black widow spiders, small unvalidated reports show improvement of priapism management when L mactans antivenom is incorporated into treatment algorithm. 36
Indications for evacuation
Essentially, all cases of priapism should be evacuated to a medical center that is capable of evaluating and managing this condition. The risks of attempting oral medications or cavernosal aspiration in the field outweigh the benefits of treatment in a controlled setting.
Wilderness Toxicology and Urologic Conditions
Acute Kidney Injury and Renal Failure
Myriad etiologies of acute kidney injury and renal failure from naturally occurring substances, wildlife envenomation, and exposures during natural disasters exist. A full evaluation of these causes and treatments is beyond the scope of this review; however, it remains an important consideration in the evaluation of patients in resource-poor environments. We recommend that healthcare providers operating in these environments tailor their evaluation of patients who have undergone an insult or injury to their particular circumstances and be familiar with potential sequelae of insults that could lead to a significant renal injury requiring rapid evacuation to a hospital center. For example, in tropical countries, snake bite-induced acute kidney injury is a significant health issue that can result in renal failure and the need for hemodialysis. 37 In a different context, natural and manmade disasters can result in the dissemination of chemicals into the environment that are harmful to the genitourinary system either directly or indirectly. Such toxins include organophosphates (eg, in pesticides, chemical warfare agents), components of rodent killers, and industrial compounds. 38
Urinary Tract Infections
Urinary tract infections (UTIs) are a common pathologic condition and remain one of the most common indications for prescription of antimicrobials in otherwise healthy individuals. The diagnosis of a UTI requires both the presence of signs/symptoms and a positive urine culture. However, because urine cultures can be difficult to obtain without available resources, it is necessary to recognize the signs, symptoms, and urinalysis results that suggest a UTI.
Uncomplicated versus complicated
An uncomplicated infection is characterized by any UTI in an adult female. A “complicated” UTI includes any person who is immunosuppressed, pregnant, male, or a pediatric patient. In addition, any patient with urinary obstruction (ie, ureteral calculus, urinary retention with UTI sequelae) is considered to have a complicated UTI. Lastly, patients with fever, flank pain, or inability to tolerate oral fluids should raise suspicion for a complicated UTI.
Signs and symptoms
Acute bacterial cystitis is characterized by dysuria, frequency, urgency, fever, suprapubic discomfort, and foul-smelling urine. Pyelonephritis often includes the symptoms of acute cystitis plus flank pain, GI symptoms, and fever. On examination, patients with pyelonephritis may have costovertebral angle tenderness.
Urinalysis testing
A simple and effective tool for evaluating for the presence of a urinary infection is urinalysis. Understanding test results may help in making an accurate diagnostic decision. Pyuria is defined as the presence of >5 white blood cells per high-powered field in centrifuged urine and is a helpful surrogate marker of infection. The presence of nitrites can be also be used as a surrogate marker for an infection because some bacteria contain enzymes that produce nitrites in urine.
Treatment
Patients with uncomplicated acute bacterial cystitis and mildly ill patients with uncomplicated pyelonephritis may be treated with oral antibiotics. Patients who have fevers, nausea/vomiting, or other hemodynamic instability should be evacuated to a hospital setting for intravenous antibiotics and supportive care. After beginning antibiotics, patients with uncomplicated pyelonephritis are generally afebrile within 72 h; fevers beyond this time are suggestive of a more complicated and serious infection and should be investigated appropriately (ie, with imaging).
Antimicrobial choice
The most common bacterial pathogen causing a UTI is Escherichia coli. Patient allergies should be taken into account. The Infectious Disease Society of America recommends the following options as first line for uncomplicated cystitis UTI.
39
Treatment for pyelonephritis is an extended course of antibiotics (eg, 14 d of trimethoprim-sulfamethoxazole), which should not include nitrofurantoin because it does not reach adequate tissue penetration.
40
Nitrofurantoin monohydrate/macrocrystals 100 mg BID × 5 d (although it has poor tissue penetration). Trimethoprim-sulfamethoxazole 160/800 mg BID × 3 d Fosfomycin trometamol 3 mg single dose
Recommended medications and urologic supplies to be included in emergency kit
Nonsteroidal anti-inflammatory drugs (eg, ibuprofen, naproxen) Two Foley urethral catheters: 16 French, 18 French coude Antibiotics (trimethoprim-sulfamethoxazole 160/800 mg, fosfomycin trometamol 3 g) Urine dipstick testing kit
Conclusions
This review addresses common urologic conditions that a healthcare provider may encounter in a wilderness or austere environment. Ultimately, when unclear about the patient condition or concerned about lack of improvement, we recommend evacuation for urologic evaluation. In addition, patients who experience any of these conditions in an austere environment, even if treated by local medics, should establish follow-up with a local urologist as soon as possible for further management and evaluation.
There are likely urologic conditions and diseases that providers have encountered in resource-poor settings that are not published in the literature and for which novel management strategies have been employed. Many of these conditions are doubtlessly successfully treated on a regular basis by providers without dedicated urologic training. However, we hope this review written from a urology perspective encourages a collaborative multidisciplinary approach toward the development of a dynamic educational reference resource in the medical community that serves those in a wilderness, austere, or resource-poor setting.
Footnotes
Acknowledgements
Author Contributions: Concept and design (MJM, MDM); acquisition of data (MJM, MDM); drafting of manuscript (MJM, MDM); critical revision of manuscript (MJM, MDM); approval of final manuscript (MJM, MDM)
Financial/Material Support: None.
Disclosures: None.